At the population level, there will be FOUR TYPES of #COVID19 #mortality:
1) Direct-direct
2) Direct-indirect
3) Indirect
4) Competing risks
In this short thread, I will discuss the four.
1) Direct-direct
2) Direct-indirect
3) Indirect
4) Competing risks
In this short thread, I will discuss the four.
1) Direct-direct
Basically, these are the deaths that are being counted in real time (on your dashboards, etc.) and attributed to #COVID.
These are deaths, typically in hospital, typically with a positive test. Might be coded as underlying cause of death ICD-10 J22...
Basically, these are the deaths that are being counted in real time (on your dashboards, etc.) and attributed to #COVID.
These are deaths, typically in hospital, typically with a positive test. Might be coded as underlying cause of death ICD-10 J22...
Direct-direct (cont'd)
These are, basically: "This person died of COVID"
This category (D-d) is what everyone (dashboards, the press, etc.) is counting, and it's essentially a tally.
Many of these deaths will also be coded as U07.1:
who.int/classification…
These are, basically: "This person died of COVID"
This category (D-d) is what everyone (dashboards, the press, etc.) is counting, and it's essentially a tally.
Many of these deaths will also be coded as U07.1:
who.int/classification…
2) Direct-indirect
These are early COVID deaths that were mistaken for influenza, and later COVD deaths that are somehow not recorded as such.
These will be coded things like: ICD-10 J11, J18, etc.
These *do* *not* show up in your dashboards or in the press.
These are early COVID deaths that were mistaken for influenza, and later COVD deaths that are somehow not recorded as such.
These will be coded things like: ICD-10 J11, J18, etc.
These *do* *not* show up in your dashboards or in the press.
Direct-indirect, cont'd
These are NOT simply a tally and will have to be inferred from seeing excess deaths in J11, J18, etc., relative to expectations.
There are relatively non-controversial models to calculate expected, and, hence, excess, mortality, but it's not a tally.
These are NOT simply a tally and will have to be inferred from seeing excess deaths in J11, J18, etc., relative to expectations.
There are relatively non-controversial models to calculate expected, and, hence, excess, mortality, but it's not a tally.
3) Indirect.
This is — for example — someone who dies of a broken femur (ICD 10 S72 in this example) because this injury was not treated in the emergency department altho under normal circumstances it would not cause death in most cases.
This is — for example — someone who dies of a broken femur (ICD 10 S72 in this example) because this injury was not treated in the emergency department altho under normal circumstances it would not cause death in most cases.
Indirect, cont'd.
This mortality is *not* *counted* in the dashboards, etc.
It is not a tally and will have to be inferred afterwards from models, as with Direct-indirect.
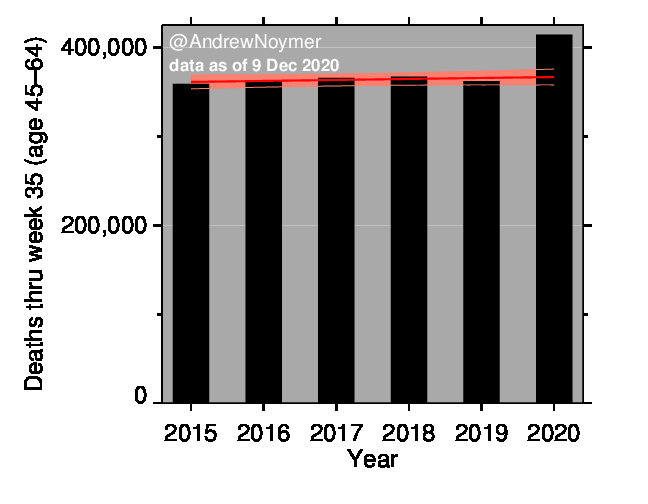
This is one of the huge "X-factors", especially as regards mortality at ages below 60.
This mortality is *not* *counted* in the dashboards, etc.
It is not a tally and will have to be inferred afterwards from models, as with Direct-indirect.
This is one of the huge "X-factors", especially as regards mortality at ages below 60.
4) Competing risks.
This isn't reallly a category of deaths, per se, but is highly relevant.
This refers to the fact that — for example — someone who dies of #COVID now may have been otherwise destined to die of a heart attack in a July heat wave...
This isn't reallly a category of deaths, per se, but is highly relevant.
This refers to the fact that — for example — someone who dies of #COVID now may have been otherwise destined to die of a heart attack in a July heat wave...
Competing risks, cont'd.
Competing risks means that (e.g.) heart disease deaths could — in principle, anyways — *decline* due to #COVID2019
But it's a decline for the wrong reasons. We can only die once, +some COVID deaths will have been borrowed, so to say, from other causes.
Competing risks means that (e.g.) heart disease deaths could — in principle, anyways — *decline* due to #COVID2019
But it's a decline for the wrong reasons. We can only die once, +some COVID deaths will have been borrowed, so to say, from other causes.
Competing risks, cont'd.
This is another "X-factor". We don't really know how much this will matter.
Demographers will pore over the data (ex-post) and use multiple-decrement life tables to understand this phenomenon....
This is another "X-factor". We don't really know how much this will matter.
Demographers will pore over the data (ex-post) and use multiple-decrement life tables to understand this phenomenon....
Stay tuned... but it will be a while before we understand all the dimentions of #COVID19 mortality. /end.
Addendum 1: There are health effects of recessions. Per past research, these often — counter-intuitively — reduce mortality, on net.
This will be difficult to disentangle, except for the period in which the recession out-lasts the epidemic.
This will be difficult to disentangle, except for the period in which the recession out-lasts the epidemic.
Addendum 2: Scarring.
It's too early to say if COVID will see this kind of effect, in which survivors of infection have durable health problems. We will have to monitor for years...
It's too early to say if COVID will see this kind of effect, in which survivors of infection have durable health problems. We will have to monitor for years...
Scarring, cont'd
There is an hypothesis that 1918 flu caused cardiac scarring, which in turn generated the 20th century heart disease mortality epidemic in the decades thereafter.
Full disclosure: I have argued that for 1918, this isn't correct. Link: doi.org/10.7717/peerj.…
There is an hypothesis that 1918 flu caused cardiac scarring, which in turn generated the 20th century heart disease mortality epidemic in the decades thereafter.
Full disclosure: I have argued that for 1918, this isn't correct. Link: doi.org/10.7717/peerj.…
• • •
Missing some Tweet in this thread? You can try to
force a refresh