
Hard to think about #EndNeurophobia #neurology #tweetorials when I know we're all thinking/tweeting more about #EndRacism!
But #MedStudentTwitter asked and I will deliver....To f/u on CPSolvers recent case of ataxia
Here are the basics of CEREBELLUM and ATAXIA!
1
But #MedStudentTwitter asked and I will deliver....To f/u on CPSolvers recent case of ataxia
Here are the basics of CEREBELLUM and ATAXIA!
1
But first, a moment of silence for
#GeorgeFloyd
#AhmaudArbery
#BreonnaTaylor
and other lives lost to racism, structural violence, police brutality
.
.
.
.
.
.
.
#GeorgeFloyd
#AhmaudArbery
#BreonnaTaylor
and other lives lost to racism, structural violence, police brutality
.
.
.
.
.
.
.
I’m grateful for all the❤️#EndNeurophobia has received but hope you’ll check out the rest of my feed, which seeks to amplify voices I’m learning from in the path to being an antiracist ally. Want to learn more? Follow & learn:
@uche_blackstock @DrOniBee @LashNolen @michellemorse
@uche_blackstock @DrOniBee @LashNolen @michellemorse
OK so:
The main function of the cerebellum is coordination of motor actions including eye movements and speech.
It even has a role in cognition (check out Jeremy Schmahmann’s work to learn more). sciencedirect.com/science/articl…
But here let’s focus on the motor coordination aspect.
The main function of the cerebellum is coordination of motor actions including eye movements and speech.
It even has a role in cognition (check out Jeremy Schmahmann’s work to learn more). sciencedirect.com/science/articl…
But here let’s focus on the motor coordination aspect.
First a little basic anatomy. Cerebellum sits posterior to the brainstem, inferior to the occipital lobes.
For clinical purposes know: L and R hemispheres, and between them midline vermis.
For clinical purposes know: L and R hemispheres, and between them midline vermis.
In general, midline vermis lesions affect axial coordination, so lesions can cause gait and truncal ataxia.
Hemispheric lesions cause ipsilateral limb ataxia, dysdiadochokinesia, dysmetria, etc.
Hemispheric lesions cause ipsilateral limb ataxia, dysdiadochokinesia, dysmetria, etc.
So how does the cerebellum coordinate actions?
It needs to know 2 things:
1 The motor action the brain wants to perform
2 Where the body (and head) are in space
It then compares current body position w goal position, and comes up w a plan to help the brain reach its goal.
It needs to know 2 things:
1 The motor action the brain wants to perform
2 Where the body (and head) are in space
It then compares current body position w goal position, and comes up w a plan to help the brain reach its goal.
So the cerebellum needs 2 inputs (motor plan from brain; proprioceptive/vestibular info from body/head) and 1 output (calculated coordination info back to brain)
These 2 inputs + 1 output travel in the 3 pairs of CEREBELLAR PEDUNCLES
These 2 inputs + 1 output travel in the 3 pairs of CEREBELLAR PEDUNCLES

INferior cerebellar peduncle (medullar level) mostly brings information INto the cerebellum: proprioceptive (from dorsal columns) and vestibular (from CN8 nuclei in medulla)
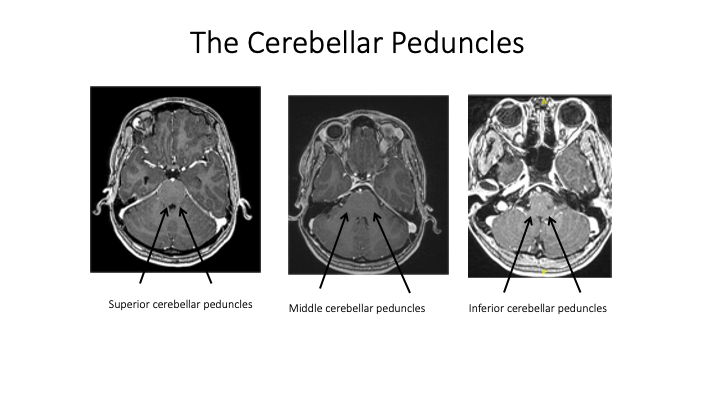
Middle cerebellar peduncle brings information from the Motor regions of the brain to the cerebellum (corticopontocerebellar fibers run with the corticospinal tracts and essentially “cc” the motor plan )
sUPerior cerebellar peduncle=mostly output back UP to brain (via red nucleus and VL nuc of thalamus)
(Note a few other pathways travel in the inf/sup that don’t all obey the Inf/In and sUP/UP but have little clinical relevance)
(Note a few other pathways travel in the inf/sup that don’t all obey the Inf/In and sUP/UP but have little clinical relevance)
Cerebellar hemisphere lesions cause IPSILATERAL limb ataxia (unlike cerebral hemisphere lesions, which tend to cause contralateral deficit).
