#FITSurvivalGuide #ACCFIT
Topic - Ventricular Tachycardia!
Agenda:
1- Approach to evaluating #VT
2- Management of #VT
3- Practice Cases
Please share your thoughts & input to this #tweetorial!
@ACCCardioEd @ACCinTouch #FOAMed @MichiganACC
Topic - Ventricular Tachycardia!
Agenda:
1- Approach to evaluating #VT
2- Management of #VT
3- Practice Cases
Please share your thoughts & input to this #tweetorial!
@ACCCardioEd @ACCinTouch #FOAMed @MichiganACC
#FITSurvivalGuide #ACCFIT
1/10 – Ventricular Tachycardia
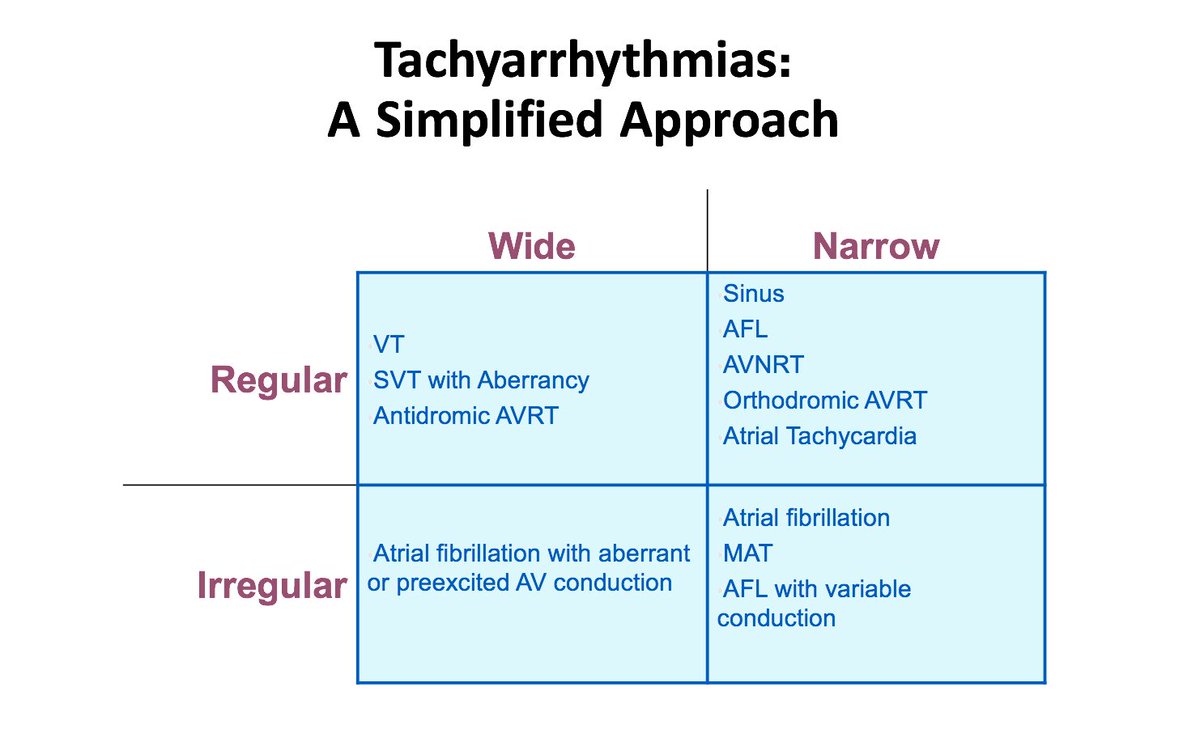
Simplified approach to evaluate tachycardia:
Rule #1 – If HD unstable ➡️ shock!
If HD stable, sit down & think.
Step # 1 - QRS: wide or narrow?
Step # 2 - Rhythm: regular or irregular?
This will narrow DDx!
1/10 – Ventricular Tachycardia
Simplified approach to evaluate tachycardia:
Rule #1 – If HD unstable ➡️ shock!
If HD stable, sit down & think.
Step # 1 - QRS: wide or narrow?
Step # 2 - Rhythm: regular or irregular?
This will narrow DDx!
#FITSurvivalGuide #ACCFIT
2/10 - Wide complex tachycardia
Always consider clinical Scenario!
Look for history of MI and cardiomyopathy ➡️ strongly favor #VT!
* If structural heart disease is present, you will be correct 9/10 times with diagnosis of VT!
2/10 - Wide complex tachycardia
Always consider clinical Scenario!
Look for history of MI and cardiomyopathy ➡️ strongly favor #VT!
* If structural heart disease is present, you will be correct 9/10 times with diagnosis of VT!


