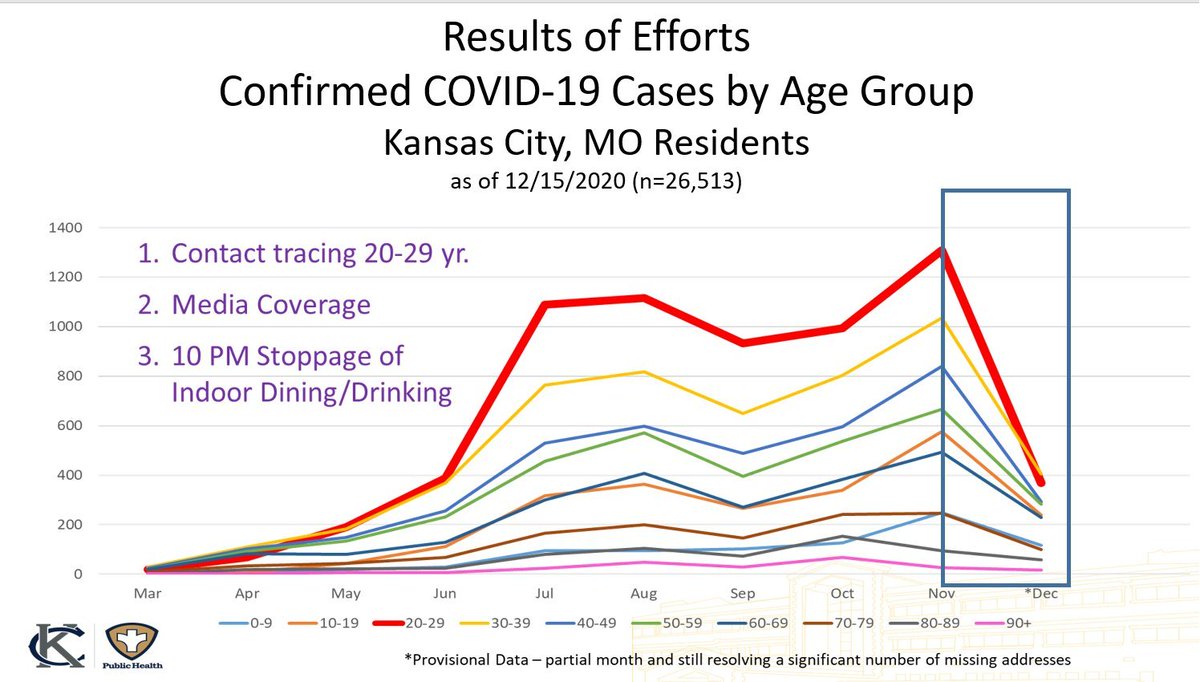
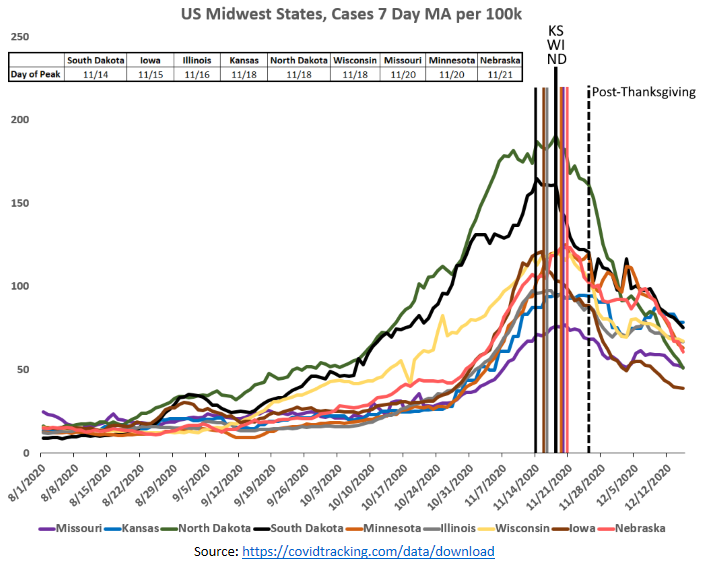
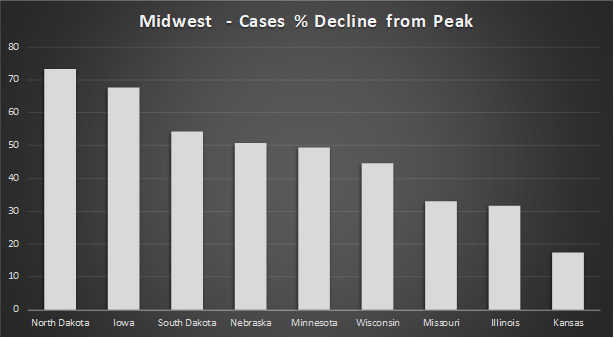
Tom claims COVID spread is entirely because of noncompliance with COVID measures, but he’ll never explain how 9 Midwest states peaked within one week of each other despite having completely different COVID policies, or how South Dakota managed to be the first to peak among them 
https://twitter.com/DrTomFrieden/status/1347711454816989185

Tom just hand-waves California’s terrible COVID numbers with “places in CA haven’t masked and distanced”. Really? Where? When? How? Do you have studies? Anything? California has some of the highest mask compliance numbers in the country. Can you be more specific, @DrTomFrieden?
https://twitter.com/DrTomFrieden/status/1347711484940398594
If Tom were actually scientifically-minded he’d show a real interest in how California continues to spike despite having very drastic measures, or how all these Midwest states follow the exact same trajectory. That can’t be explained by 40 million people all complying at once.

Seriously, I don’t think @DrTomFrieden has the words “seasonality” or “regionality” in his vocabulary. To him, everything is because of opening too soon or noncompliance with public health measures. Does he truly believe this, or is he lying and thinks people are that stupid?
https://twitter.com/drtomfrieden/status/1347711472282046473
Or, the third, and probably most likely option - Tom is the President and CEO of an organization that specifically relies on the idea that these measures are highly effective, and will do everything in his power to try to prove people need his organization to help implement them

Making $400,000 a year on this type of grift would definitely make a guy want to ensure they have that job security
https://twitter.com/EWoodhouse7/status/1347932661935988738
And, of course there’s also this abcnews.go.com/US/cdc-directo…
• • •
Missing some Tweet in this thread? You can try to
force a refresh