,
14 tweets,
9 min read
Read on Twitter
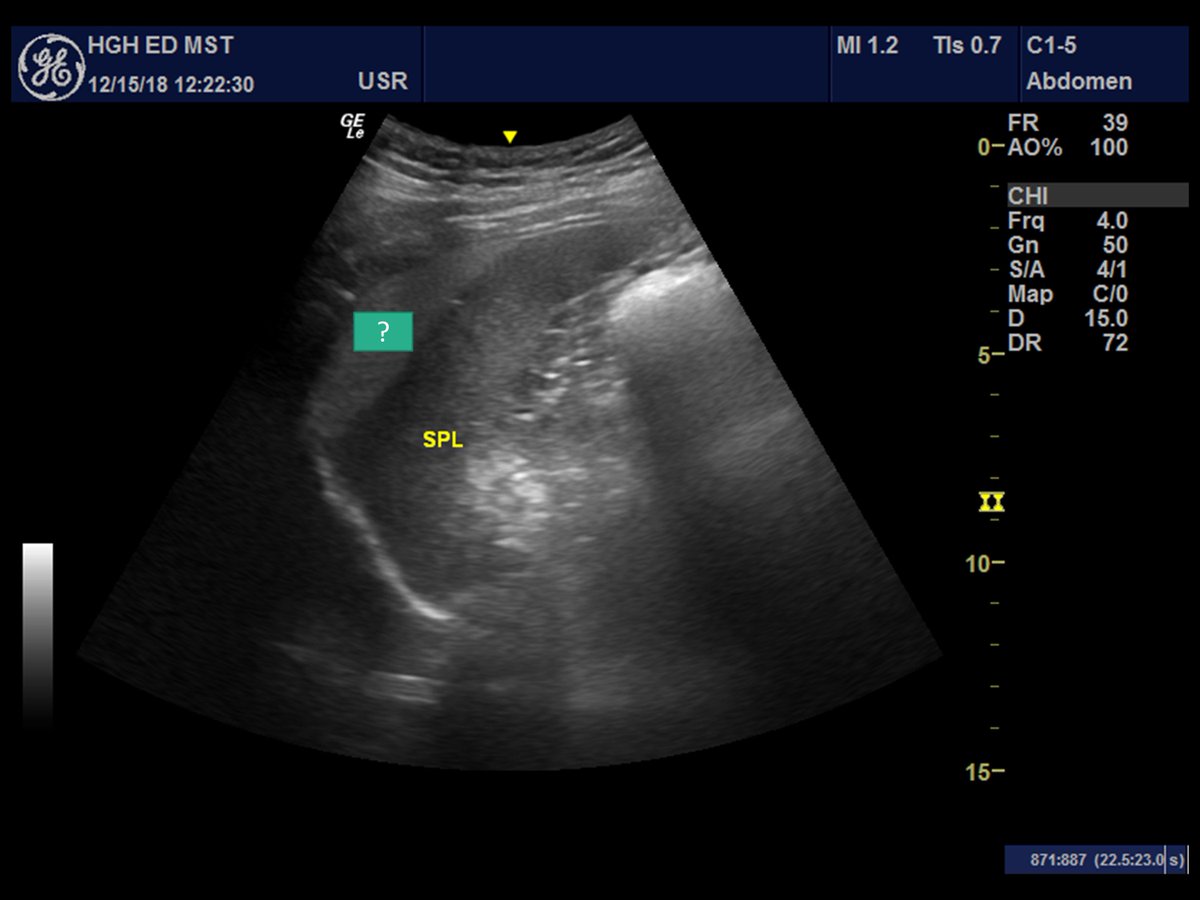
#POCUS #VenousEXcessUScore guided diuresis in ❤️renal sx. Pt w T2DM and CKDG4A3 with HFpEF. After multi-agent diuresis (targeted to normalize venous flow patterns) pt lost 14 kg and returned to basal kidney function. ¿Should we pursue "decongestion" goals in these pts? (1/13) 
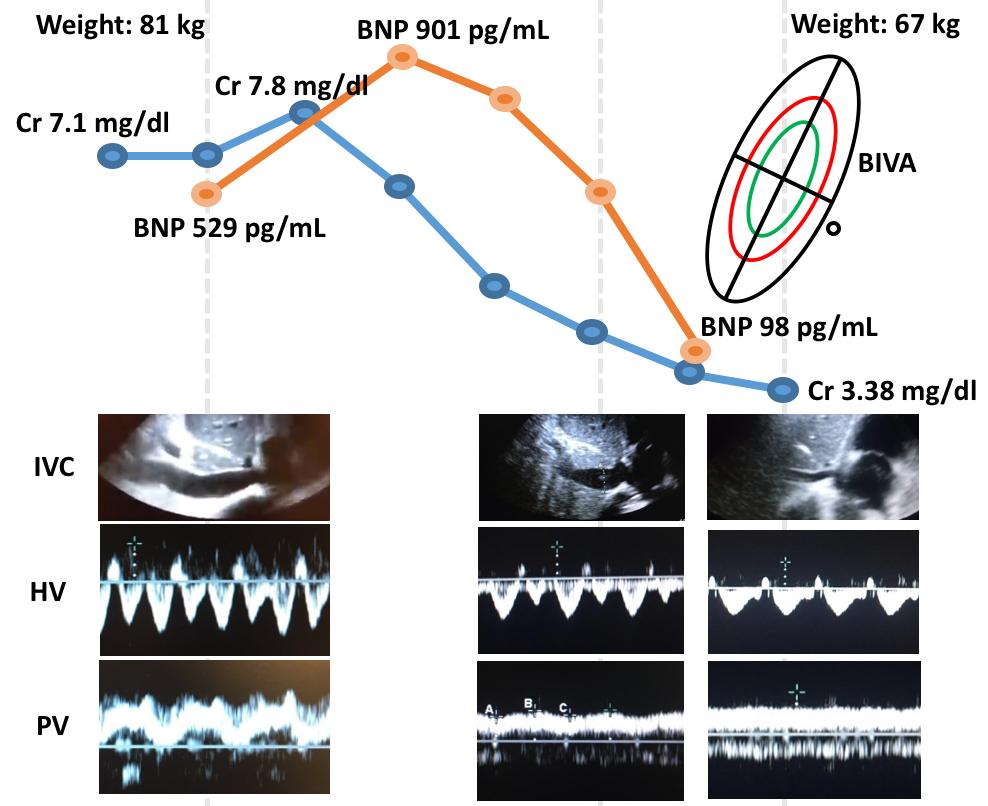
It's interesting that the recent statement from @American_Heart spends a great deal discussing Bioelectrical impedance Vector Analysis (BIVA) as an aid to guide discharge and diuresis goals (2/13)
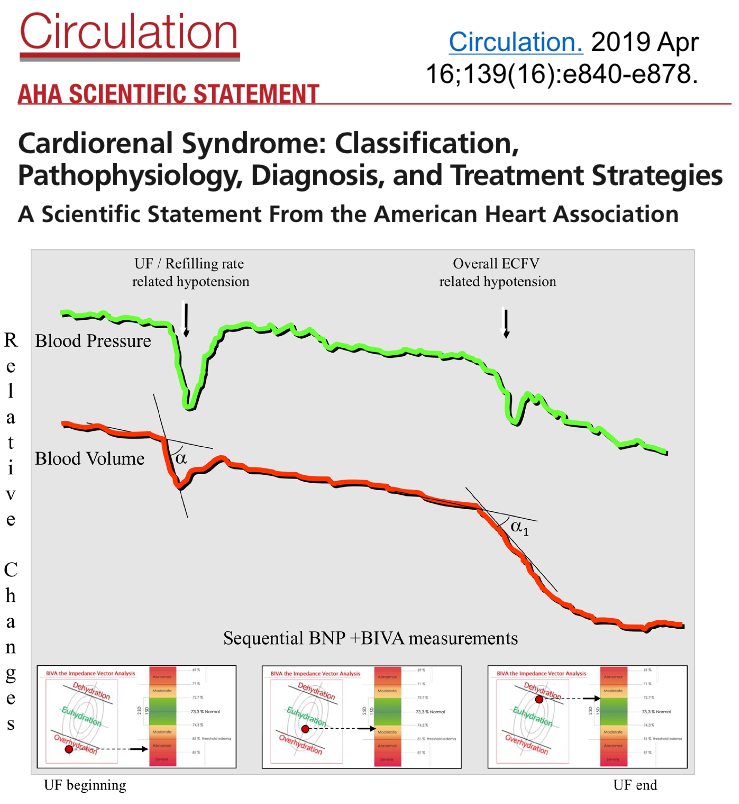
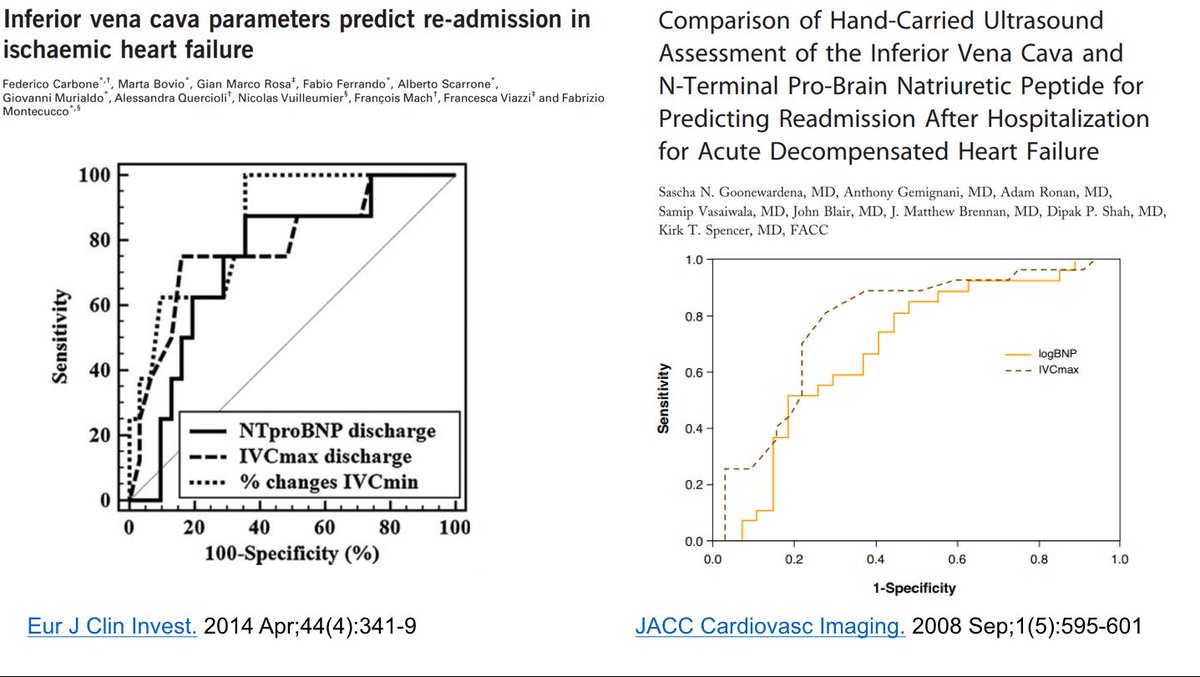