#FITSurvivalGuide #ACCFIT
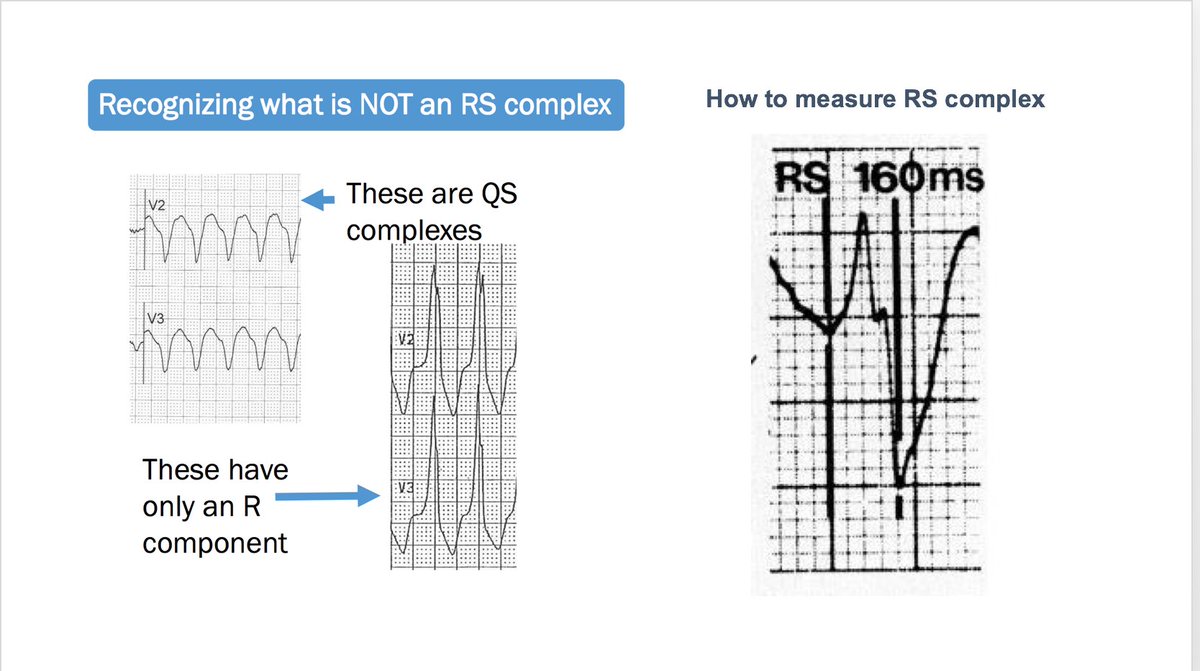
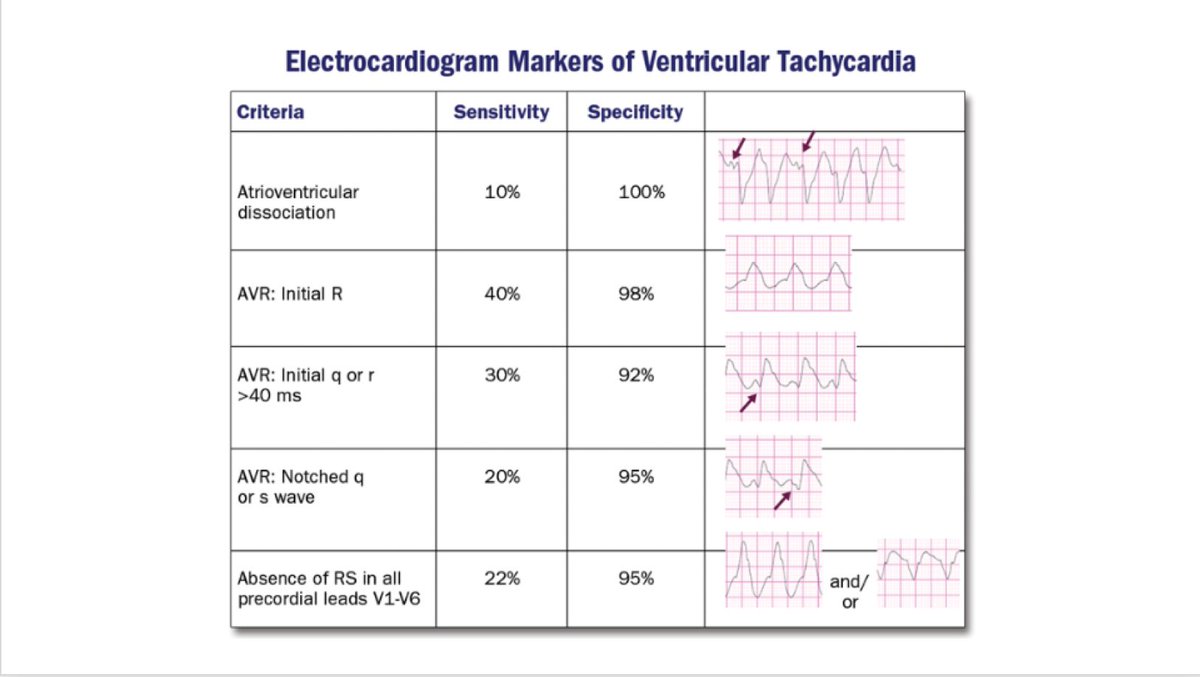
4/10 – VT from SVT (Brugada Criteria)
Q1) RS absent in precordial leads? If YES, it’s #VT!
