1/
While we're all doom-scrolling through Twitter, I thought I could help provide some distraction for #medtwitter, #dermtwitter & #medstudenttwitter.
A #Derm101 #tweetorial on the #dermatology exam:
REACTION PATTERNS!
AKA: "How a dermatologist approaches a rash!"
pc:@AADskin
While we're all doom-scrolling through Twitter, I thought I could help provide some distraction for #medtwitter, #dermtwitter & #medstudenttwitter.
A #Derm101 #tweetorial on the #dermatology exam:
REACTION PATTERNS!
AKA: "How a dermatologist approaches a rash!"
pc:@AADskin

2/
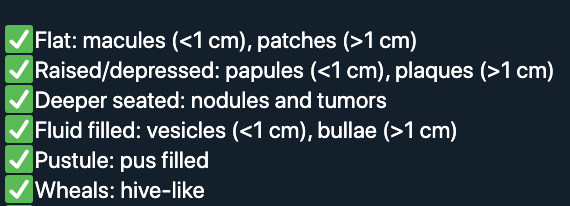
So what exactly is a reaction pattern? It's an organizational way to think about rashes so that we can bucket them. There are FIVE main reaction patterns:
1) Papapulosquamous
2) Eczematous
3) Dermal
4) Vascular
5) Vesicobullous
Which reaction pattern was that last photo?👆
So what exactly is a reaction pattern? It's an organizational way to think about rashes so that we can bucket them. There are FIVE main reaction patterns:
1) Papapulosquamous
2) Eczematous
3) Dermal
4) Vascular
5) Vesicobullous
Which reaction pattern was that last photo?👆
3/
It's PAPULOSQUAMOUS! The name means it's papular (raised) with scale. The prototypical rash for these is psoriasis, which is that 1st photo! Notice how in darker skin, the erythema of psoriasis is harder to see!
Here's a whole #tweetorial I made:
It's PAPULOSQUAMOUS! The name means it's papular (raised) with scale. The prototypical rash for these is psoriasis, which is that 1st photo! Notice how in darker skin, the erythema of psoriasis is harder to see!
Here's a whole #tweetorial I made:
https://twitter.com/DrStevenTChen/status/1245395326237724672?s=20
4/
The ddx for papulosquamous rashes can be quite long. Things like secondary syphilis (pic 1), pityriasis rubra pilaris (pic2 and 3), and lichen planus (pic 4) all fall in this category!
Notice that you need to rely on the rest of your physical exam to further differentiate!
The ddx for papulosquamous rashes can be quite long. Things like secondary syphilis (pic 1), pityriasis rubra pilaris (pic2 and 3), and lichen planus (pic 4) all fall in this category!
Notice that you need to rely on the rest of your physical exam to further differentiate!




5/
Next up, let's talk ECZEMATOUS. This one is a little tricky, because there are three stages of eczema.
1-Acute eczema, with vesicles that leak fluid (pic1).
2-Subacute, dryer, fine scale, fissure (pic2, pc: NEA).
3-Chronic, plaque with hyper-accentuated skin markings (pic3)!
Next up, let's talk ECZEMATOUS. This one is a little tricky, because there are three stages of eczema.
1-Acute eczema, with vesicles that leak fluid (pic1).
2-Subacute, dryer, fine scale, fissure (pic2, pc: NEA).
3-Chronic, plaque with hyper-accentuated skin markings (pic3)!



6/
Remember that "ECZEMA" does not mean atopic dermatitis (AD). Whenever we say someone has eczema, all we're saying is the rash falls in the ECZEMATOUS reaction pattern!
Here's my #tweetorial on AD with more details on that distinction:
Remember that "ECZEMA" does not mean atopic dermatitis (AD). Whenever we say someone has eczema, all we're saying is the rash falls in the ECZEMATOUS reaction pattern!
Here's my #tweetorial on AD with more details on that distinction:
https://twitter.com/DrStevenTChen/status/1229398061845106688?s=20
7/
Next up, DERMAL. I use this term for skin eruptions that are mainly in the dermis or subcutis. Basically not epidermal. Because of that, these rashes usually lack scale, since scale implies there's epidermal involvement.
A good example is granuloma annulare, pictured here:
Next up, DERMAL. I use this term for skin eruptions that are mainly in the dermis or subcutis. Basically not epidermal. Because of that, these rashes usually lack scale, since scale implies there's epidermal involvement.
A good example is granuloma annulare, pictured here:

8/
Another example: erythema nodosum since the inflammation's in subcutis.
Bottom line, no scale, feels deep & indurated, think "DERMAL." Think about what layer the action's in, & maybe what is filling that space (inflammation v. fibrosis v. neoplasia v. edema)!
pc: DFTbubble
Another example: erythema nodosum since the inflammation's in subcutis.
Bottom line, no scale, feels deep & indurated, think "DERMAL." Think about what layer the action's in, & maybe what is filling that space (inflammation v. fibrosis v. neoplasia v. edema)!
pc: DFTbubble

