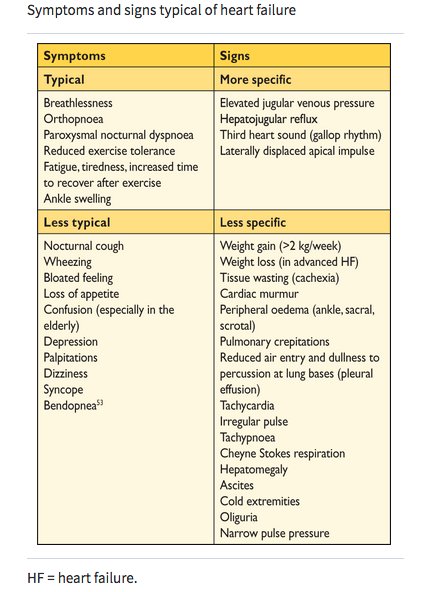
Heart Failure with Preserved Ejection Fraction #HFPEF Tweetorial! Once thought as just diastolic dysfunction, it is much more than that!
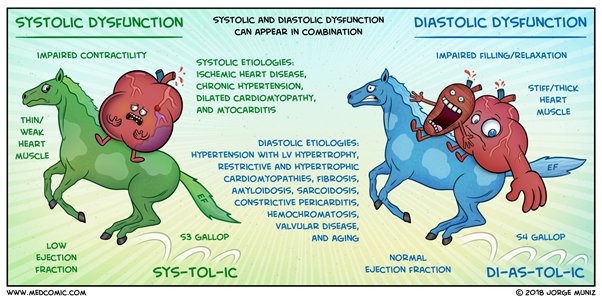
(picture credit @Medcomic) #HeartFailure #CardioEd
(picture credit @Medcomic) #HeartFailure #CardioEd
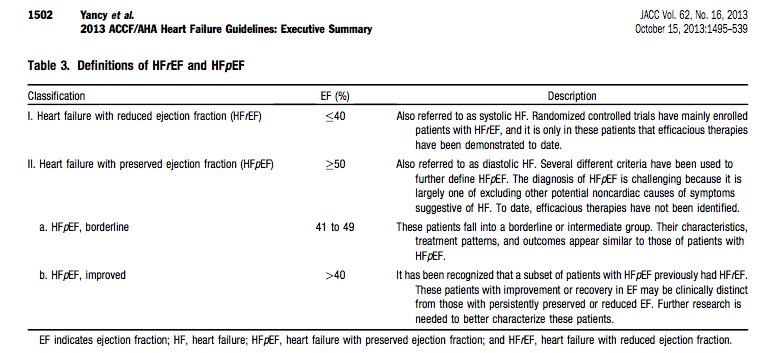
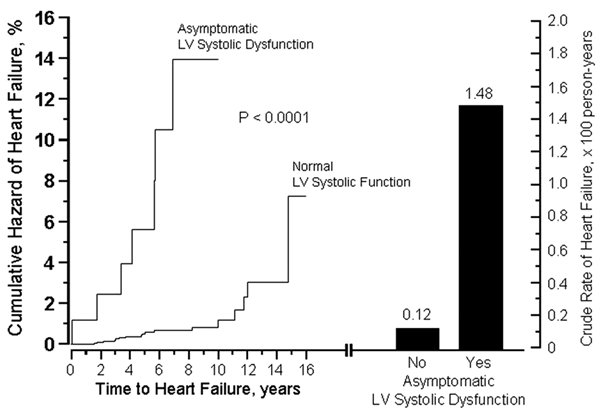
Why have we drawn a cut-off of 50% for rEF vs pEF? Well, this relates to older studies which showed that the risk of symptomatic heart failure increased significantly when your EF was less than 50%.
ahajournals.org/cgi/doi/10.116…
ahajournals.org/cgi/doi/10.116…
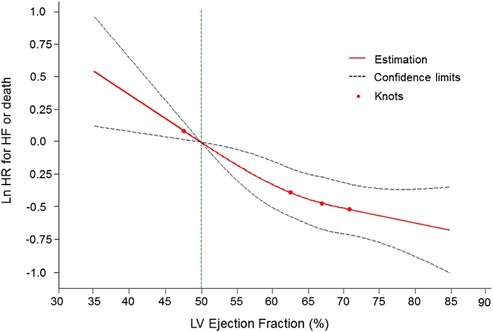
But is that still a relevant cut-off? Those with EF between 50 and 55% still have increased risk – and indeed EF has shown to correlate continuously with risk.
