1/
WHERE does ascites come from?
HOW do diuretics treat ascites?
ARE you ready for a #tweetorial?
#livertwitter #medtwitter #MedEd
WHERE does ascites come from?
HOW do diuretics treat ascites?
ARE you ready for a #tweetorial?
#livertwitter #medtwitter #MedEd

2/
First, ascites is:
1⃣Fluid in the belly
2⃣Awful
3⃣A cruel trick the liver plays on the heart and kidney
Throw back to my "what is #cirrhosis?" tweetorial
First, ascites is:
1⃣Fluid in the belly
2⃣Awful
3⃣A cruel trick the liver plays on the heart and kidney
Throw back to my "what is #cirrhosis?" tweetorial
https://twitter.com/ebtapper/status/1185513443199246336?s=20

3/
The first 'lesion' in ascites formation is the fibrotic liver.
Fibrotic liver:
⬆️sinusoidal hydrostatic pressure
⬆️lymph formation
"Mo sinusoidal pressure, mo lymph"
- Ernest H. Starling MD, personal communication
The first 'lesion' in ascites formation is the fibrotic liver.
Fibrotic liver:
⬆️sinusoidal hydrostatic pressure
⬆️lymph formation
"Mo sinusoidal pressure, mo lymph"
- Ernest H. Starling MD, personal communication

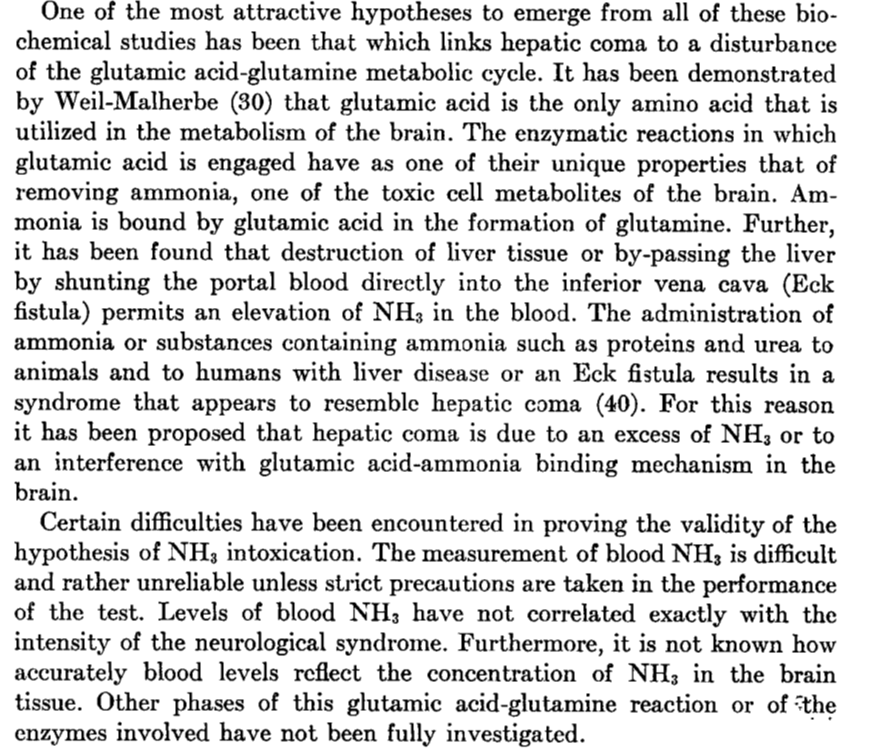
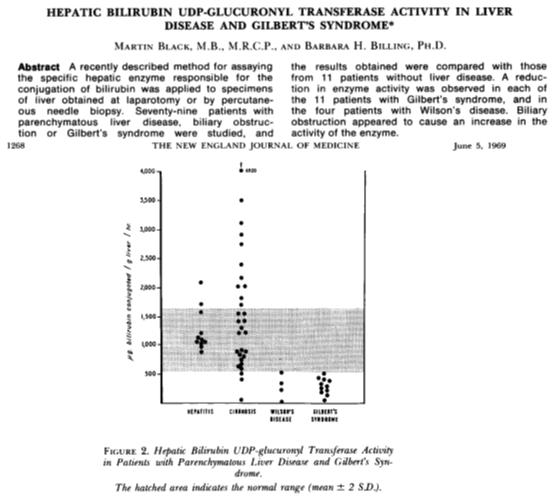
4/
Lymph production in #cirrhosis is:
1⃣Proportional to portal pressure
2⃣Massive. Nearly 10 times normal
Thoracic duct flow goes from 120cc/hr to up to 1.2L/hr!
😀Fig2: Splenorenal shunt surgery ⬇️lymph production
🥸Fig3: Drain the thoracic duct & eliminate ascites
Lymph production in #cirrhosis is:
1⃣Proportional to portal pressure
2⃣Massive. Nearly 10 times normal
Thoracic duct flow goes from 120cc/hr to up to 1.2L/hr!
😀Fig2: Splenorenal shunt surgery ⬇️lymph production
🥸Fig3: Drain the thoracic duct & eliminate ascites



