
MIS-C Tweetorial: Here’s recent alert from CDC regarding this multisystem inflammatory syndrome in children (MIS-C, or #PIMSTS on #medtwitter). emergency.cdc.gov/han/2020/han00…. This Kawasaki-like syndrome was noted about 4 weeks after #COVID peak in Italy #PedsICU
CDC named it MIS-C, diagnosed by:
✅T>38 for 24hrs
✅⬆️CRP, ESR, ferritin, procal, or IL-6, etc
✅>=2 organ system dysfxn
✅no other infxn/reason for sxs
✅recent #COVID19 or just exposure (many are PCR-, variable serology)
✅T>38 for 24hrs
✅⬆️CRP, ESR, ferritin, procal, or IL-6, etc
✅>=2 organ system dysfxn
✅no other infxn/reason for sxs
✅recent #COVID19 or just exposure (many are PCR-, variable serology)
Kawasaki Disease for those not in the know: Basically, vasculopathy with diffuse inflammation and fever with some combo of:
Rash, conjunctivitis, mucositis, adenopathy, ext changes (early swelling later desquamation)
AHA official recs: ahajournals.org/doi/10.1161/CI…
Rash, conjunctivitis, mucositis, adenopathy, ext changes (early swelling later desquamation)
AHA official recs: ahajournals.org/doi/10.1161/CI…
Kawasaki kids are typically younger (preschool/infants) and they are not sick. Ward level but require IVIG and ASA to prevent coronary aneurysms. This new #PIMSTS is a little different....
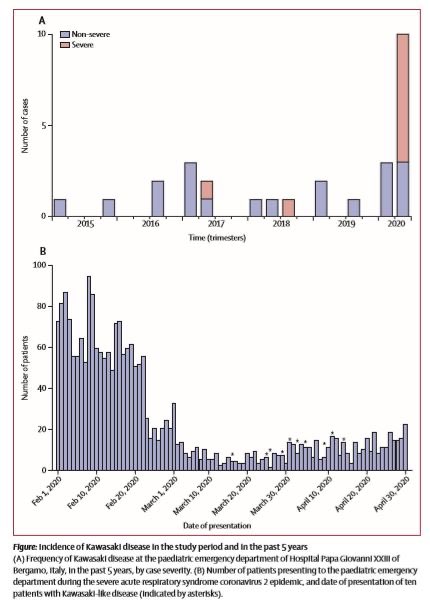
First, there’s this clear temporal relationship with #COVID infection. Currently, ~25% PCR+, majority +serology, but some with no history and neg labs. Check out the Italian study here who started seeing it ~1 month post COVID peak 
Spain, UK, and NY have seen similar timing. NY with >100 cases and ~3 deaths. While 80% of hospitalized peds COVID cases have pre-existing illnesses, virtually all of these #PIMSTS kids are healthy. What’s most important is they are much sicker: ~2/3 ICU
Disclaimer: What follows is just anecdotal obs (NY DoH webinar 5/14 by several Picu docs), numbers not reviewed and will change: Here’s the webinar:
totalwebcasting.com/view/?func=VOF…
totalwebcasting.com/view/?func=VOF…
Older: mean 8yo, but 1/2 are 11-20yo,
male predominance
Most present with fever and GI sxs
Cardiac issues (>60%) are occurring EARLY
Troponin leak common
male predominance
Most present with fever and GI sxs
Cardiac issues (>60%) are occurring EARLY
Troponin leak common
They are very inflamed:
CRP super high
Ferritin >1000
d-dimer >2000
Pro-BNP >7000
Half have liver and kidney dysfxn
Neutrophilia but lymphopenic
Low NA and alb
High TG
CRP super high
Ferritin >1000
d-dimer >2000
Pro-BNP >7000
Half have liver and kidney dysfxn
Neutrophilia but lymphopenic
Low NA and alb
High TG
Management:
Good supportive ICU care (pressors, careful fluids)
Serial Echos
IVIG and ASA per AHA Kawasaki guidelines
Otherwise not evidence based:
-most getting steroids
-immune mods case-by-case with rheum
-lovenox prophylaxis, many get Tx dose
Good supportive ICU care (pressors, careful fluids)
Serial Echos
IVIG and ASA per AHA Kawasaki guidelines
Otherwise not evidence based:
-most getting steroids
-immune mods case-by-case with rheum
-lovenox prophylaxis, many get Tx dose
Unanswered questions:
1. Should IVIG/ASA be given before Kawasaki criteria?
2. Is this present in older “kids” 20-30yo?
3. If 21yo+ meet criteria, should they be getting IVIG/ASA?
4. Criteria for steroids/rheum drugs?
5. Anticoags?
6. Overlap with adult CRS?
1. Should IVIG/ASA be given before Kawasaki criteria?
2. Is this present in older “kids” 20-30yo?
3. If 21yo+ meet criteria, should they be getting IVIG/ASA?
4. Criteria for steroids/rheum drugs?
5. Anticoags?
6. Overlap with adult CRS?
Here’s initial overview from the UK rcpch.ac.uk/sites/default/… <end>
@chungk1031 this #tweetorial is for you 😉