Q2) If present, is RS interval > 100ms? If YES, it’s #VT!
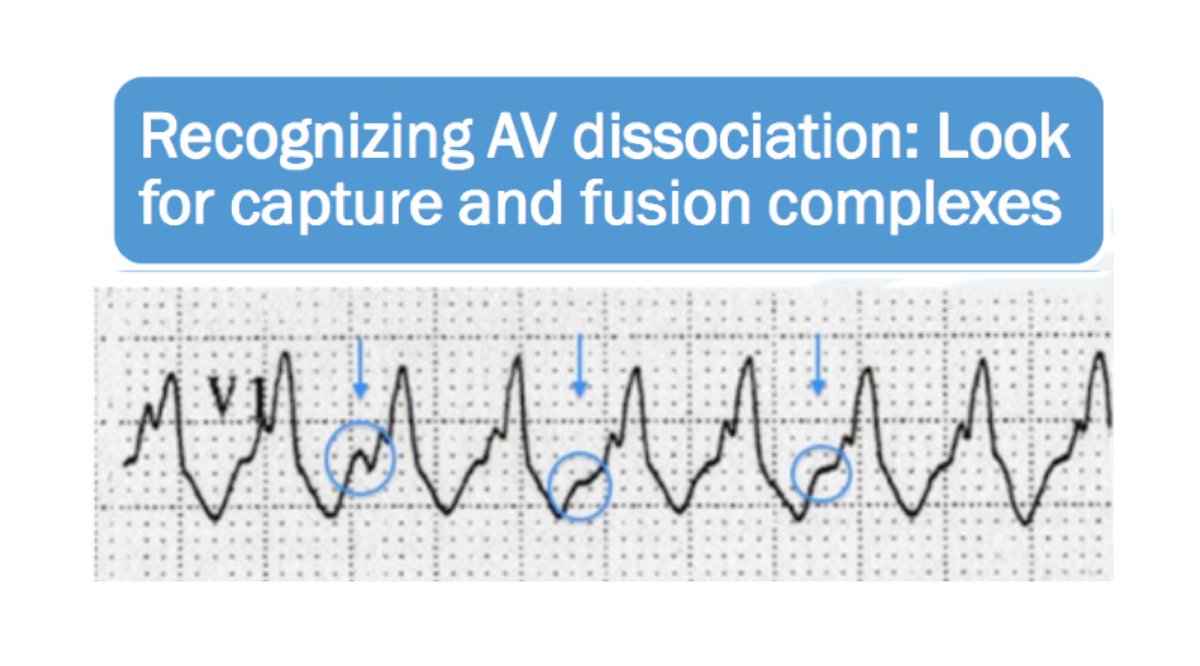
Q3) If Q1 & 2 are NO, any AV dissociation? If YES, it’s #VT!
If all Qs are NO, then ✔️QRS morphology
4/10 – VT from SVT (Brugada Criteria)
Q1) RS absent in precordial leads? If YES, it’s #VT!
Q2) If present, is RS interval > 100ms? If YES, it’s #VT!
Q3) If Q1 & 2 are NO, any AV dissociation? If YES, it’s #VT!
If all Qs are NO, then ✔️QRS morphology
#FITSurvivalGuide #ACCFIT
5/10 – VT from SVT continued...