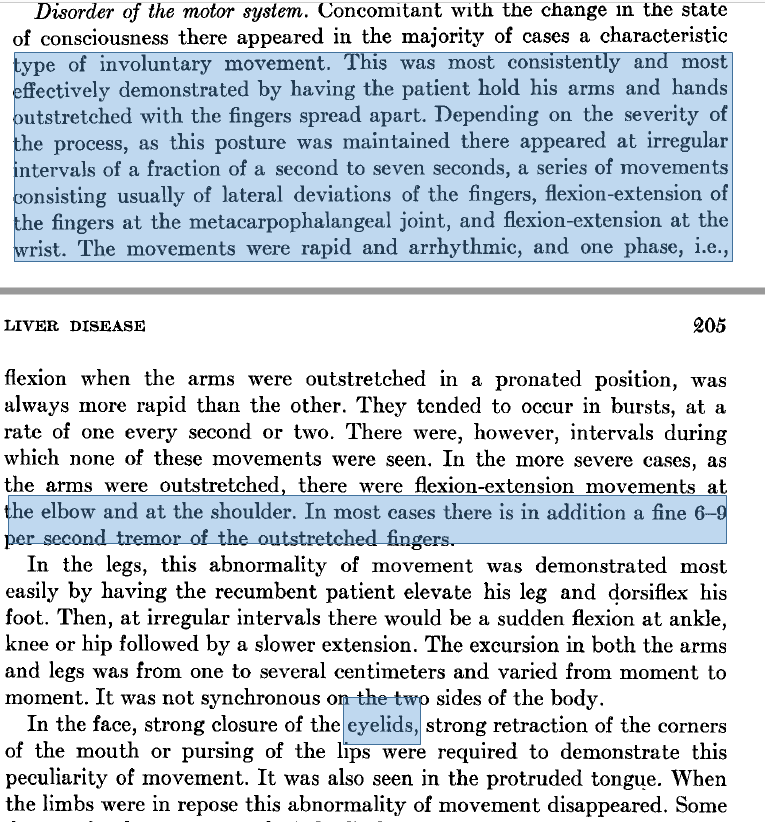
5/
As portal hypertension worsens (as the HVPG rises past 10mmHg), the lymphatics are stressed, then overwhelmed, and ascites develops
As portal hypertension worsens (as the HVPG rises past 10mmHg), the lymphatics are stressed, then overwhelmed, and ascites develops


