We all learn in medical school to give calcium in hyperkalemia for ‘membrane stabilization’. But what does ‘membrane stabilization’ actually mean? 🤷♀️ #iforgot #medschool #nephtwitter #tweetorial #physiology #pleasecareeventhoughstep1ispassfail
2/
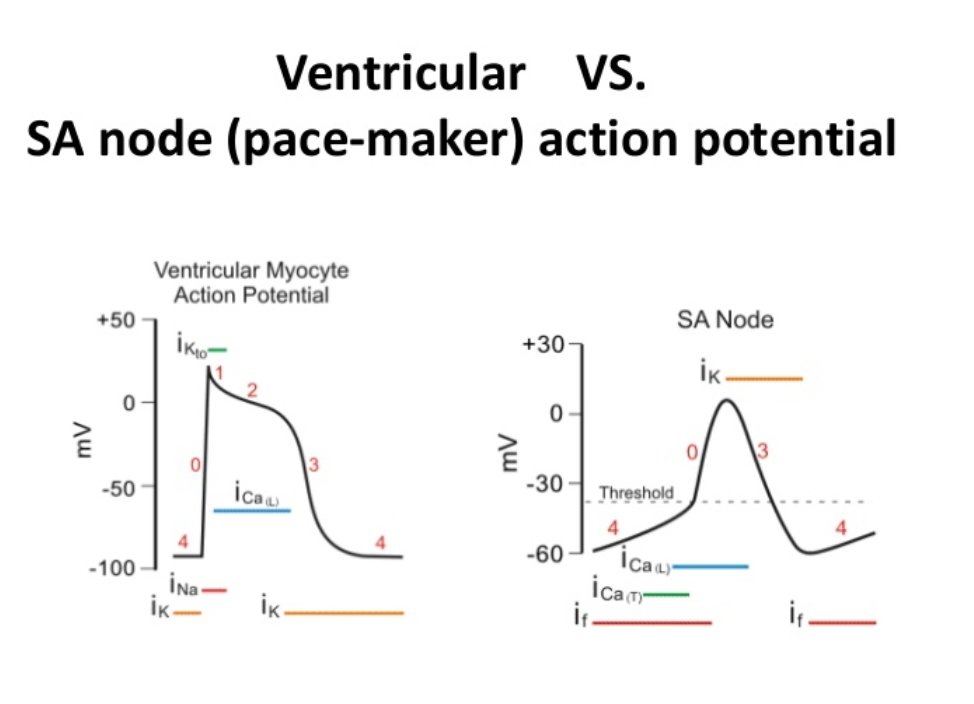
Trick question - because there are 2 answers! But before we tackle hyperkalemia, check out this brief but brilliant refresher on action potentials in the heart.
Trick question - because there are 2 answers! But before we tackle hyperkalemia, check out this brief but brilliant refresher on action potentials in the heart.
3/
Now, hyperkalemia raises the resting membrane potential of cardiac myocytes, shifting them closer to the threshold for activation.
This should make the myocytes more irritable and easily activated - which it does... at first!
Now, hyperkalemia raises the resting membrane potential of cardiac myocytes, shifting them closer to the threshold for activation.
This should make the myocytes more irritable and easily activated - which it does... at first!
4/
But why then are the dangers of hyperkalemia actually related to slowed conduction - manifested by P wave widening, QRS widening, AV blocks and bradycardia? Why does this happen?
But why then are the dangers of hyperkalemia actually related to slowed conduction - manifested by P wave widening, QRS widening, AV blocks and bradycardia? Why does this happen?
