THREAD: Spent the past 2 days co-designing & testing the #CovidVaccine administration process @UnityHealthTO using #simulation informed #design.
A huge multi-disciplinary effort coordinated by @Sim_StMikes. cc: @IrfanDhalla
Here's some insights into the process
1/
A huge multi-disciplinary effort coordinated by @Sim_StMikes. cc: @IrfanDhalla
Here's some insights into the process
1/

2/ Why does it matter? Somewhat self evident, but we want to design & test a process that optimizes the number of people who be vaccinated while also ensuring a pleasant & safe experience
Great clip from "the Founder"... example of design #simulation
Great clip from "the Founder"... example of design #simulation
3/ We began with core objectives/principles for the project.
This informed the blueprints for the design of the space
But we all know, things may look good on paper, but don't necessarily translate to real-life
More importantly, people's behavior can be difficult to predict
This informed the blueprints for the design of the space
But we all know, things may look good on paper, but don't necessarily translate to real-life
More importantly, people's behavior can be difficult to predict
4/ We began with a modified "pluralistic walkthrough"
bit.ly/38n10aC - users/experts/designers step-by-step work through usability issues with dialog elements
We modified the process to enhance the user-experience, optimize safety while reducing confusion points
bit.ly/38n10aC - users/experts/designers step-by-step work through usability issues with dialog elements
We modified the process to enhance the user-experience, optimize safety while reducing confusion points

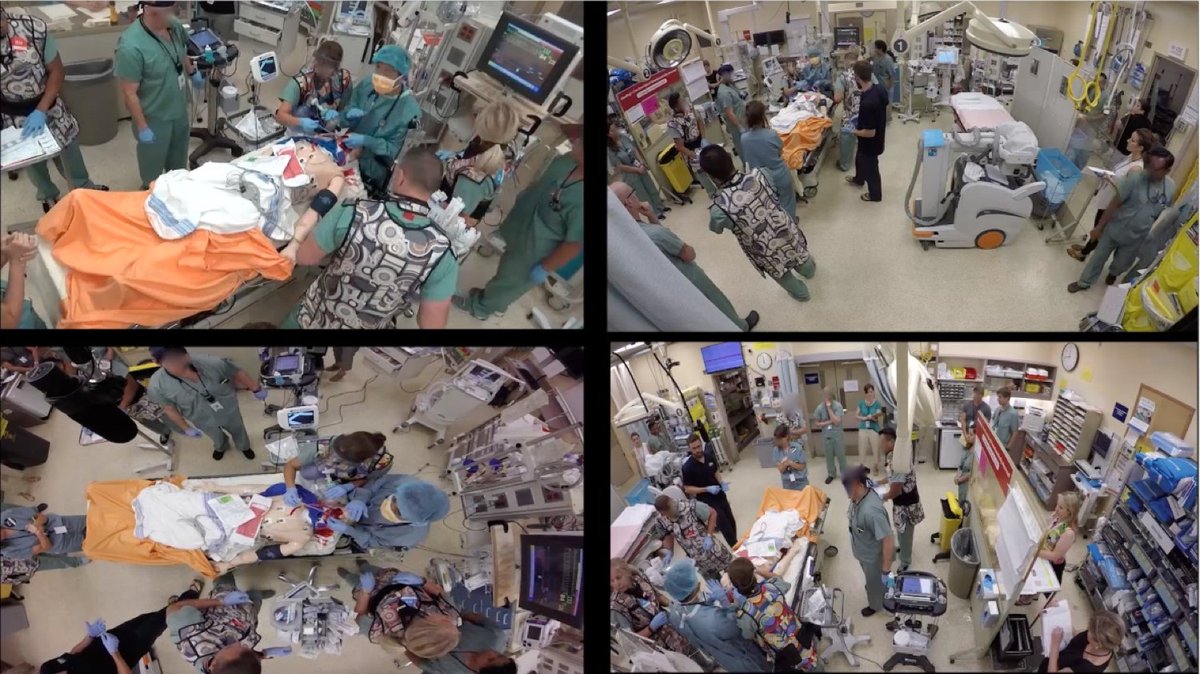
5/ The following day with a more finalized set of steps participants moved through the process in real time. Each step was timed to accurately establish time from registration to vaccination to exit
Rapid cycling simulation resulted in immediate changes to improve the process.
Rapid cycling simulation resulted in immediate changes to improve the process.




6/ These iterative changes have allowed us to rapidly modify the design of our space, add user-centered design features and increase efficiency.
We've tested multiple scenarios and potential challenges that may arise - each now has specifically designed mitigation strategies
We've tested multiple scenarios and potential challenges that may arise - each now has specifically designed mitigation strategies
7/ When we begin vaccination this week, we're confident our process will be both safe and efficient while taking into account the importance of the human experience.
#crushcovid
#crushcovid

• • •
Missing some Tweet in this thread? You can try to
force a refresh