1. How do we tell primary lung cancer from metastatic cancers from other sites?
It’s correct to say we should use all available clinical, radiologic and pathologic information, but that’s too vague to be helpful in a practical sense.
Here I offer some tips. #tweetorial
It’s correct to say we should use all available clinical, radiologic and pathologic information, but that’s too vague to be helpful in a practical sense.
Here I offer some tips. #tweetorial
2. This #pathtweetorial is applicable mainly to #pulmpath . The principles in each organ are different. A carcinoma in a lymph node is a metastasis by definition. Not so in lung or colon.
IMHO it’s a mistake to approach a carcinoma in the lung as carcinoma of unknown primary
IMHO it’s a mistake to approach a carcinoma in the lung as carcinoma of unknown primary
3. Most metastatic carcinomas to the lung occur after the primary carcinoma has already been diagnosed in another site.
💥Clinicians: give your pathologists this information! If you don’t, this is substandard, dangerous patient care.
💥Clinicians: give your pathologists this information! If you don’t, this is substandard, dangerous patient care.
4. One thing I’ve realized after 13 doing lung pathology is that most clinicians (even experts) don’t understand the powers and limitations of pathologists.
Also, pathologists don’t always grasp the clinical question.
This is a recipe for confusion.
Also, pathologists don’t always grasp the clinical question.
This is a recipe for confusion.
5. So let’s start with the clinical. In an elderly smoker with a solitary spiculated lung mass and no history of malignancy, the clinical question is: “is this malignant”? If so, what type?
Not: “is this a metastasis from an occult primary?”
Not: “is this a metastasis from an occult primary?”
6. In the situation in tweet 5, #ihcpath are justified if needed for subtyping, but not for site of origin. If you do immunos, you’re answering a question that nobody is asking.
And if the sample is a biopsy you’re wasting precious tissue.
And if the sample is a biopsy you’re wasting precious tissue.
7. Now let’s look at the other extreme. Known history of extrapulmonary carcinoma, mutiple bilateral lung nodules and morphology that fits. You almost don’t need #ihcpath here either.
If you want to do ihc just to confirm it’s not lung that’s ok.
If you want to do ihc just to confirm it’s not lung that’s ok.
8. In most metastases to the lung from other sites, history, imaging and morphology all align together and suggest a met. Easy.
“But I never get any clinical history!!” some will say. Well then, your clinicians are putting patients in danger.
“But I never get any clinical history!!” some will say. Well then, your clinicians are putting patients in danger.
9. Immunohistochemistry can never solve all problems created by insufficient communication of history, insufficient history taking or lack of access to EMR for pathologists. Ditto for morphology. We will make some heroic saves but this is not ideal.
10. One of our thoracic surgeons (@DanRaymondMD ) emails us when he does a lobectomy or wedge resection on a case where he knows there is a history of carcinoma elsewhere. He wants us to know because he cares about his patients. This is not a game of gotcha.