5/
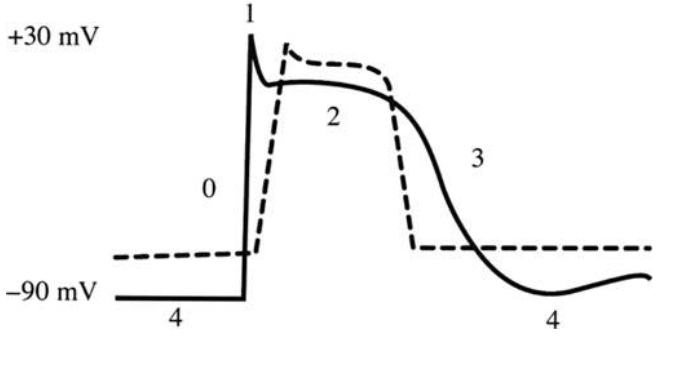
Right, hyperkalemia raises the resting membrane potential AND slows depolarization at phase 0… let’s take a closer look at the action potential in hyperkalemia (dashed line) compared to normal (solid line)🧐
Image source: ncbi.nlm.nih.gov/pmc/articles/P…
Right, hyperkalemia raises the resting membrane potential AND slows depolarization at phase 0… let’s take a closer look at the action potential in hyperkalemia (dashed line) compared to normal (solid line)🧐
Image source: ncbi.nlm.nih.gov/pmc/articles/P…
6/
Notice that Phase 0, when sodium is rushing into the cell 🏃🏻, appears...slower 🐢. Why is that?
Notice that Phase 0, when sodium is rushing into the cell 🏃🏻, appears...slower 🐢. Why is that?
7/
The slope 🧗🏽♂️ of Phase 0 is called Vmax, and it is slowed because the voltage gated sodium channels like to be at their usual resting potential of -75mV.
When the resting potential is more positive (ie in hyperkalemia), these sodium channels are inactivated, or closed.
The slope 🧗🏽♂️ of Phase 0 is called Vmax, and it is slowed because the voltage gated sodium channels like to be at their usual resting potential of -75mV.
When the resting potential is more positive (ie in hyperkalemia), these sodium channels are inactivated, or closed.
8/
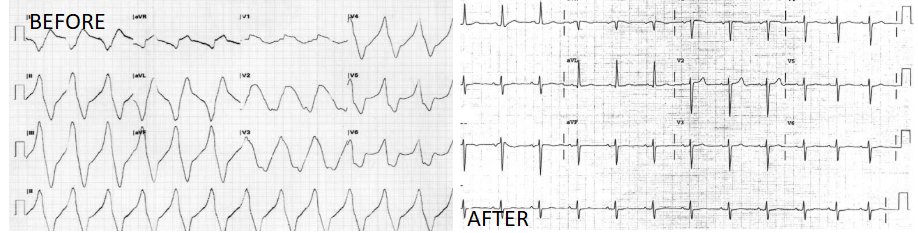
Now, back to the original question - what happens when you give calcium?
If you were to check an EKG before and after you push calcium gluconate in a patient with hyperkalemia, this is what you might see. Image source: ncbi.nlm.nih.gov/pmc/articles/P…
Now, back to the original question - what happens when you give calcium?