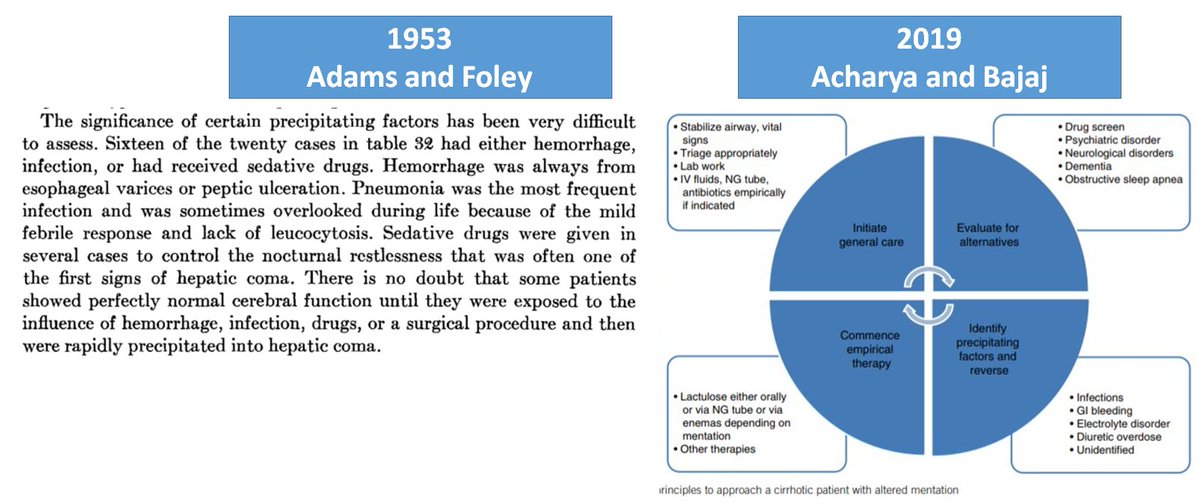
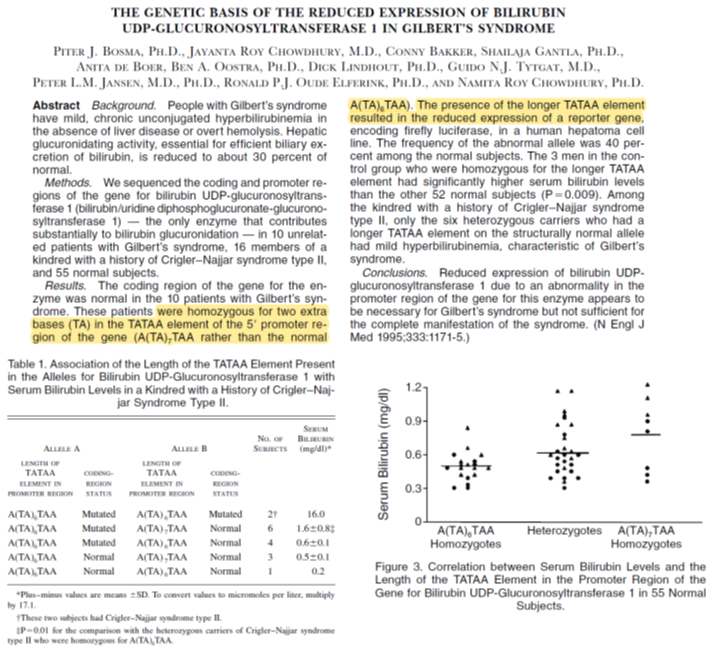
6/
But WHERE does the ascites actually come from?
The weeping liver!
Check this 1955 paper out:
Method: clamped IVC in dogs
Result: Ascites beaded on the liver surface. Covering the liver with a bag collects all the ascites, keeps the gut dry
But WHERE does the ascites actually come from?
The weeping liver!
Check this 1955 paper out:
Method: clamped IVC in dogs
Result: Ascites beaded on the liver surface. Covering the liver with a bag collects all the ascites, keeps the gut dry

7/
Hold up!
We dont yet understand where the extra fluid is coming from
The secret lies between two seemingly conflicting facts:
People with #cirrhosis and ascites have:
1. Peripheral fluid overload
2. Low central blood volume
Hold up!
We dont yet understand where the extra fluid is coming from
The secret lies between two seemingly conflicting facts:
People with #cirrhosis and ascites have:
1. Peripheral fluid overload
2. Low central blood volume
8/
The reason for low central blood volume in #cirrhosis:
1⃣Despite ⬆️lymph return, 🫀is underfilled
2⃣All the blood is trapped in vasodilated gut arteries
3⃣Arterial vasodilation is proportional to disease severity
The reason for low central blood volume in #cirrhosis:
1⃣Despite ⬆️lymph return, 🫀is underfilled
2⃣All the blood is trapped in vasodilated gut arteries
3⃣Arterial vasodilation is proportional to disease severity