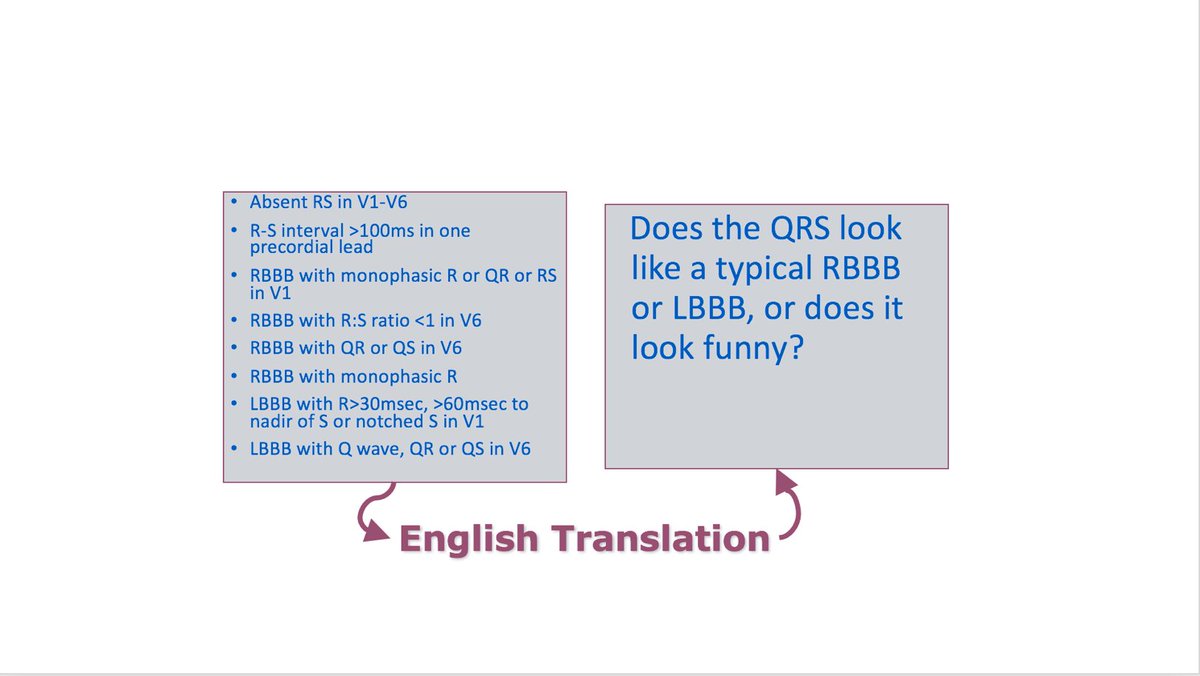
If prior 3 Qs are NO ➡️ check QRS morphology
Q4) Does QRS appear like a typical RBBB or LBBB, or does it look funny?
If funny looking, likely #VT!
Specific criteria for #VT by QRS morphology (extensive, see figure)
5/10 – VT from SVT continued...
If prior 3 Qs are NO ➡️ check QRS morphology
Q4) Does QRS appear like a typical RBBB or LBBB, or does it look funny?
If funny looking, likely #VT!
Specific criteria for #VT by QRS morphology (extensive, see figure)
#FITSurvivalGuide #ACCFIT
6/10 – Other useful #ECG findings suggestive of VT:
-Axis - Extreme AD (“northwest axis”) — QRS + in aVR & - in I / aVF