11. Now let’s address problem areas: what about a patient with a history of carcinoma but only a solitary lung mass?
ALWAYS consider a met in this situation, even if the mass is large and solitary. #IHCpath can be very helpful (know your pitfalls)
ALWAYS consider a met in this situation, even if the mass is large and solitary. #IHCpath can be very helpful (know your pitfalls)
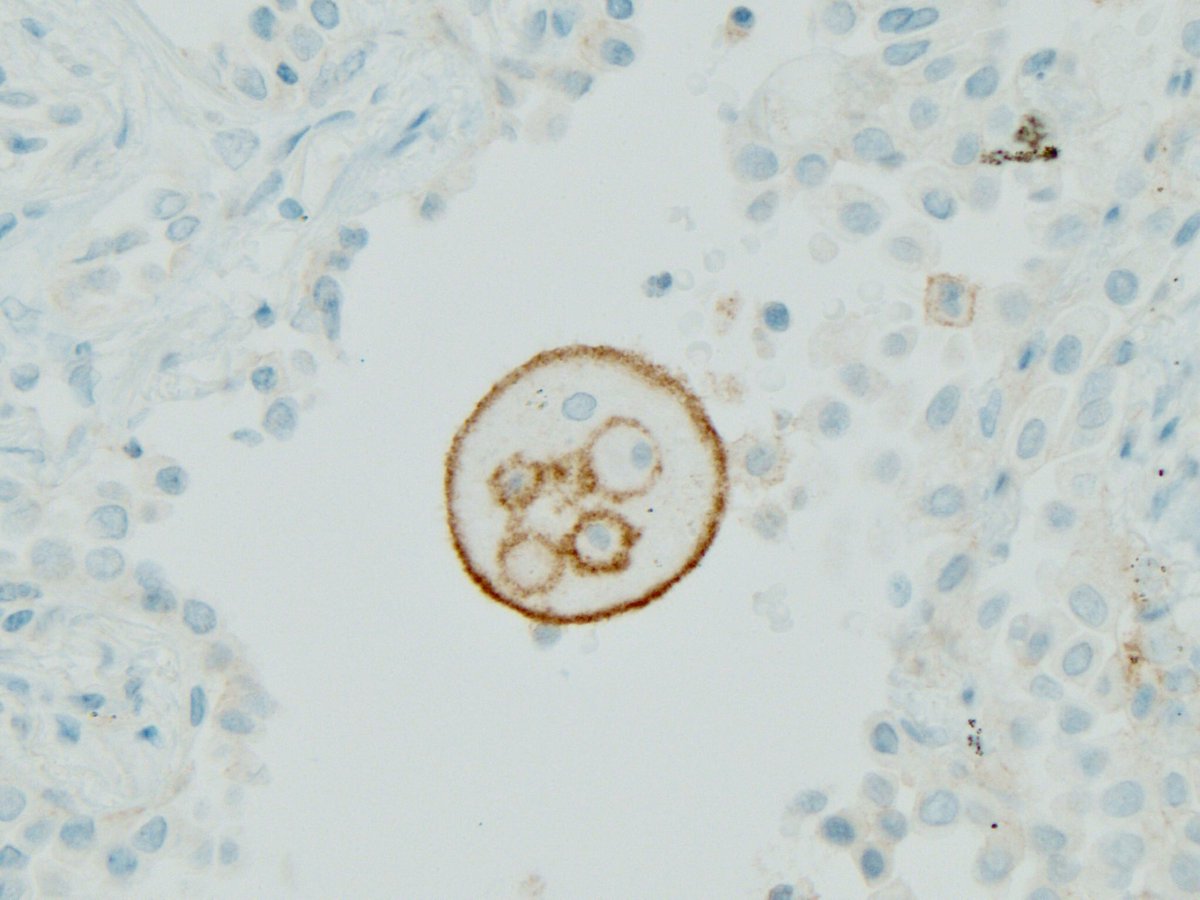
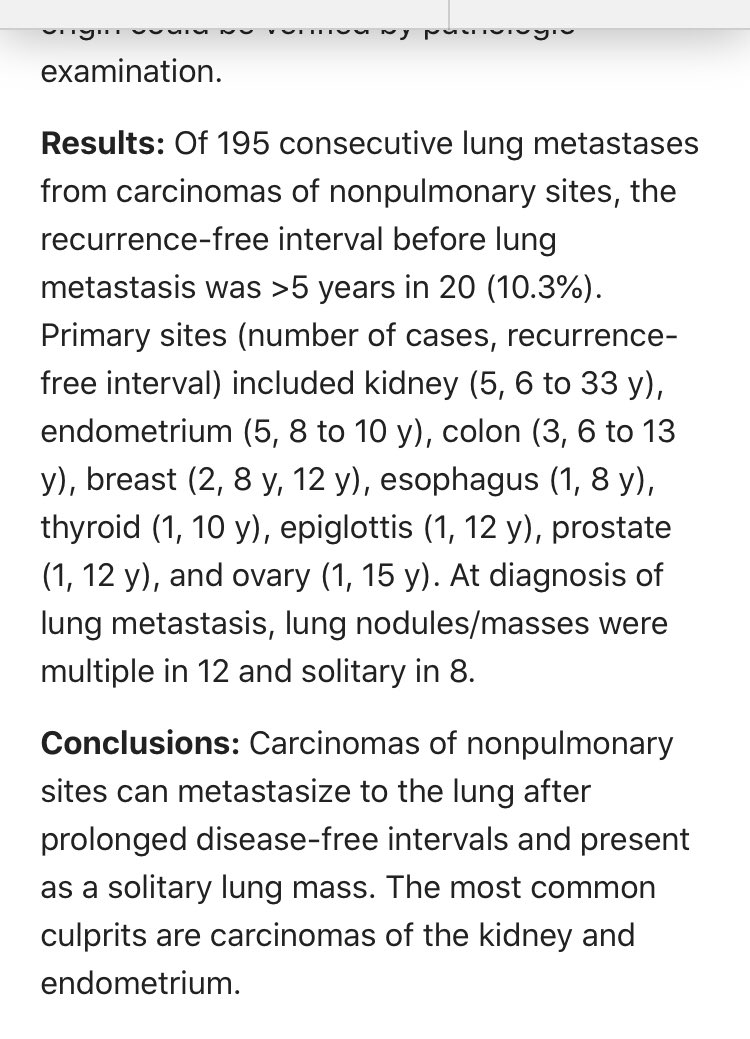
12. What if solitary lung mass & the extrapulmonary cancer was cured long ago? What if your surgeon says “it can’t happen”?
Too bad. Late mets to lung do happen. As long as 33 years later. Especially with RCC and endometrial carcinoma.
pubmed.ncbi.nlm.nih.gov/28248821/
Too bad. Late mets to lung do happen. As long as 33 years later. Especially with RCC and endometrial carcinoma.
pubmed.ncbi.nlm.nih.gov/28248821/
13. The bottom line: history of carcinoma in another site should always be taken seriously.
Use your judgement. Some of these cases will require #ihcpath and some won’t. But always at least consider a met.
Next tweets will address situations without a history of carcinoma...
Use your judgement. Some of these cases will require #ihcpath and some won’t. But always at least consider a met.
Next tweets will address situations without a history of carcinoma...
14. First scenario: no history of carcinoma but miliary bilateral tiny lung nodules. This is rare but does happen (rarely) with papillary thyroid carcinoma.
If you get a lung biopsy with carcinoma in this uncommon situation by all means use #ihcpath
If you get a lung biopsy with carcinoma in this uncommon situation by all means use #ihcpath
15. No history of carcinoma, multiple lung nodules but one dominant nodule or mass: in my experience the vast majority of such cases are primary lung carcinoma with intrapulmonary mets. I don’t do #ihcpath here