If you were to check an EKG before and after you push calcium gluconate in a patient with hyperkalemia, this is what you might see. Image source: ncbi.nlm.nih.gov/pmc/articles/P…
9/
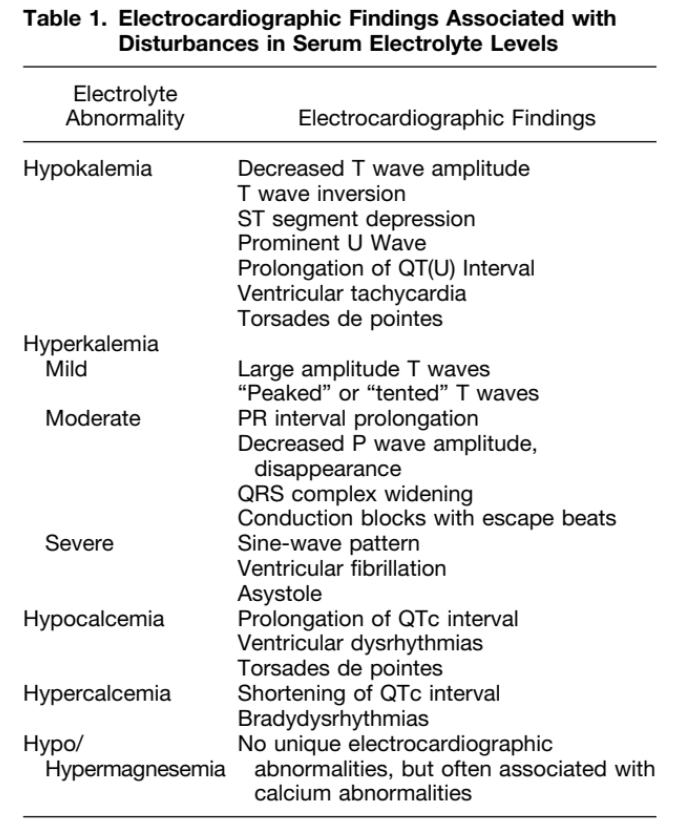
Of course, other EKG changes may occur at different stages of hyperkalemia. Check out this review for a summary: ncbi.nlm.nih.gov/pubmed/15261358
Of course, other EKG changes may occur at different stages of hyperkalemia. Check out this review for a summary: ncbi.nlm.nih.gov/pubmed/15261358
10/
Finally, for the story of calcium ...Calcium has long been known to raise the threshold for depolarization, restoring the difference between resting & threshold potentials. So it becomes less easy to reach the threshold to depolarize than it otherwise would in hyperkalemia.
Finally, for the story of calcium ...Calcium has long been known to raise the threshold for depolarization, restoring the difference between resting & threshold potentials. So it becomes less easy to reach the threshold to depolarize than it otherwise would in hyperkalemia.
11/
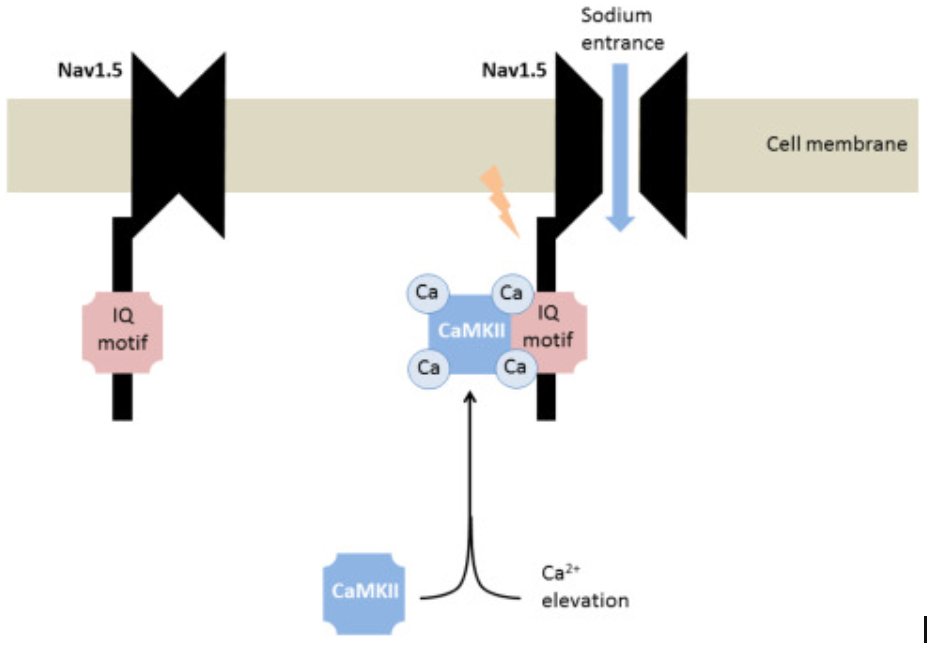
Remember those voltage gated Na channels that remain closed in hyperkalemia? Calcium binds them via calmodulin and helps them open back up again! The rate of depolarization, or Vmax, in Phase 0 is thus restored.