9/
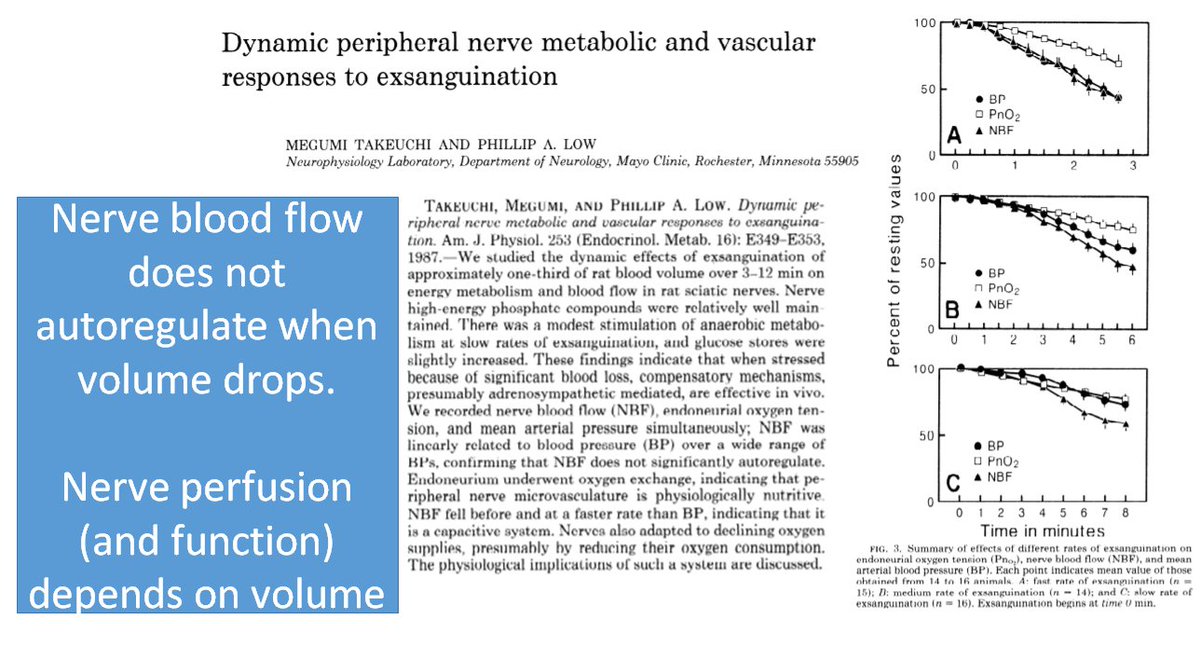
If blood is trapped, return to the heart is low, and so is delivery to the pesky kidney
As a result:
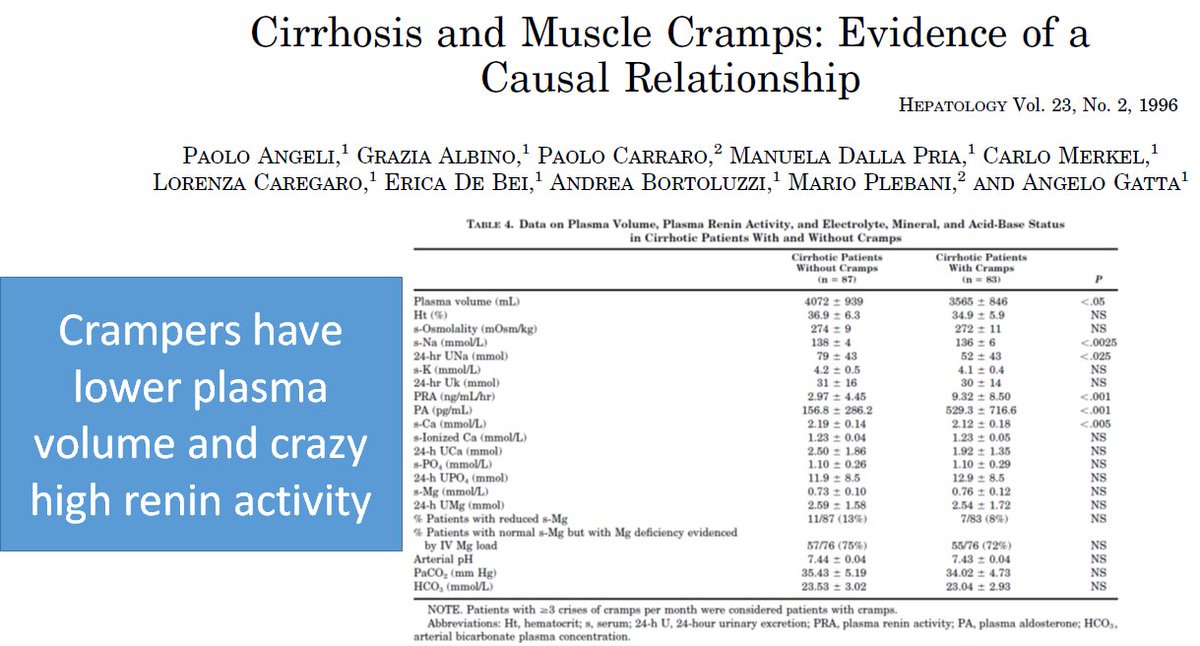
1⃣ALL THE TOOLS are revved: Renin, aldosterone, ADH, norepi
2⃣Renal tubules respond: sodium & free H20 excretion plummets
3⃣Plasma volume increases
If blood is trapped, return to the heart is low, and so is delivery to the pesky kidney
As a result:
1⃣ALL THE TOOLS are revved: Renin, aldosterone, ADH, norepi
2⃣Renal tubules respond: sodium & free H20 excretion plummets
3⃣Plasma volume increases