heartfailure.onlinejacc.org/content/4/6/502
heartfailure.onlinejacc.org/content/4/6/502
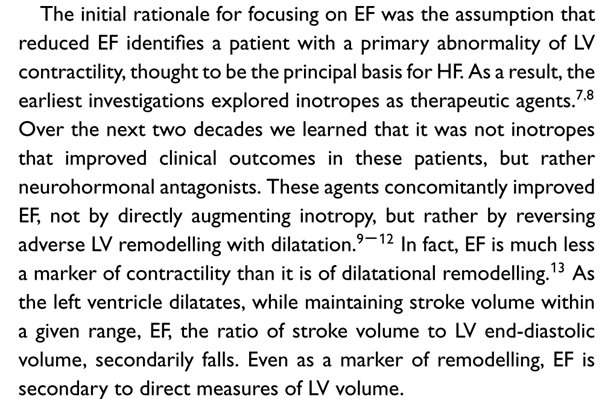
So we have to ask ourselves what a reduced ejection fraction is - @mkonstam puts it best: a reduced EF signifies dilational remodelling after an insult rather than a lack of contractility.
onlinelibrary.wiley.com/doi/abs/10.100…
onlinelibrary.wiley.com/doi/abs/10.100…
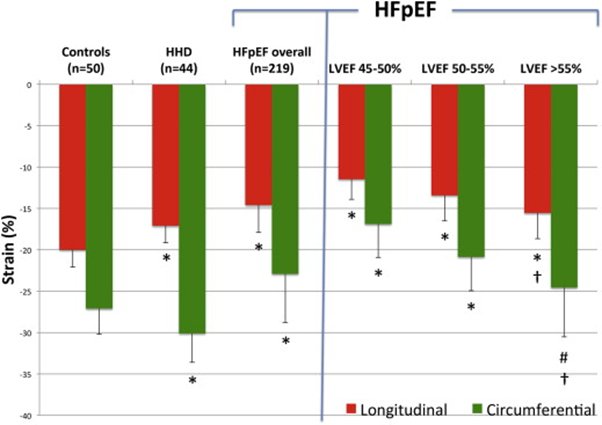
And we also know that EF lacks the subtlety to really discriminate impaired function: for instance, HFpEF has impaired strain values compared to healthy controls.
sciencedirect.com/science/articl…
sciencedirect.com/science/articl…
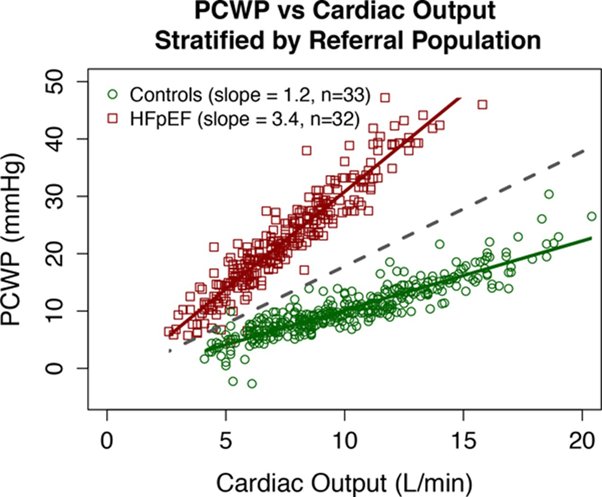
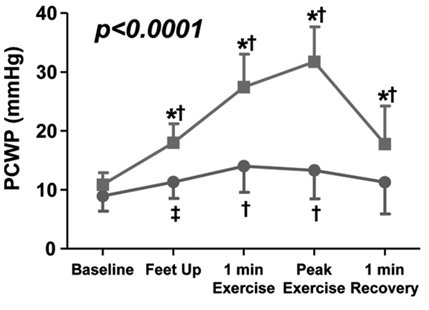
…not to mention showing impaired performance during exercise. Central to this seems to be an inability to deal with increased filling such as increased venous return on exertion.
ncbi.nlm.nih.gov/pubmed/29695381
ncbi.nlm.nih.gov/pubmed/29695381
While there is one common clinical phenotype, there are distinct pathologies at play which can broadly be divided into energetic dysfunction and cytoskeletal/extracellular rearrangement causing stiffening.
