#Nephrology consult for worsening creatinine in the context of diuresis in a patient with #heartfailure
Documented weight 3 kg ⬇️ than the previous day. No accurate urine output. Pt feels OK (has some unrelated issue).
Question: over diuresis?
#POCUS #MedEd #VExUS see thread 👇
Documented weight 3 kg ⬇️ than the previous day. No accurate urine output. Pt feels OK (has some unrelated issue).
Question: over diuresis?
#POCUS #MedEd #VExUS see thread 👇
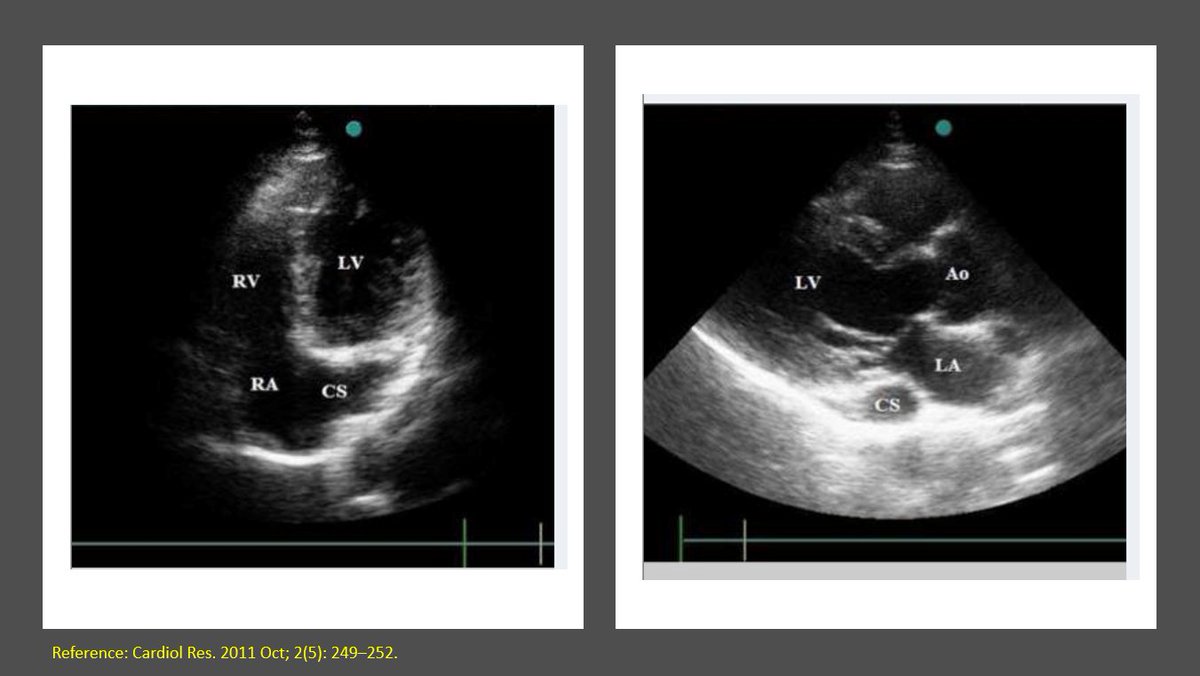
So, there is decreased LV systolic function and obviously diastolic dysfunction. Bi atrial enlargement. No significant pericardial effusion (there was trace on PLAX).
Next step in the hemodynamic circuit #POCUS assessment?
btw repeat weight was similar.
Next step in the hemodynamic circuit #POCUS assessment?
btw repeat weight was similar.
Next: IVC #POCUS assessment to assess right atrial pressure.
Here it is 👇
Big and plethoric (take it as 15 mmHg in a spontaneously breathing person - we get RVSP of ~41 mmHg based on the above tricuspid gradient)
Here it is 👇
Big and plethoric (take it as 15 mmHg in a spontaneously breathing person - we get RVSP of ~41 mmHg based on the above tricuspid gradient)
Is it always big? did it get better from yesterday by any chance?
Need to do #VExUS to know how the organs are feeling congestion.
Start with #VExUSlite of hepatic 👇
red-blue-red-blue 😢
Need to do #VExUS to know how the organs are feeling congestion.