-QRS width - Very broad (RBBB > 140 ms, LBBB >160 ms)
-Q waves – sign of CAD
-Josephson’s sign – Notching near nadir of the S-wave
6/10 – Other useful #ECG findings suggestive of VT:
-Axis - Extreme AD (“northwest axis”) — QRS + in aVR & - in I / aVF
-QRS width - Very broad (RBBB > 140 ms, LBBB >160 ms)
-Q waves – sign of CAD
-Josephson’s sign – Notching near nadir of the S-wave
#FITSurvivalGuide #ACCFIT
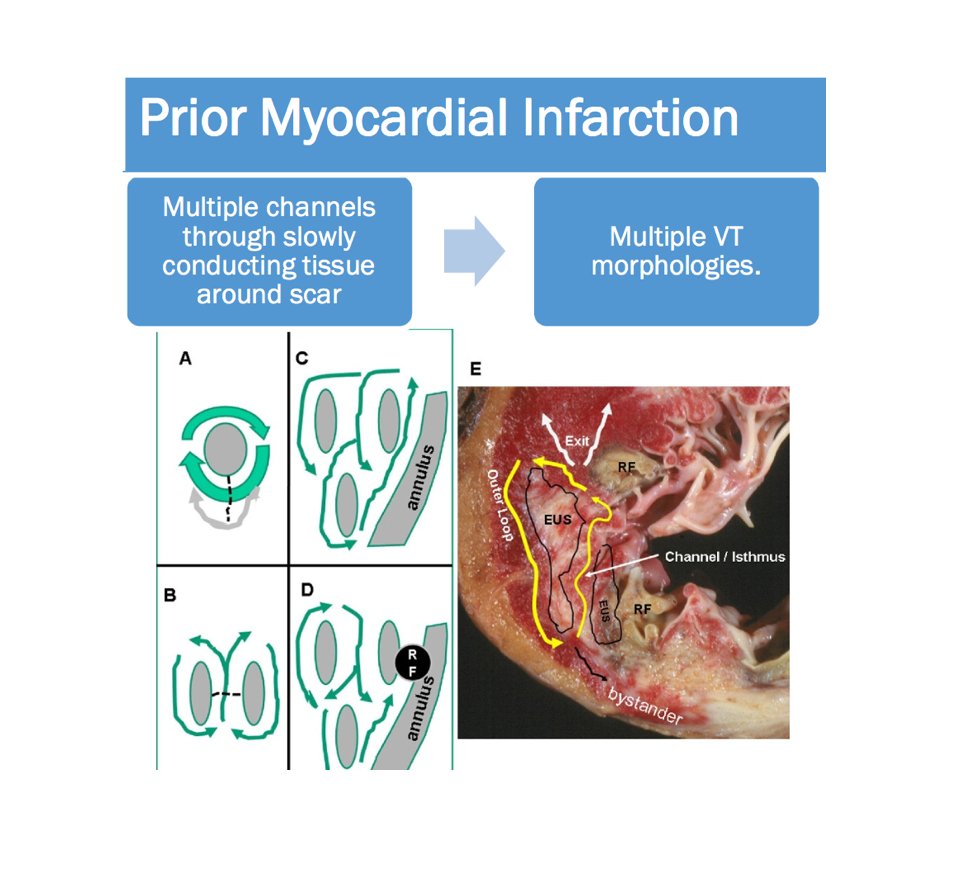
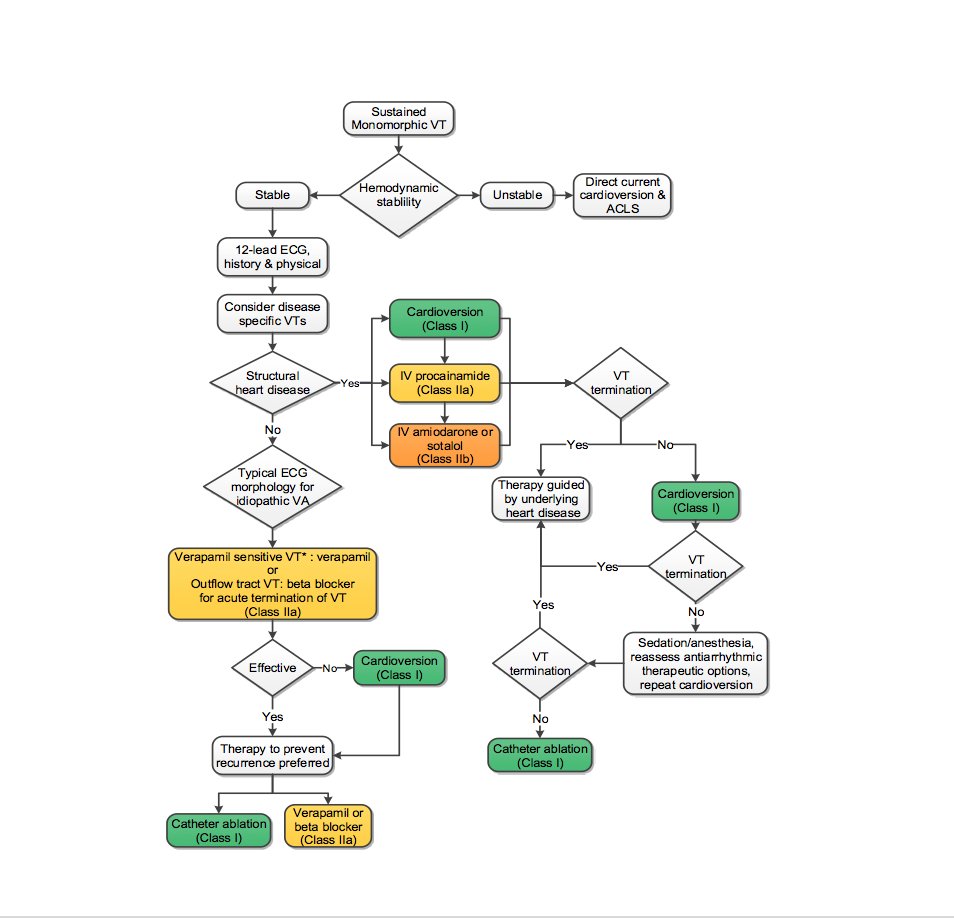
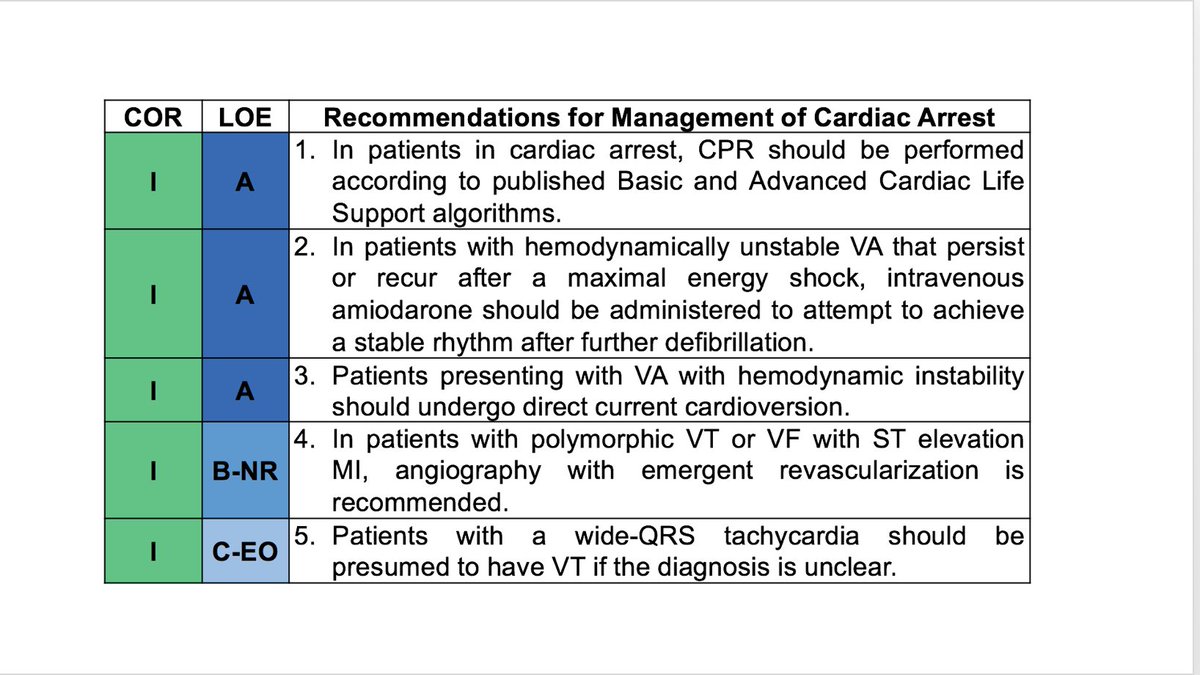
7/10 – Management of Monomorphic #VT
-Usually 2/2 reentry around scar
-Initial Tx – ACLS!