sciencedirect.com/science/articl…
sciencedirect.com/science/articl…
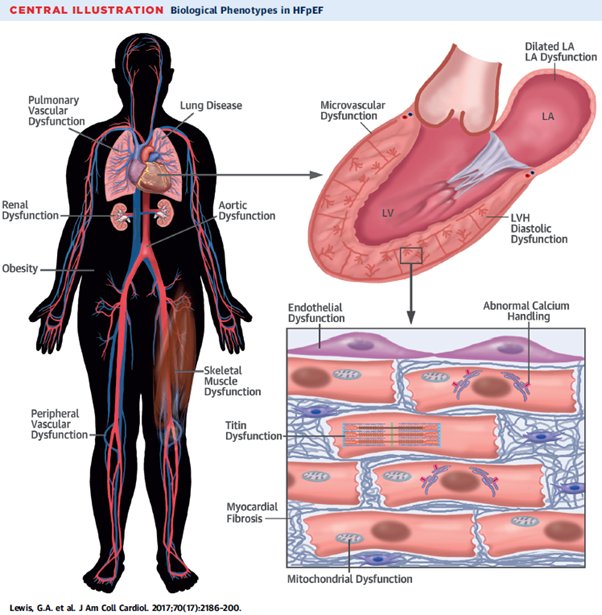
As cellular energy falls (for instance in insulin resistance), one of the first domains to be affected is the reuptake of calcium into the endoplasmic reticulum. This prolongs diastole and slows relaxation.
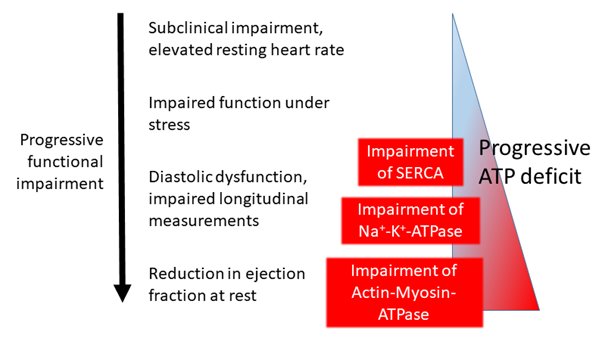
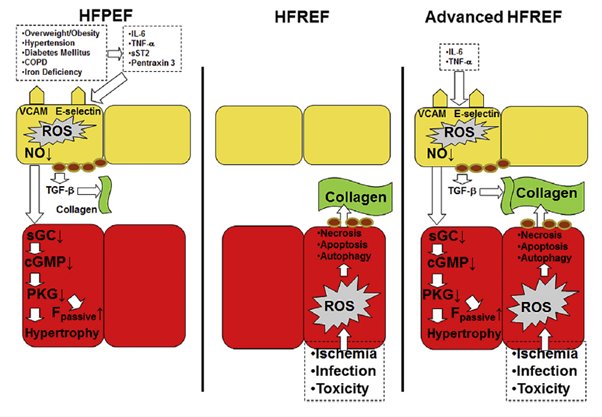
Meanwhile, various mechanisms (perhaps deriving from inflammation) lead to the development of cellular hypertrophy and fibrosis leading to mechanical stiffening. sciencedirect.com/science/articl…
The pathology and its interaction is not easy to understand!

But cluster studies on phenomapping allow us to tease out different groups: obese, diabetic patients with metabolic derangement falling on one side and hypertensive or older patients with stiffening falling on the other.
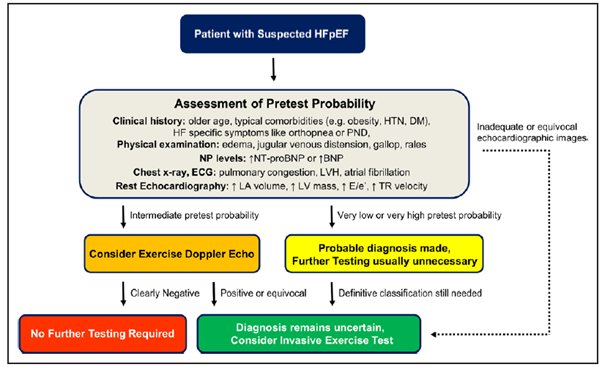
ESC guidelines allow us to make some headway into making diagnosis but are often criticised for their blunt approach.