You could but your yield for finding mets will be near zero
You could but your yield for finding mets will be near zero
16. This brings us back to the original scenario:
🔥 solitary lung mass
💥 no history of prior carcinoma
I don’t do any #ihcpath here but many people do. What do they find? TTF-1 pos in 80% cases, thus answering a question no one asked
How often do they find mets? Zero.
🔥 solitary lung mass
💥 no history of prior carcinoma
I don’t do any #ihcpath here but many people do. What do they find? TTF-1 pos in 80% cases, thus answering a question no one asked
How often do they find mets? Zero.
17. Many pathologists fear that if they don’t do a TTF-1 an occult primary will be missed. But the clinical protocol in lung cancer mandates PET for staging.
How often do PET scans find an occult primary in the scenario outlined in tweet 16?
Zero.
How often do PET scans find an occult primary in the scenario outlined in tweet 16?
Zero.
18. But surely there is a robust body of literature showing us how often non pulmonary carcinomas present clinically as a solitary lung mass when there is no prior evidence of carcinoma in another organ.
I have asked in public for such a paper for years.
How many are there?
I have asked in public for such a paper for years.
How many are there?
19. But surely in 13 years of practicing lung pathology I must have seen some outliers? Some zebras where an occult thyroid cancer presented as a solitary lung mass. Or colon? Or endometrial? Or renal? Where it came to light after I missed it?
How many such cases have I seen?
How many such cases have I seen?
20. All I hear are occasional anecdotes re: extraordinarily rare zebras without any good documentation that the mass was solitary or that the history of non lung cancer was unknown.