Start with #VExUSlite of hepatic 👇
red-blue-red-blue 😢
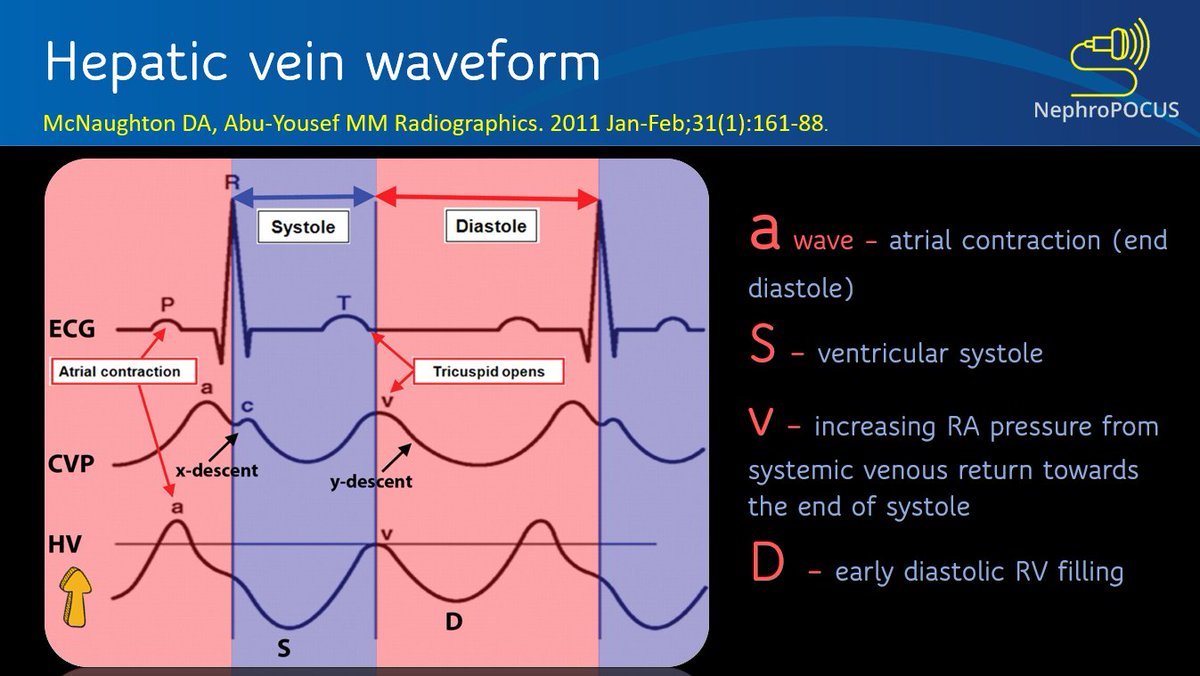
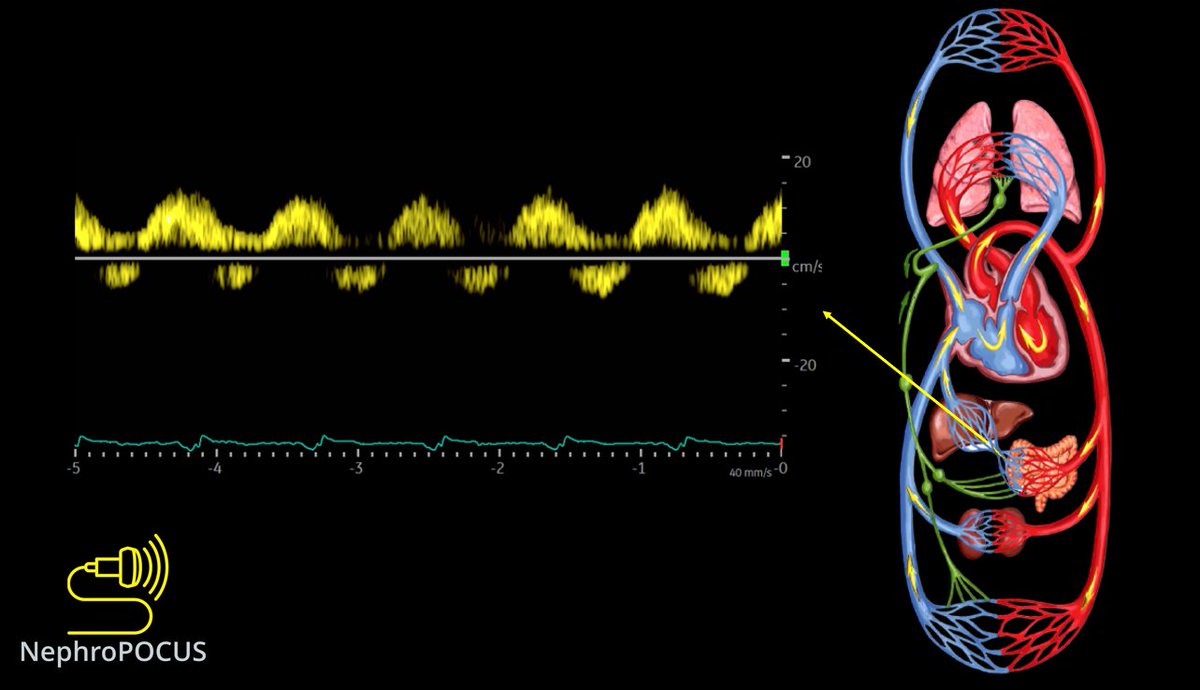
PW #Doppler of hepatic vein
As expected, D-only pattern: systolic flow reversal and venous return only during diastole. Finally have EKG (though gain not optimized)
As expected, D-only pattern: systolic flow reversal and venous return only during diastole. Finally have EKG (though gain not optimized)

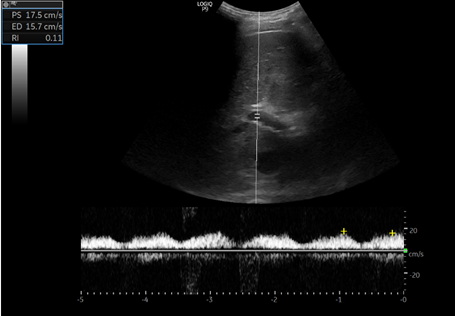
Now #POCUS #VExUSlite of portal vein
[first you'll see hepatic veins and the clip transitions to portal]
Am I seeing some blue color? then its not good....(systolic flow reversal). Let's confirm it in PW mode
[first you'll see hepatic veins and the clip transitions to portal]
Am I seeing some blue color? then its not good....(systolic flow reversal). Let's confirm it in PW mode
100% pulsatile with systolic flow reversal as expected. Note that the reversal corresponds to the little blue sparkle seen on color #POCUS
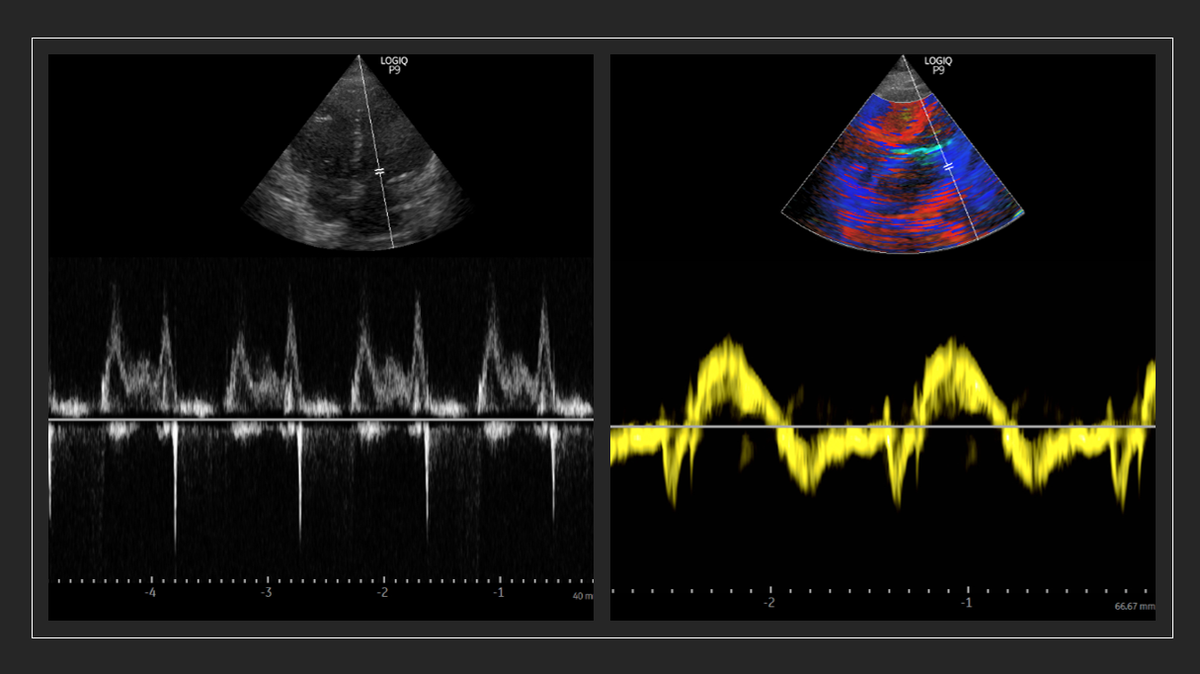
Now its intra-renal vein's turn #VExUS
Clear monophasic (diastole-only) flow pattern
Even that diastolic flow is little unlike the recent case we saw where it was spanning throughout the diastole.
That means the venous stasis index is very low = severe congestion
Clear monophasic (diastole-only) flow pattern
Even that diastolic flow is little unlike the recent case we saw where it was spanning throughout the diastole.
That means the venous stasis index is very low = severe congestion

What should we do now? fluids because the weight dropped? 🙄
Point I'm making: #POCUS #VExUS (= physical examination) is very important in day-to-day #nephrology & any specialty. Why rely on indirect methods when you can see the anatomy at patient's bedside without radiation 🤦
Point I'm making: #POCUS #VExUS (= physical examination) is very important in day-to-day #nephrology & any specialty. Why rely on indirect methods when you can see the anatomy at patient's bedside without radiation 🤦
In this case, repeat weight was almost unchanged - so the previous weight was likely wrong. Another interesting point.
Cc some #VExUS allies @khaycock2 @ThinkingCC @ArgaizR @katiewiskar @OKiamanesh @Scottiedoc1 @BillyBam28er @DrBaudy @KalagaraHari
Cc some #VExUS allies @khaycock2 @ThinkingCC @ArgaizR @katiewiskar @OKiamanesh @Scottiedoc1 @BillyBam28er @DrBaudy @KalagaraHari
• • •
Missing some Tweet in this thread? You can try to
force a refresh