There is some evidence that "Hidration Status" (by BIVA) at discharge predicts CV events better than BNP. However for some reason this study used admission BNP while it is most likely that discharge BNP is the one that matters (3/13)


Its worth looking at this study by Valle. Their protocol assigned pts whose BNP remained >250 after clinical stability (84%) to receive aggressive diuresis guided by BIVA and WRF. After aggressive tx, 18% achieved BNP goals and had as good outcomes as early responders (4/13)


66% of patients (Non Responders) did not achieve BNP goals. Surely most of them must have severe ❤️disease and thus unattainable BNP despite tx. However one might question if "Dehydration by BIVA" or WRF was the correct "Stopping Point", ¿How many remained "congestive"? (5/13)

BIVA can give an estimate of TBW and also ECW. However "euvolemia" or "normal hydration" is based on averages from healthy populations. Readings form pts w HF and no peripheral edema are very similar to readings from pts w/o HF. ¿Is it then useful to guide therapy? (6/13)

¿Should "normal hydration" even be the target? Even if you could accurately measure blood volume (Which BIVA can't), the distribution of this volume MUST be different in every patient (splanchnic compliance, venous tone, etc). ¿What is "Euvolemia" anyway? (7/13)

It is quite possible that congestive organ dysfunction is related to CV mechanical power (Work/Time) on venous flow (See @heart_lung recent post) (8/13)
