For those following #ACIP vaccine prioritization debate - proposal to have 75+ alongside frontline workers in phase 1B is interesting, and different from prior discussion. But there are still pitfalls with any age cutoff, whether 75 or 65, as I explained in a comment to ACIP /1
https://twitter.com/HelenBranswell/status/1340698200882229250
Down Syndrome deaths are disparately high and happen before 75. 54%, 61%, and 69% of Black, Hispanic, and AI/AN deaths (respectively) happen before 75. I haven't seen US data on income x age at death, but a similar gradient is plausible, and may help explain the race data. /2 

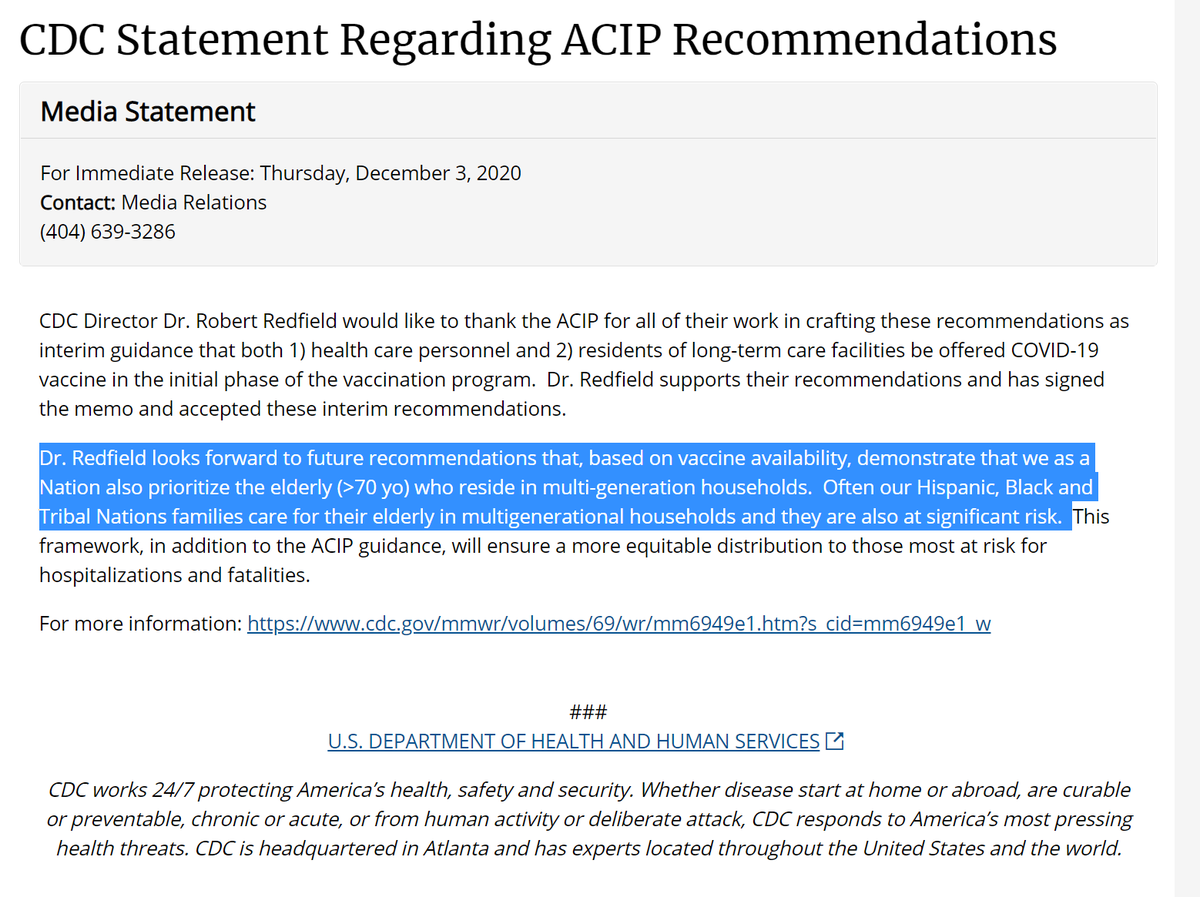
So I continue to think #ACIP should encourage states & localities to look at overlapping risk factors like housing+age as LTCF priority did and @CDCDirector suggested, rather than using age cutoffs that sweep in ppl at very different risk & exclude some
https://twitter.com/DrTomFrieden/status/1340131768217825287/3

Also, as i pointed out to a Twitter luminary yesterday, the public cares about a lot of different values--and doesn't want grocery workers or teachers or ppl w Down Syndrome going behind all people of a given age /4
https://twitter.com/GovindPersad/status/1340504698504146944?s=20
(If you're wondering why I didn't sign up to give an oral public comment: I did. The ACIP comment lottery didn't pick me. It did pick my co-author, a doc/MPH who'd have been great. But she couldn't answer the email in time-pitfall of allocation-& seems to have lost her spot.) /5
One more thought about how #ACIP could still do better at framework of aligning rather than conflicting values:
https://twitter.com/GovindPersad/status/1340723366987108352?s=20/6
• • •
Missing some Tweet in this thread? You can try to
force a refresh