One exchange with my friend @BinXu16 is still with me to this day.
One exchange with my friend @BinXu16 is still with me to this day.
21. In the really excellent series by @BinXu16 , which included 26 years of low risk thyroid cancer at MSKCC there was only 1 case presenting as lung only mets, and it wasn’t specified if this was a solitary nodule. I remain unconvinced.
22. My friend @natasharekhtman posted a case recently showing that morphology is important. But in that case, there WAS a history of endometrial cancer. It was a failure of communication of important info to the pathologist. Not an occult primary.
24. “This is all too confusing” some will say. “I like #ihcpath because it’s more objective.”
These are usually residents, or bright folks with a strong research or basic science background. They believe in objective facts, not fuzzy clinical data or fuzzy supreme H&E.
These are usually residents, or bright folks with a strong research or basic science background. They believe in objective facts, not fuzzy clinical data or fuzzy supreme H&E.
25. These folks like the objective approach:
TTF-1 positive = lung origin
TTF-1 negative = not lung origin
The problem is, neither of these statements are true.
TTF-1 stains thyroid, GYN, even rare colon and breast carcinomas.
Colon by @BinXu16
pubmed.ncbi.nlm.nih.gov/20042854/
TTF-1 positive = lung origin
TTF-1 negative = not lung origin
The problem is, neither of these statements are true.
TTF-1 stains thyroid, GYN, even rare colon and breast carcinomas.
Colon by @BinXu16
pubmed.ncbi.nlm.nih.gov/20042854/
26. More examples of TTF-1 in non lung carcinomas:
Cholangiocarcinoma
pubmed.ncbi.nlm.nih.gov/24418856/
Breast (Juan Rosai)
pubmed.ncbi.nlm.nih.gov/21677546/
Prostate, salivary, colon
pubmed.ncbi.nlm.nih.gov/19887917/
You didn’t know TTF-1 was this “promiscuous”, did you? 😳😢
Cholangiocarcinoma
pubmed.ncbi.nlm.nih.gov/24418856/
Breast (Juan Rosai)
pubmed.ncbi.nlm.nih.gov/21677546/
Prostate, salivary, colon
pubmed.ncbi.nlm.nih.gov/19887917/
You didn’t know TTF-1 was this “promiscuous”, did you? 😳😢
27. What about napsin A? Surely that will solve the problem?
Sorry, napsin A also stains thyroid, RCC and GYN carcinomas especially clear cell carcinomas.
The polyclonal antibody will even stain GI cancers!
Sorry, napsin A also stains thyroid, RCC and GYN carcinomas especially clear cell carcinomas.
The polyclonal antibody will even stain GI cancers!
28. The combination of TTF-1 and napsin A suffers from the same problem: it can be positive in thyroid carcinomas and carcinomas in the GYN tract.
This is where PAX-8 is helpful.
An adenocarcinoma pos for TTF-1 and napsin A but neg for PAX-8 is likely to be from the lung.
This is where PAX-8 is helpful.
An adenocarcinoma pos for TTF-1 and napsin A but neg for PAX-8 is likely to be from the lung.
29. But even if you have the perfect immunophenotype (TTF-1 pos, napsin pos, PAX-8 neg) you still need a lung mass or nodule to complete the picture. No mass in lung, no lung cancer.
Which brings us back to the need for clinical and imaging info. You gotta have it.
Which brings us back to the need for clinical and imaging info. You gotta have it.
30. What’s the value of TTF-1 and napsin A for excluding lung origin?
The frequency of TTF-1 and napsin A in primary lung adenocarcinoma is approximately 80%.
What of the other 20%? Many folks write a comment: “cannot exclude an upper GI or pancreatic primary”
Clinicians:
The frequency of TTF-1 and napsin A in primary lung adenocarcinoma is approximately 80%.
What of the other 20%? Many folks write a comment: “cannot exclude an upper GI or pancreatic primary”
Clinicians:
31. Many pathologists imagine that this comment will cause clinicians to rush to endoscopy or wheel patients into CT (STAT!) to look at the pancreas.