-Immediate cardioversion if unstable, or drugs don’t work!
-HD stable? Give amiodarone 150mg over 10 minutes followed by 1mg/min
-Evaluate underlying etiology!
7/10 – Management of Monomorphic #VT
-Usually 2/2 reentry around scar
-Initial Tx – ACLS!
-Immediate cardioversion if unstable, or drugs don’t work!
-HD stable? Give amiodarone 150mg over 10 minutes followed by 1mg/min
-Evaluate underlying etiology!
#FITSurvivalGuide #ACCFIT
8/10 – Long term #VT Tx:
-Assess SCD risk & ICD need
-Anti-arrhythmic Tx (amio, sotalol, mexiletine)
-Ablation in selected pts
-HF therapy
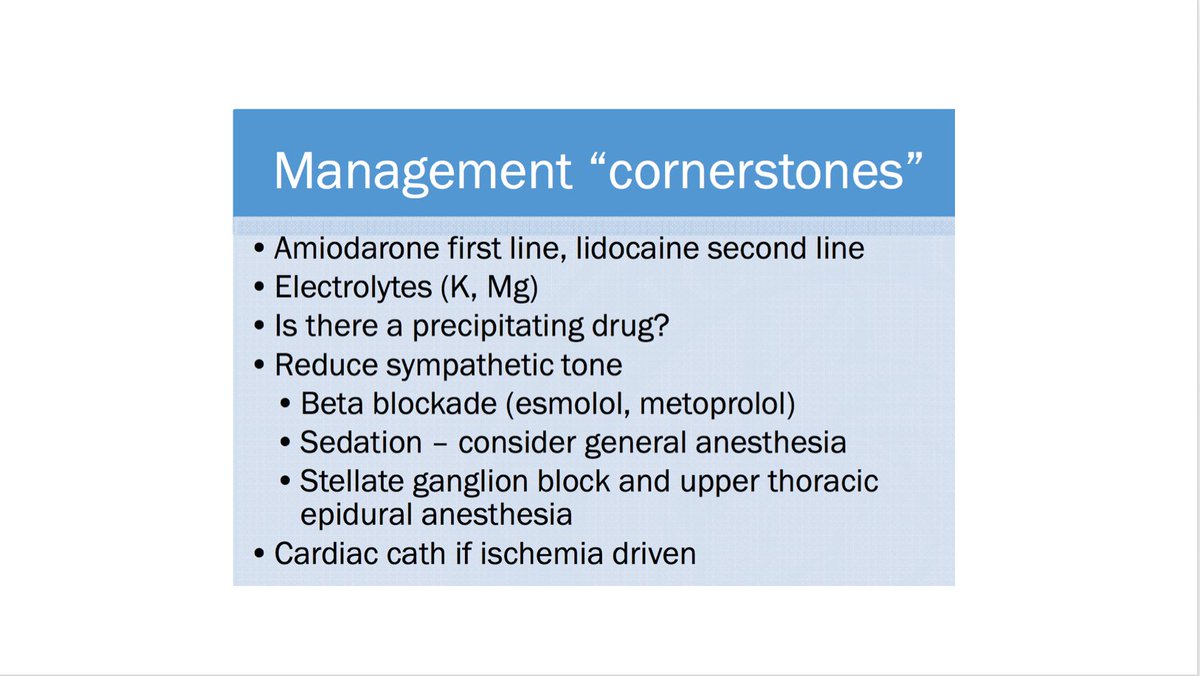
#VT Storm:
≥3 VT episodes/ 24 hrs
Can ☞ incessant state!
