1/ I really want to highlight how this #COVID19 graph from @KCMOHealthDept is a masterclass in either incompetence, narrative-spinning, or both. This is a bit niche with it being KC but I think it applies to health depts across the US. This is lying with graphs at its finest. 
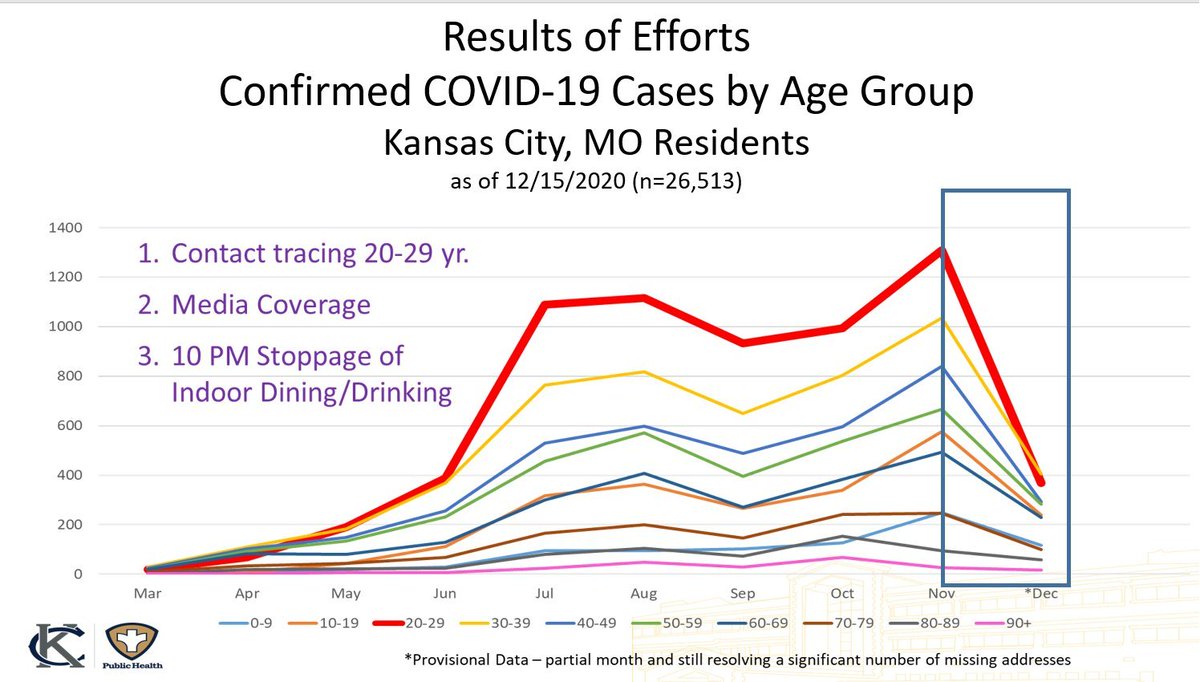
2/ First, the graph itself. They have it broken out as cumulative counts per month, as of 12/15. December is half over, so you can't compare it to other months, yet they highlight how far cases have fallen in all groups since November with a tiny blink-and-you-miss-it disclaimer.
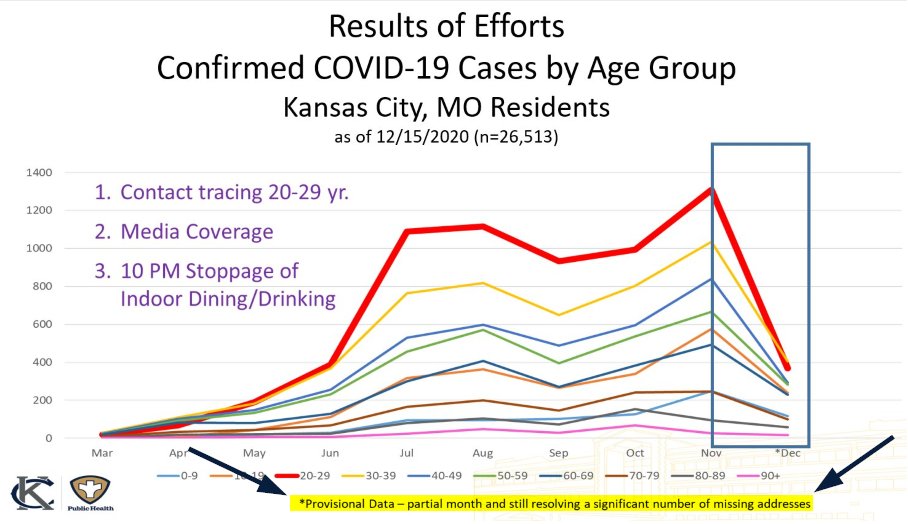
3/ They wouldn't be wrong in assuming cases will be down in December though. But their argument falls apart when they credit 10 PM bar closures for the decline. The curfew was announced 11/16. Cases peaked 11/10 - 20 DAYS before we would see any meaningful effect from the curfew.
