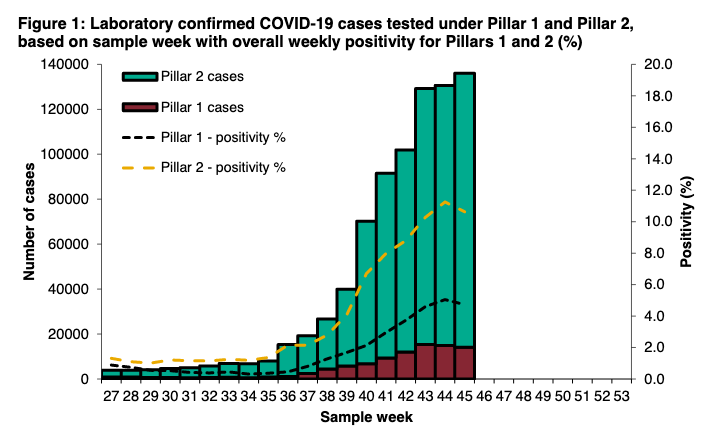
This is v helpful thread from @ScienceShared.
One thing missing is positive predictive and negative predictive values (PPV and NPV) that crucially depend on what proportion of people being tested have disease - the prevalence.
One thing missing is positive predictive and negative predictive values (PPV and NPV) that crucially depend on what proportion of people being tested have disease - the prevalence.
https://twitter.com/ScienceShared/status/1326563891766243329
Take recent ONS survey - 1.1% of pop infected: PPV is 73%, meaning around 1 in 4 positive tests are false positives
(NPV is 99.7% - if you test -ve, you are)
Test 1000 people: there will be 8 true positives, 3 false positives, 3 false negatives, and 986 true negatives.
(NPV is 99.7% - if you test -ve, you are)
Test 1000 people: there will be 8 true positives, 3 false positives, 3 false negatives, and 986 true negatives.
If in NW where prevalence is 2.2%, PPV rises to 84% (about 1 in 6 positive tests are false)
BUT in SE, prevalence is 0.5% meaning PPV is 55%, i.e. every other positive result is a false positive.
BUT in SE, prevalence is 0.5% meaning PPV is 55%, i.e. every other positive result is a false positive.
Of course, PPV will be much higher if you have symptoms, live with a case etc, but otherwise false positives from asymptomatic population screening remain an issue.
So as @ScienceShared says, positive tests in asymptomatic ppl should ideally be repeated or followed up with PCR.
So as @ScienceShared says, positive tests in asymptomatic ppl should ideally be repeated or followed up with PCR.
And of course, as @angelaraffle has elegantly described, there are a whole range of reasons for caution and rigorous evaluation to mitigate unintended harm when it comes to population level screening.
https://twitter.com/angelaraffle/status/1325870626482106370?s=20
Just to complete this thread.
High specificity means number of false +ve basically doesn't change as prevalence rises, but low sensitivity means false -ve⬆️ (where false reassurance comes in).
And the proportion of all positives that are false⬇️ as prevalence⬆️
Table below.
High specificity means number of false +ve basically doesn't change as prevalence rises, but low sensitivity means false -ve⬆️ (where false reassurance comes in).
And the proportion of all positives that are false⬇️ as prevalence⬆️
Table below.