10/
Interim summary:
#cirrhosis
+ Portal hypertension
+ Arterial vasodilation
+ ⬆️plasma volume
+ Starling forces
= Ascites
QED
Interim summary:
#cirrhosis
+ Portal hypertension
+ Arterial vasodilation
+ ⬆️plasma volume
+ Starling forces
= Ascites
QED

11/
NOW
how do diuretics work?
1⃣The peritoneum absorbs 0.5-1L/day
2⃣Diuretics do NOT speed this up
3⃣Diuretics drop plasma volume!
NOW
how do diuretics work?
1⃣The peritoneum absorbs 0.5-1L/day
2⃣Diuretics do NOT speed this up
3⃣Diuretics drop plasma volume!



12/
1⃣Diuretics work by Starling forces!
They⬇️pressure gradient between portal & hepatic veins (HVPG)
How?
2⃣They drop HVPG proportional to⬇️plasma volume
How?
3⃣Spironolactone addresses the cause: high aldo
1⃣Diuretics work by Starling forces!
They⬇️pressure gradient between portal & hepatic veins (HVPG)
How?
2⃣They drop HVPG proportional to⬇️plasma volume
How?
3⃣Spironolactone addresses the cause: high aldo



13/
Final summary
1⃣Ascites=a trick the liver plays on the 🫀/kidney
2⃣Sinusoidal htn⬆️⬆️lymph production
3⃣Arterial vasodilation traps blood in the gut
4⃣Cardiac return suffers
5⃣RAAS en fuego
6⃣⬆️Plasma volume
7⃣Ascites forms
8⃣Diuretics⬇️plasma volume; spiro⬇️RAAS
Final summary
1⃣Ascites=a trick the liver plays on the 🫀/kidney
2⃣Sinusoidal htn⬆️⬆️lymph production
3⃣Arterial vasodilation traps blood in the gut
4⃣Cardiac return suffers
5⃣RAAS en fuego
6⃣⬆️Plasma volume
7⃣Ascites forms
8⃣Diuretics⬇️plasma volume; spiro⬇️RAAS

/End
This concludes a #tweetorial on ascites formation/treatment. Thank you for reading. I hope you enjoyed.
🙏to @jaumebosch9 and @BloomPringle for their input
If interested, please see below for my 'ascites' menu
This concludes a #tweetorial on ascites formation/treatment. Thank you for reading. I hope you enjoyed.
🙏to @jaumebosch9 and @BloomPringle for their input
If interested, please see below for my 'ascites' menu

Correction in the first figure: "Total blood volume is high" is correct. But that is addressed in the next tweet. This figure shows that central blood volume is low, proportional to portal pressure.
• • •
Missing some Tweet in this thread? You can try to
force a refresh