Only STRESSED volume contributes (BV/Venous capacitance). And its systemic effects also depend on ❤️ fx. Summarised by the concept of "Cardiac Performance (Eh). So even if stressed volume is nl or even low, congestion can still exist (given poor❤️fx) and thus high RAP (9/13)

Increased stress volume + reduced Cardiac performance promotes "veno-cardiac uncoupling" which might be the actual cause of organ dysfunction if CHF. *Notice that BIVA can't possibly measure Eh, venous capacitance and is not even accurate for determining blood Volume! (10/13)

Enter #POCUS! "Congestive" Venous Flow patterns might reflect "Veno-Cardiac Uncoupling". Intrarenal Doppler US is a very powerful predictor of CV outcomes in HF, and it is INDEPENDENT of RAP (Consistent with the Veno-Cardiac Uncoupling theory). IVC is also good predictor! (11/13)
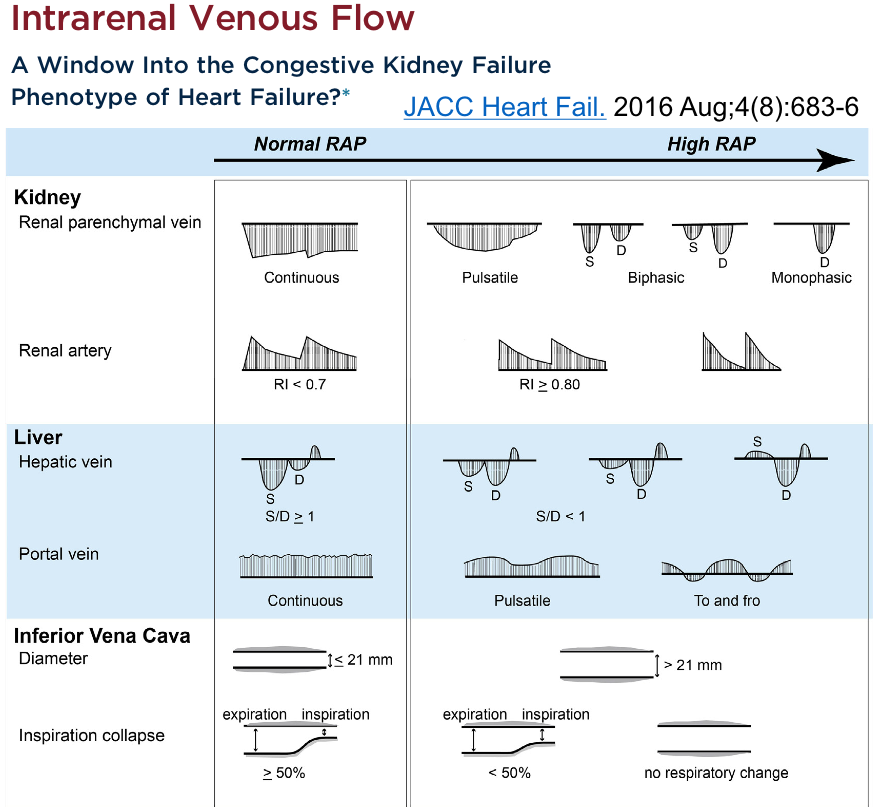
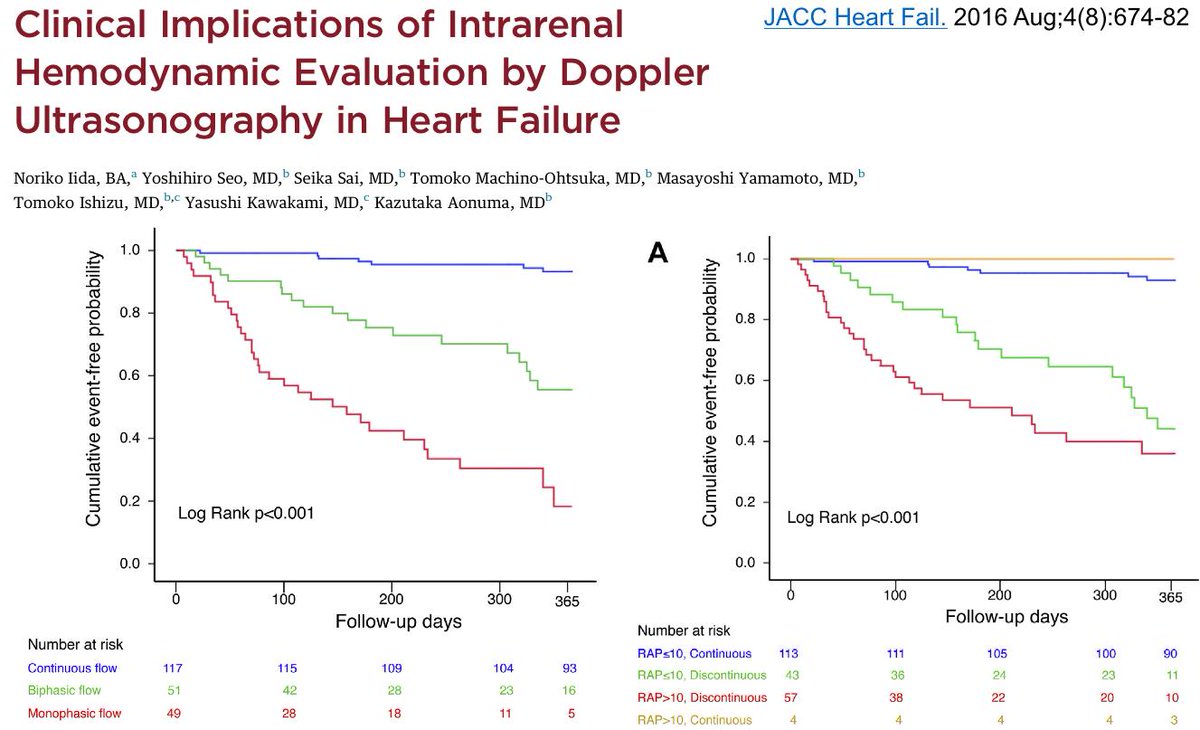
Intrarenal doppler might require advanced training. Hepatic Vein and Portal Vein doppler + IVC (VEXUS) could be an easier way to evaluate "Veno-Cardiac Uncoupling". Portal Vein Pulsatility shows good agreement with intrarenal doppler patterns and predicts renal outcomes! (12/13)


Congestive organ dysfunction depends on Cardiac Performance (Eh) and Stressed Volume (which depends on venous capacitance and blood volume). BIVA will only approximate blood volume assuming no third spacing 👎. #POCUS guided diuresis might be correct target! (13/13)
Would love to hear some thoughts. Ping @ThinkingCC @khaycock2 @EMNerd_ @heart_lung @iceman_ex @LMSaxhaug @WBeaubien @PulmCrit