How many times have I seen an occult upper GI or pancreatic primary found this way in the context of a solitary lung mass?
How many times have I seen an occult upper GI or pancreatic primary found this way in the context of a solitary lung mass?
32. All these TTF-1 negative solitary lung masses with no history of cancer are managed as lung cancer. Most clinicians ignore your comment and move on to staging and Rx.
Then what good is the TTF-1 stain in this situation? Positive doesn’t confirm. Negative doesn’t exclude.
Then what good is the TTF-1 stain in this situation? Positive doesn’t confirm. Negative doesn’t exclude.
33. What about other stains? Don’t they help to exclude lung cancer?
Nope.
The list of #ihcpath that can be expressed in lung cancer:
🔥 GATA-3
🔥 CDX-2
🔥 ER
🔥 CA19-9
🔥 CK19
🔥 SALL4
The only exception is strong and diffuse PAX-8
pubmed.ncbi.nlm.nih.gov/28777151/
Nope.
The list of #ihcpath that can be expressed in lung cancer:
🔥 GATA-3
🔥 CDX-2
🔥 ER
🔥 CA19-9
🔥 CK19
🔥 SALL4
The only exception is strong and diffuse PAX-8
pubmed.ncbi.nlm.nih.gov/28777151/
34. But wait! What if we make TTF-1 super sensitive? Then we’ll never miss a single case of lung adenocarcinoma. They will all be pos!
Nope. You will create even bigger problems because this antibody will be super promiscuous. See SP141
Nope. You will create even bigger problems because this antibody will be super promiscuous. See SP141
35. For years we knew SPT24 was worse than 8G7G3/1. Less specific. And then SPT141 came along, and there was a new bad boy in town. You better hire a good lawyer before you use this clone of TTF-1.
36. Or you could buy a combo pack: TTF-1 SP141 plus good lawyer at 20% off!
37. There are also practical issues for clinicians. In a patient with a solitary mass and no cancer history, the pathologist finds strong GATA-3. Does this call for a breast exam?
Should CDX-2 staining prompt a colonoscopy?
Your clinician will say:
Should CDX-2 staining prompt a colonoscopy?
Your clinician will say:
38. There are legitimate uses of TTF-1 in lung biopsies. One of them is to tell whether a poorly differentiated non-small cell carcinoma is adenocarcinoma or sqamous cell carcinoma if you cannot tell by H&E.
The issue is subtyping, not site of origin.
journals.lww.com/ajsp/fulltext/…
The issue is subtyping, not site of origin.
journals.lww.com/ajsp/fulltext/…
38. Finally let me address H&E morphology as a tool for determining site of origin.
We must use it as @natasharekhtman says. If a tumor has papillary structures and psammoma bodies, you gotta think thyroid. But lung cancer can have psammoma bodies & papillary structures too
We must use it as @natasharekhtman says. If a tumor has papillary structures and psammoma bodies, you gotta think thyroid. But lung cancer can have psammoma bodies & papillary structures too
39. If you see clear cells typical of RCC of course you try a PAX-8 stain.
But then you must return to clinical/imaging. No renal mass, no RCC.
You will never be able to sell a solitary lung mass as a met from endometrium without an endometrial mass or history.
But then you must return to clinical/imaging. No renal mass, no RCC.
You will never be able to sell a solitary lung mass as a met from endometrium without an endometrial mass or history.
40. How many solitary lung masses with “odd morphology” must we stain with #ihcpath to find one case with an occult primary? That’s the real question.
One man’s “typical lung cancer” is another man’s “enteric looking”. That’s the problem with morphology.
It’s a good debate!
One man’s “typical lung cancer” is another man’s “enteric looking”. That’s the problem with morphology.
It’s a good debate!
41. I will add to this #Tweetorial as time goes by and other cases are posted. I’m willing to change my mind! 😊
For now, I’ll leave you with the stuff of #ihcpath nightmares. A GYN carcinoma that stains with TTF-1, GATA-3 and calretinin! Sweet dreams!
For now, I’ll leave you with the stuff of #ihcpath nightmares. A GYN carcinoma that stains with TTF-1, GATA-3 and calretinin! Sweet dreams!