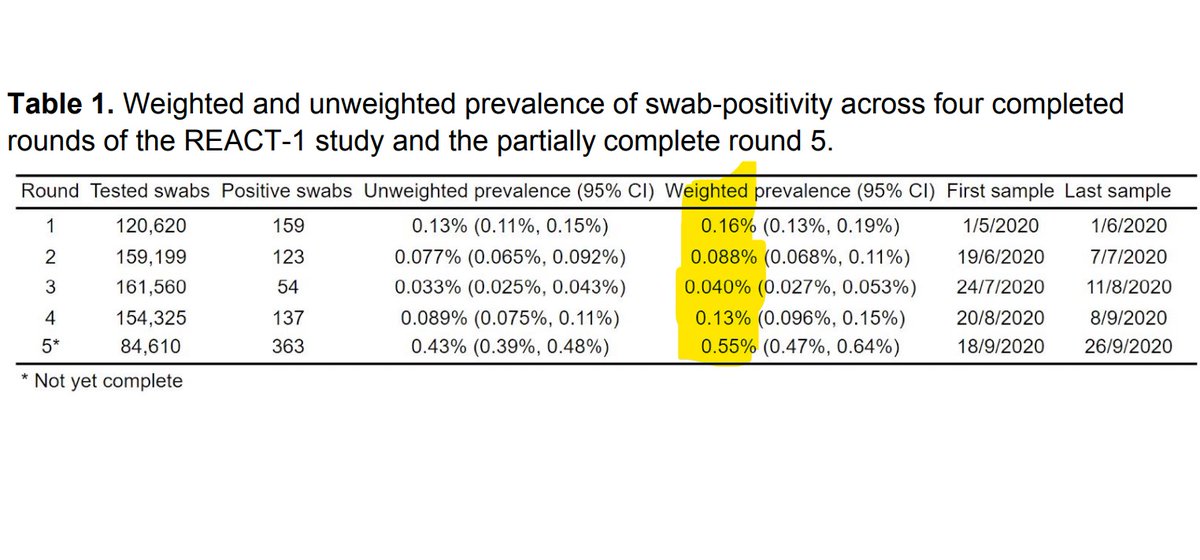
The latest #REACT study by @imperialcollege shows decreasing levels of antibody prevalence. Overall levels fell by 24% over a 12 week period, from 6% to 4.8% in Round 2, and now 4.4%. Let's take a closer look in this short thread. 1/6 

By age the % fall was greatest in the oldest groups, with an increasing trend from age 45. There is some variability though, eg in the data table in the report we see 75+ increased in Rd 3 by 25%, reflecting some wide CI's. 2/6

Showing the wide regional variation, London fell 27% from 13% to 9.5%, whereas at the other end of the spectrum, the SW fell 42% from 2.8% to 1.6%. Note again the increase in Rd 3 for the SW, with a very wide CI for the change we shouldn't read too much into this. 3/6

Those who had the virus worst first time around have much better retention. Those who never had symptoms see falls of 64%, against around 22% for those who knew or suspected they had it. Similarly those in healthcare have much better retention. 4/6
The study discusses the implications for immunity. Whilst noting other factors such as T-cells and memory responses it suggests that this may indicate an overall decline in population immunity. It also notes that the rate of decline may mean we underestimated the first wave. 5/6
Another extensive survey by the REACT team, reflected in the numbers shown. Thanks to all involved at @imperialcollege and its partner organisations for another insightful update. 6/6 ENDS imperial.ac.uk/media/imperial…

• • •
Missing some Tweet in this thread? You can try to
force a refresh