Tx - amio > lido, lytes, BB (see Tx “cornerstones”)
8/10 – Long term #VT Tx:
-Assess SCD risk & ICD need
-Anti-arrhythmic Tx (amio, sotalol, mexiletine)
-Ablation in selected pts
-HF therapy
#VT Storm:
≥3 VT episodes/ 24 hrs
Can ☞ incessant state!
Tx - amio > lido, lytes, BB (see Tx “cornerstones”)
#FITSurvivalGuide #ACCFIT
9/10 – Polymorphic VT/VF
Think ischemia!!!
#AMI ➡️ early cardiac cath!
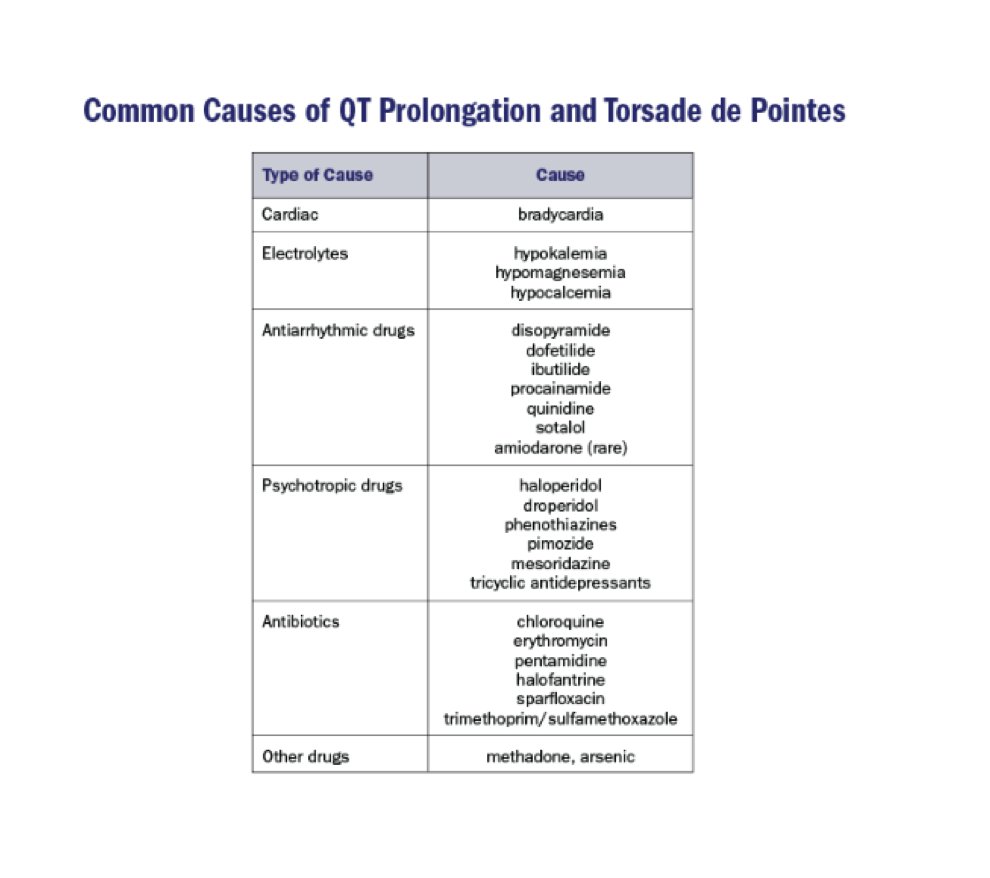
Other precipitating causes: Drugs (QT prolonging -- see figure), electrolytes, decompensated HF
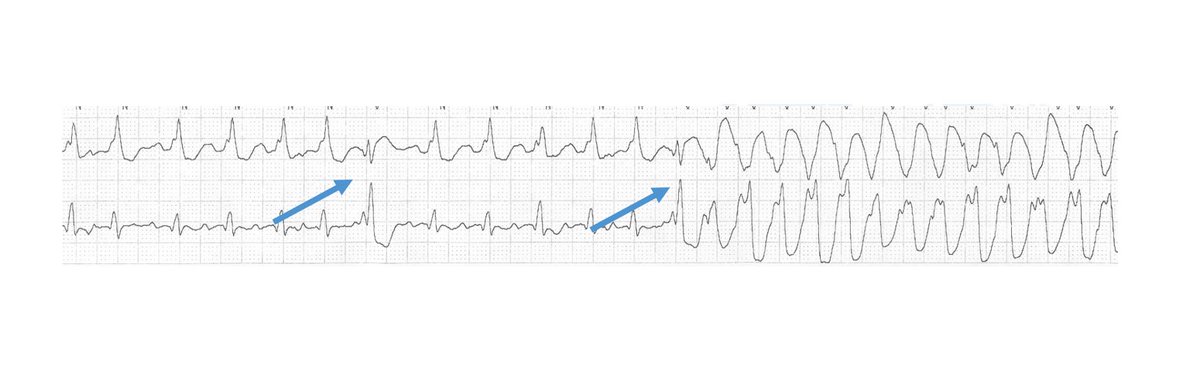
PVC may trigger polymorphic VT/VF; can be a target for ablation (see fig)
9/10 – Polymorphic VT/VF
Think ischemia!!!