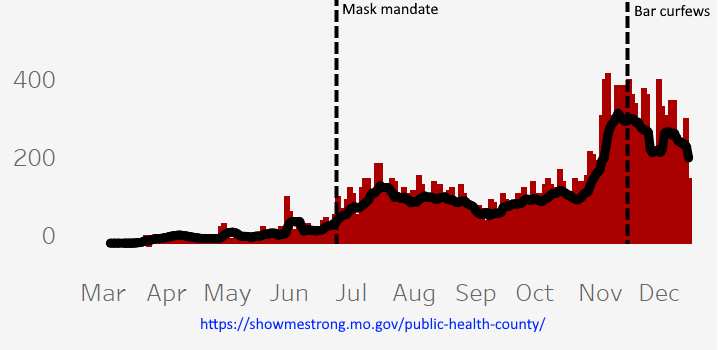
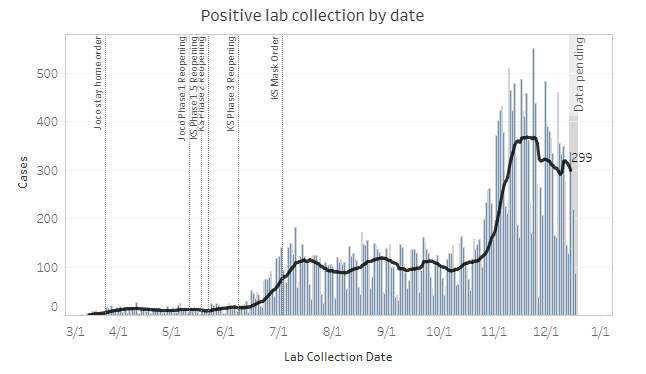
4/ Johnson County, KS, which is just across the state line from Kansas City, also imposed a curfew just as cases peaked, so the timelines don't add up there either. The kicker is that their curfew was midnight - so I guess bars could've been open here in KC for another two hours.
5/ They also credit contact tracing, but to date they have not provided a single data point of how many cases can be traced to restaurants or bars. For reference, NY's large-scale contact tracing program could only trace 1.4% to restaurants and bars.
6/ Last week when asked how many cases could be traced to bars, @QuintonLucasKC deflected the question and said "40% of cases can be traced to 20-30 year olds", which...doesn't answer the question. It's been 9 months. They'll likely never answer it.
https://twitter.com/FactsVs0pinion/status/1338164615499354113?s=20
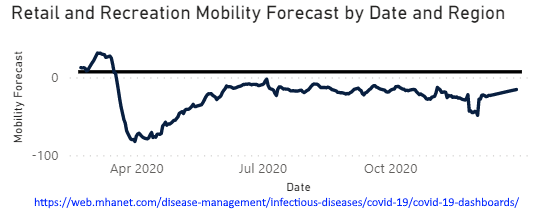
7/ The health dept credits "media coverage", which anyone who lives in Kansas City knows has been sky-is-falling apocalyptic for months now. They imply media coverage has changed citizens' behavior - yet mobility has been at roughly the same level (20% below baseline) since July.