Image source: kidney-international.org/article/S0085-…
Remember those voltage gated Na channels that remain closed in hyperkalemia? Calcium binds them via calmodulin and helps them open back up again! The rate of depolarization, or Vmax, in Phase 0 is thus restored.
Image source: kidney-international.org/article/S0085-…
12/
And last but not least, calcium can even produce its own action potential via slow L-type calcium channels found most abundantly in pacemaker cells (in the SA and AV node). Image source: slideshare.net/AmrElsharkawy1…
And last but not least, calcium can even produce its own action potential via slow L-type calcium channels found most abundantly in pacemaker cells (in the SA and AV node). Image source: slideshare.net/AmrElsharkawy1…
13/
Calcium influx via L-type Ca channels is predominant not only in pacemaker cells, but also in regular myocytes in which the sodium influx has been suppressed - as in hyperkalemia. Source: ncbi.nlm.nih.gov/pmc/articles/P…
Calcium influx via L-type Ca channels is predominant not only in pacemaker cells, but also in regular myocytes in which the sodium influx has been suppressed - as in hyperkalemia. Source: ncbi.nlm.nih.gov/pmc/articles/P…
14/
There is limited evidence that this may be a major mechanism by which calcium restores cardiac conductivity in hyperkalemia. Source: sciencedirect.com/science/articl…
There is limited evidence that this may be a major mechanism by which calcium restores cardiac conductivity in hyperkalemia. Source: sciencedirect.com/science/articl…
15/
So how does calcium help in hyperkalemia?
- Calcium restores the gradient between resting and threshold potential (phase 4)
- Calcium opens voltage-gated Na channels (phase 0)
-Calcium depolarizes pacemaker cells and may help depolarize myocytes when Na channels are inactive
So how does calcium help in hyperkalemia?
- Calcium restores the gradient between resting and threshold potential (phase 4)
- Calcium opens voltage-gated Na channels (phase 0)
-Calcium depolarizes pacemaker cells and may help depolarize myocytes when Na channels are inactive
16/
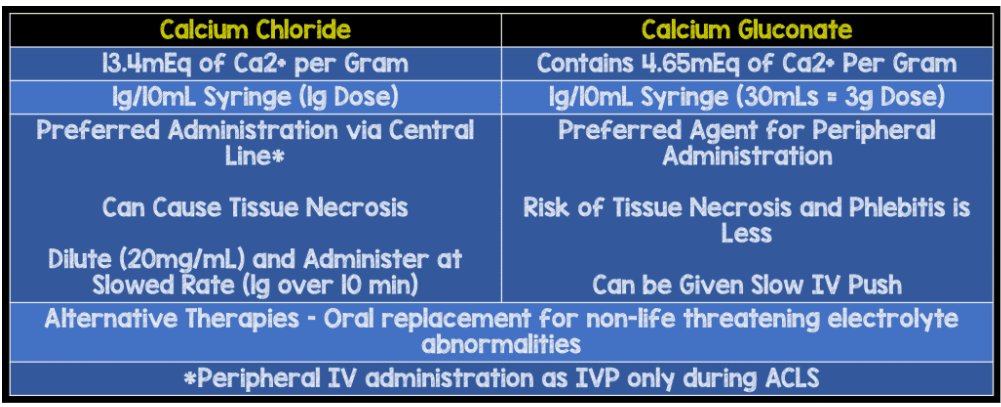
☝️ Bonus question: When would you give calcium chloride versus calcium gluconate?
Remember that calcium chloride has 3X the elemental calcium, but is also associated with more tissue necrosis! Image source: rebelem.com/whats-your-dru…
☝️ Bonus question: When would you give calcium chloride versus calcium gluconate?
Remember that calcium chloride has 3X the elemental calcium, but is also associated with more tissue necrosis! Image source: rebelem.com/whats-your-dru…