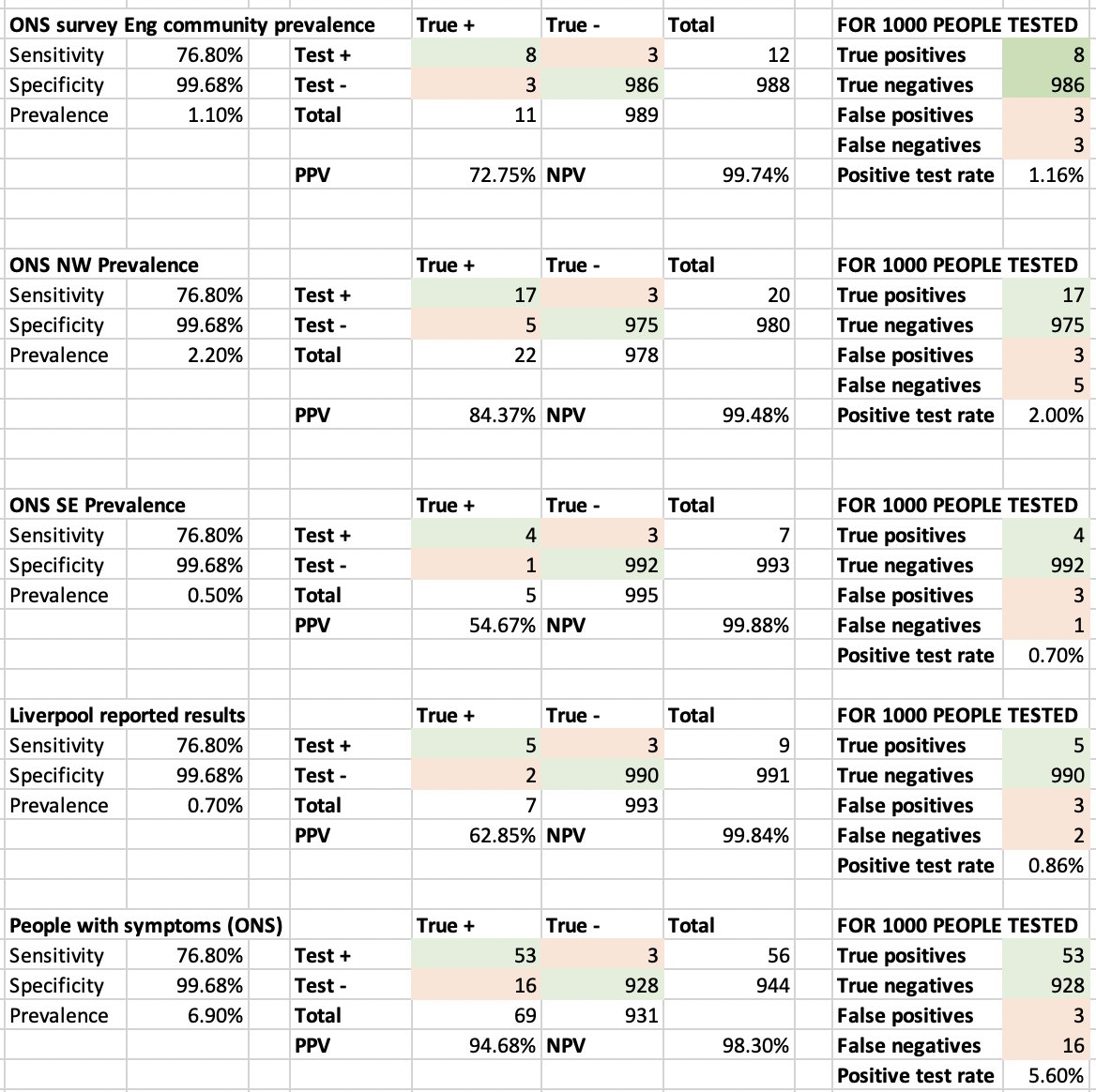
This table is all with the assumptions of the sensitivity and specificity as reported.
So in people with cough or temp or loss of smell, ONS suggests 6.9% test positive. In this group PPV is now 95%, and in every 1000 people get 53 true +ve, 3 false +ve, but 16 false -ve.
So in people with cough or temp or loss of smell, ONS suggests 6.9% test positive. In this group PPV is now 95%, and in every 1000 people get 53 true +ve, 3 false +ve, but 16 false -ve.
+ if these are the sens & spec in Liverpool, a true 0.7% prevalence among those tested would actually detect 9 cases/1000 (so would see a 0.9% prevalence).
So the reported results suggest asymptomatic community prevalence more like 0.5% to give 0.7% of people testing positive.
So the reported results suggest asymptomatic community prevalence more like 0.5% to give 0.7% of people testing positive.
• • •
Missing some Tweet in this thread? You can try to
force a refresh