(Gourmet anatomy pearl: L cerebral hemisphere and R cerebellar hemisphere communicate; R cerebral hemisphere->L cerebellar hemisphere. So info in MCPs is crossed on way down (in ventral pons); SCP info crosses on way up (en route to red nucl / VL of thalamus))
Cerebellum shares blood supply w/brainstem from vertebrobasilar system: SCAs, AICAs, PICAs (see brainstem tweetorial!)
Now if you see ATAXIA, don’t always assume it’s cerebellar.
Since cerebellum relies on sensory input, lesions of the sensory pathways (e.g., dorsal columns or sensory neuropathy or ganglionopathy) can cause SENSORY ataxia. table has tips for distinguishing them!
Since cerebellum relies on sensory input, lesions of the sensory pathways (e.g., dorsal columns or sensory neuropathy or ganglionopathy) can cause SENSORY ataxia. table has tips for distinguishing them!

while we're discussing the exam, Romberg is NOT a cerebellar sign, it's a sign of decreased PROPRIOCEPTION (e.g., dorsal columns or peripheral nerves). If someone has bad cerebellar ataxia, they probably won't even be able to stand w feet together and eyes open let alone closed
Let’s say you see cerebellar ataxia, what’s the DDx?
First, is it unilateral or bilateral? Then time course!
My E=mc2 of neurology is
DDx= Localization x Time course
First, is it unilateral or bilateral? Then time course!
My E=mc2 of neurology is
DDx= Localization x Time course
Sudden/Hyperacute ataxia
-Unilateral: ischemic stroke or hemorrhage
-Bilateral: toxic (alcohol, cytarabine)
Acute ataxia (hours-days)
-Unilateral: demyelinating (eg MS flare)
-Bilateral: Cerebellitis (e.g., pediatric post-VZV)
-Unilateral: ischemic stroke or hemorrhage
-Bilateral: toxic (alcohol, cytarabine)
Acute ataxia (hours-days)
-Unilateral: demyelinating (eg MS flare)
-Bilateral: Cerebellitis (e.g., pediatric post-VZV)
Subacute ataxia
- Unilateral: tumor (mets in adults, primary in kids) or PML (loves middle cerebellar peduncle)
- Bilateral: Paraneoplastic (ovary, breast, testicular)
Chronic
- Degenerative: MSA-C, inherited (Friedreich, SCA, etc)
- Toxic: Chronic ETOH or phenytoin use
- Unilateral: tumor (mets in adults, primary in kids) or PML (loves middle cerebellar peduncle)
- Bilateral: Paraneoplastic (ovary, breast, testicular)
Chronic
- Degenerative: MSA-C, inherited (Friedreich, SCA, etc)
- Toxic: Chronic ETOH or phenytoin use
** PEARL: Don't miss paraneoplastic cerebellar degeneration!! Subacute symmetric ataxia & nystagmus in an adult with normal imaging = PAN SCAN and find the tumor**
I once saw my mentor diagnose a CPC after the first sentence! Subacute symmetric ataxia in woman > 50 = ovarian CA
I once saw my mentor diagnose a CPC after the first sentence! Subacute symmetric ataxia in woman > 50 = ovarian CA
Feeling steadier now with all this?
@CrystalYeoMDPhD @MadSattinJ @Tracey1milligan @DxRxEdu @CPSolvers @SchmahmannLab
@CrystalYeoMDPhD @MadSattinJ @Tracey1milligan @DxRxEdu @CPSolvers @SchmahmannLab
@threadreaderapp unroll pls