In particular, looking at exercise related measurements (or even something as simple as a straight leg raise to give a volume load) needs to be taken into account as this can mask dysfunction. ncbi.nlm.nih.gov/pubmed/20543134
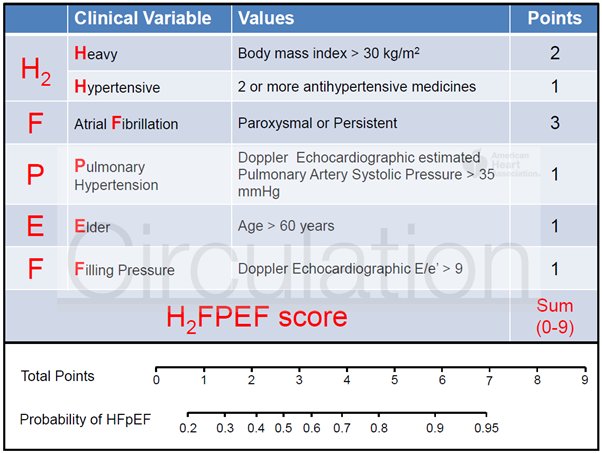
A clinical scoring system such as H2FPEF may help make a quick diagnosis ncbi.nlm.nih.gov/pubmed/29792299 @yreddyhf
Or a stepwise approach involving exercise testing and/or invasive measurements might help capture some patients at an early stage of disease who may otherwise be missed ncbi.nlm.nih.gov/pubmed/28039229
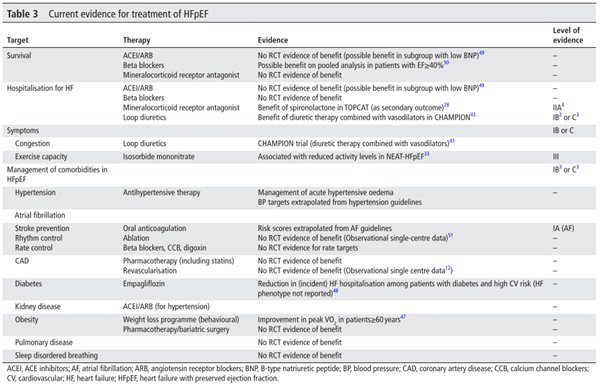
As for treatment, there has yet to be found a mortality reducing treatment but loop diuretics and spironolactone may reduce HF hospitalisation ncbi.nlm.nih.gov/pubmed/29305560 @RositaZakeri @ProfMartinCowie
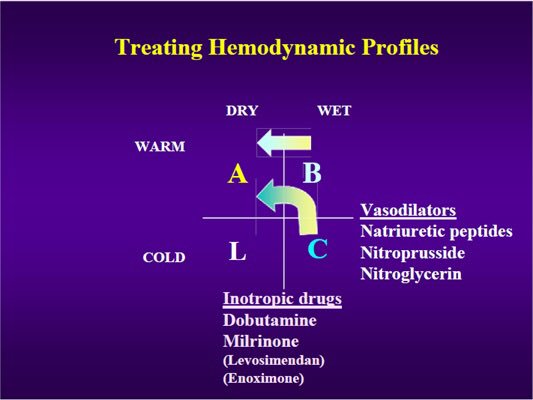
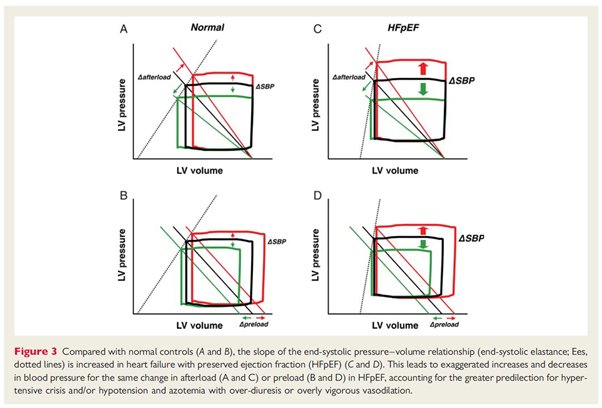
Why might this be? Well the relationship with pressure and volume in HFpEF is different to that in HFrEF, so vasodilation has much lesser effects.
academic.oup.com/eurheartj/arti…
academic.oup.com/eurheartj/arti…
Where does the future lie? Myocardial substrate modulation? Anti-fibrotic therapy? Tailored approaches for individual phenotypes is this author's feeling.
Thanks for reading!
Thanks for reading!