#AMI ➡️ early cardiac cath!
Other precipitating causes: Drugs (QT prolonging -- see figure), electrolytes, decompensated HF
PVC may trigger polymorphic VT/VF; can be a target for ablation (see fig)
#FITSurvivalGuide #ACCFIT
10/10 Summary
If HD unstable ⇧ HR ⇒ shock!
✔️ Narrow vs wide QRS & rhythm regularity ➡️narrow DDx
✔️ Brugada criteria to 👀 VT vs SVT. If underlying SHD, 90% it’s VT!
Follow Tx discussed
Now a few 💪 practice cases! Plz share your thoughts!
10/10 Summary
If HD unstable ⇧ HR ⇒ shock!
✔️ Narrow vs wide QRS & rhythm regularity ➡️narrow DDx
✔️ Brugada criteria to 👀 VT vs SVT. If underlying SHD, 90% it’s VT!
Follow Tx discussed
Now a few 💪 practice cases! Plz share your thoughts!
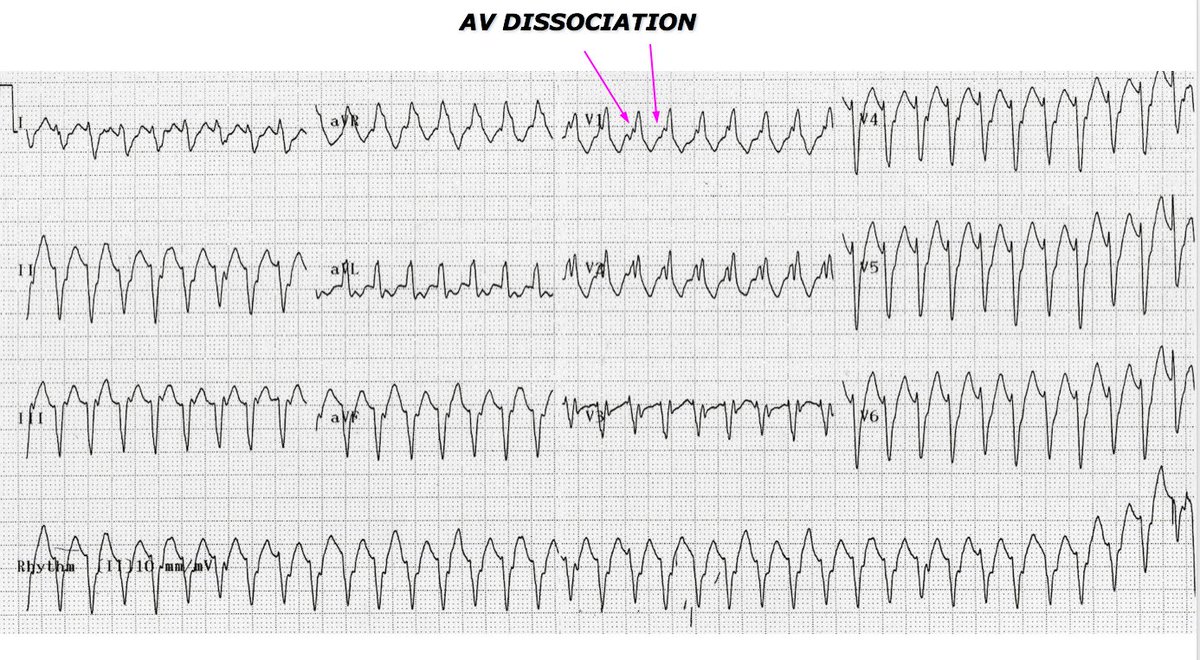
Case # 1 - 78 yo F s/p AVR presenting with palpitations.

ECG # 1 shows (answer to follow)
Case # 2 - 65 yo M presenting with palpitations/dizziness.

ECG # 2 shows (answer to follow)
Bonus Rhythm Strips

Rhythm Strips show:
Strong work! The majority got this correct. Close 👀 shows AV dissociation, with superimposed P waves visible in V1. Also, northwest axis & R/S ratio < 1 in V6 indicate that this is VT.

This was a bit tricky. The actual answer is C. Important lesson here is 👀 closely for irregularities in R-R interval ... as you'll notice towards the end of the rhythm strip this is actually irregular. The patient had post operative AF with aberrant conduction.

This was a tie! Correct answer is D. The top rhythm strip was in fact an artifact. If you trace the R-R intervals from start to end of rhythm strip, they actually march out as shown (complexes within artifact). 2nd strip was indeed Pres. Trump's Signature as shown in the image.