9/
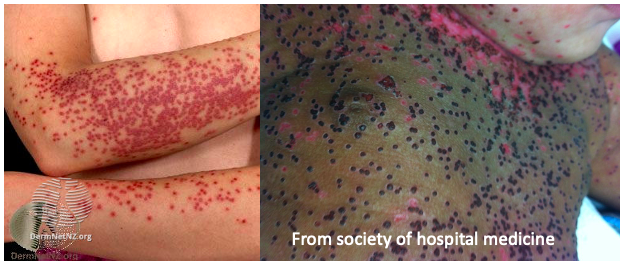
Okay, next up is VASCULAR. This is where the rash appears to be from blockage of vessels. Remember the skin is perfused in cones, so if you block a vessel, circles of skin necrose and you get stellate or RETIFORM edges (see pics). That's why retiform purpura is so worrisome!
Okay, next up is VASCULAR. This is where the rash appears to be from blockage of vessels. Remember the skin is perfused in cones, so if you block a vessel, circles of skin necrose and you get stellate or RETIFORM edges (see pics). That's why retiform purpura is so worrisome!


10/
Remember - retiform purpura, think vasculitis (inflammation in vessel wall) or vasculopathy (blockage of vessel).
But VASCULAR things don't have to cause purpura. What is a common skin eruption you might see that is vascular in pattern, but not permanent?
Remember - retiform purpura, think vasculitis (inflammation in vessel wall) or vasculopathy (blockage of vessel).
But VASCULAR things don't have to cause purpura. What is a common skin eruption you might see that is vascular in pattern, but not permanent?
11/
Livedo reticularis (pic1) is that vascular pattern you might see. It is usually physiologic, but sometimes can be pathologic.
Livedo racemosa (pic2), however, is always pathologic! It's like livedo reticularis but the net is broken! Notice how areas of the net abruptly end!
Livedo reticularis (pic1) is that vascular pattern you might see. It is usually physiologic, but sometimes can be pathologic.
Livedo racemosa (pic2), however, is always pathologic! It's like livedo reticularis but the net is broken! Notice how areas of the net abruptly end!


12/
Okay, VESICOBULLOUS - vesicles or bullae put you in this category.
You might have large tense bullae as those seen in bullous pemphigoid (pic1), or maybe small vesicles seen in eczema herpeticum (pic2)!
Here's my #tweetorial on this reaction pattern
Okay, VESICOBULLOUS - vesicles or bullae put you in this category.
You might have large tense bullae as those seen in bullous pemphigoid (pic1), or maybe small vesicles seen in eczema herpeticum (pic2)!
Here's my #tweetorial on this reaction pattern
https://twitter.com/DrStevenTChen/status/1245802714870591488?s=20

13/
So how do we use this in real life?
If a rash is purely papulosquamous, then you know things in the vesicobullous category probably aren't appropriate for your differential.
But some rashes can be in MULTIPLE categories! Which 2 patterns would you pick for this rash?
So how do we use this in real life?
If a rash is purely papulosquamous, then you know things in the vesicobullous category probably aren't appropriate for your differential.
But some rashes can be in MULTIPLE categories! Which 2 patterns would you pick for this rash?

14/
Here we see tiny vesicles draining fluid, so first, this is VESICOBULLOUS. You might also remember that an acute ECZEMATOUS rash also has tiny vesicles! So since this rash crosses over these two, our differential shifts to the list of eruptions that cross these 2 groups!
Here we see tiny vesicles draining fluid, so first, this is VESICOBULLOUS. You might also remember that an acute ECZEMATOUS rash also has tiny vesicles! So since this rash crosses over these two, our differential shifts to the list of eruptions that cross these 2 groups!
15/
SUMMARY:
✅Reaction patterns help us bucket rashes into one or more of 5 categories.
✅Each category, or each combination of categories can carry its own differential diagnosis.
✅The rest of the skin exam is still critical in arriving at the right diagnosis!
SUMMARY:
✅Reaction patterns help us bucket rashes into one or more of 5 categories.
✅Each category, or each combination of categories can carry its own differential diagnosis.
✅The rest of the skin exam is still critical in arriving at the right diagnosis!
16/16
Thanks for joining me for this #Derm101 #tweetorial! I'm hoping it might've helped distract some of you from the craziness in the world and taught some #dermatology in the process!
In case you prefer a video format of this information, check out 👉
Thanks for joining me for this #Derm101 #tweetorial! I'm hoping it might've helped distract some of you from the craziness in the world and taught some #dermatology in the process!
In case you prefer a video format of this information, check out 👉
• • •
Missing some Tweet in this thread? You can try to
force a refresh