THREAD: Are we using ACEIs & ARBs properly? A TI Tweetorial
1/6: British Columbia doctors give 4.5m scripts/year for ACE inhibitors (ACEIs) & angiotensin receptor blockers (ARBs) to control bp. Goal is to ↘️ mortality & morbidity, not simply to ↘️ bp.
#MedEd #hypertension
1/6: British Columbia doctors give 4.5m scripts/year for ACE inhibitors (ACEIs) & angiotensin receptor blockers (ARBs) to control bp. Goal is to ↘️ mortality & morbidity, not simply to ↘️ bp.
#MedEd #hypertension
2/6 BEST EVIDENCE on ARBs & ACEI for #hypertension
3⃣@CochraneHTN systematic reviews:
ACEs v ARBs for htn bit.ly/34vS0hu
BP lowering efficacy of ACEIs for htn bit.ly/30YNIOX
BP lowering efficacy of ACEIs for htn https://t.co/NCl1dfCCAO
#MedEd
3⃣@CochraneHTN systematic reviews:
ACEs v ARBs for htn bit.ly/34vS0hu
BP lowering efficacy of ACEIs for htn bit.ly/30YNIOX
BP lowering efficacy of ACEIs for htn https://t.co/NCl1dfCCAO
#MedEd

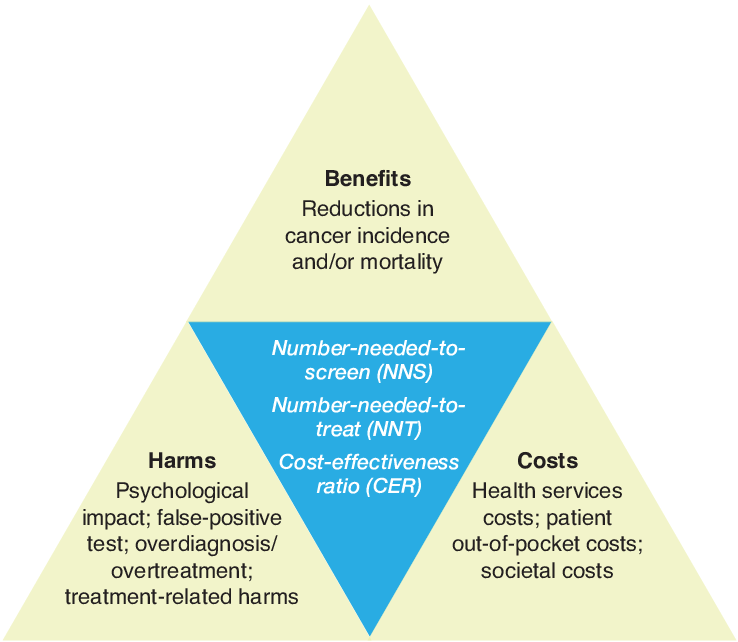
3/6 ACEIs over ARBS when considering HARMS 🤔
Both ACEIs & ARBs ↘️ blood pressure to similar extents.... BUT only ACEIs have evidence for a reduction in risk of morbidity & mortality. So they’d be your first choice 🥇
#MedEd #medsafety #ptsafety
Both ACEIs & ARBs ↘️ blood pressure to similar extents.... BUT only ACEIs have evidence for a reduction in risk of morbidity & mortality. So they’d be your first choice 🥇
#MedEd #medsafety #ptsafety
4/6 LESS IS MORE when #prescribing 💊
Don’t use more than ½ maximum dose of ACEI. ↗️ doses do NOT meaningfully reduce blood pressure further. ½ of max dose of ACEI/ARB produces 90% & 80% of BP lowering of max dose, respectively.
#MedEd #hypertension
Don’t use more than ½ maximum dose of ACEI. ↗️ doses do NOT meaningfully reduce blood pressure further. ½ of max dose of ACEI/ARB produces 90% & 80% of BP lowering of max dose, respectively.
#MedEd #hypertension

5/6 PRICES MATTER 💰💰
As drug classes, ACEIs & ARBs do not differ in blood pressure-lowering efficacy; no individual drug in either category is superior to others. The only known difference is price 🤔
#MedEd #hypertension #drugpricing
As drug classes, ACEIs & ARBs do not differ in blood pressure-lowering efficacy; no individual drug in either category is superior to others. The only known difference is price 🤔
#MedEd #hypertension #drugpricing

6/6 CHECK 💊 PRICES when #prescribing
90% of ACEI scripts in BC are for ramipril & perindopril. Cost can differ btwn equally effective 💊 in same class. In BC, 100 days perindopril 8mg = $65; equivalent ramipril 10mg = $23. Pill-splitting may save 💰, depending on price
#MedEd
90% of ACEI scripts in BC are for ramipril & perindopril. Cost can differ btwn equally effective 💊 in same class. In BC, 100 days perindopril 8mg = $65; equivalent ramipril 10mg = $23. Pill-splitting may save 💰, depending on price
#MedEd
@threadreaderapp unroll, por favor
• • •
Missing some Tweet in this thread? You can try to
force a refresh