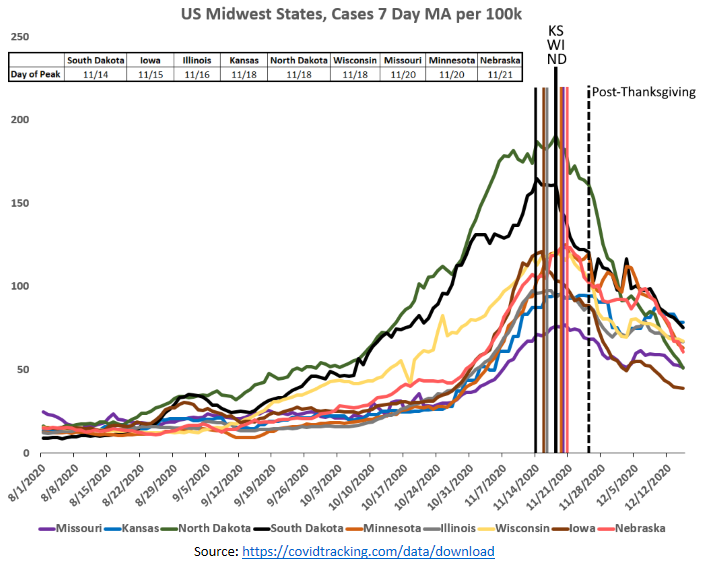
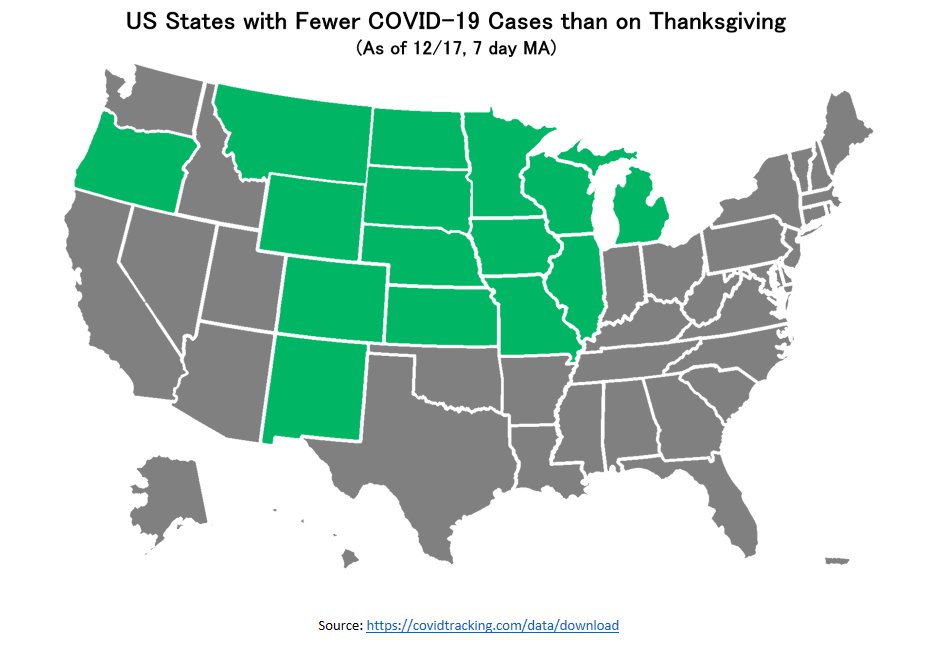
8/ Finally, to my point yesterday, it appears @QuintonLucasKC, @RexArcherMD and the @KCMOHealthDept live in a bubble - all the states surrounding MO peaked within one week of each other - even South Dakota, which peaked first. (Cases here are from date of report vs. occurrence)
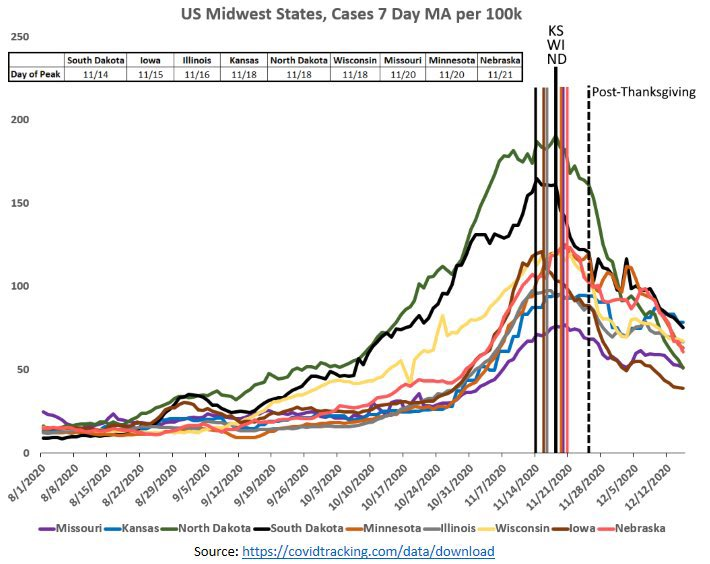
9/ This is the narrative they have to push out of self-preservation. If they admitted these outbreaks are seasonal/regional, which is clear, then they'd also have to admit their disastrous policies that disproportionately affect low-income families were largely for nothing.
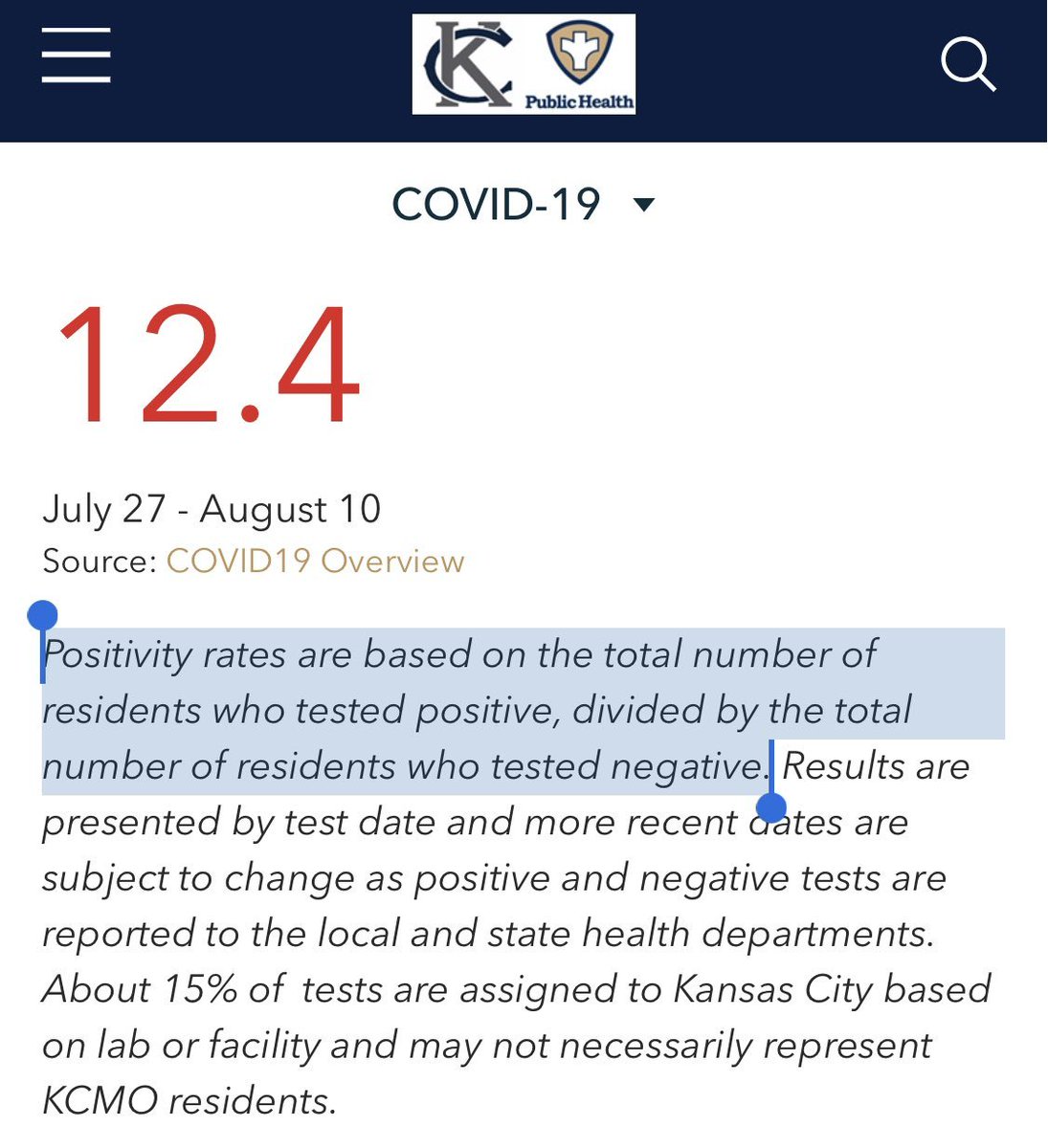
10/ But hey, maybe my standards are just too high. This is the same health department that poured bleach in soup intended for the homeless (look it up) and thought THIS was how you calculate percent positive rate. It was on their official dashboard for months.
• • •
Missing some Tweet in this thread? You can try to
force a refresh