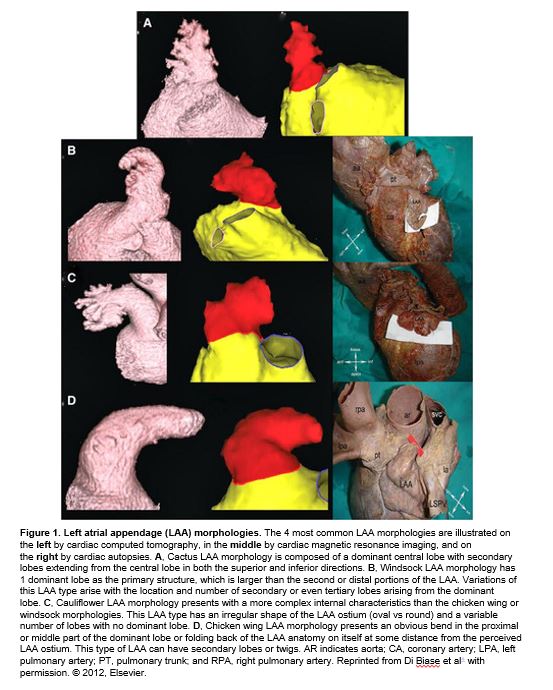
⁉️Did you know the left atrial appendage can be described as chicken wing🍗, cactus 🌵, windsock, & cauliflower morphology⁉️
Full 🧵on 💘Atrial Fibrillation💘
🎧RTL Ep. 23: bit.ly/3b6svs0
Thanks to @Gurleen_Kaur96 for this week's tweetorial!
Full 🧵on 💘Atrial Fibrillation💘
🎧RTL Ep. 23: bit.ly/3b6svs0
Thanks to @Gurleen_Kaur96 for this week's tweetorial!
https://twitter.com/i/status/1352757712472436737
🥇First, let's review the basics of atrial fibrillation (A.fib)
✨Most common cardiac arrhythmia✨
Etiology:
-🎆Rapid firing from foci in pulmonary vein triggers reentrant waves🎆
EKG:
-RR intervals have no pattern ➡️ irregularly irregular
-No distinct P waves
✨Most common cardiac arrhythmia✨
Etiology:
-🎆Rapid firing from foci in pulmonary vein triggers reentrant waves🎆
EKG:
-RR intervals have no pattern ➡️ irregularly irregular
-No distinct P waves


An aside on terminology 📅:
🔹Paroxysmal: self-terminated in < 7 days
🔹Persistent: > 7 days or need cardioversion
🔹Long-standing persistent: > 1 year
🔹Permanent: no attempt to restore/maintain sinus rhythm
🔹A.fib with rapid ventricular response (RVR): >110-120 bpm
🔹Paroxysmal: self-terminated in < 7 days
🔹Persistent: > 7 days or need cardioversion
🔹Long-standing persistent: > 1 year
🔹Permanent: no attempt to restore/maintain sinus rhythm
🔹A.fib with rapid ventricular response (RVR): >110-120 bpm


A.fib can be asymptomatic or present with:
💓Palpitations, chest discomfort/angina
🫁 SOB, exercise intolerance
😫Fatigue, weakness
🧠Pre-syncope
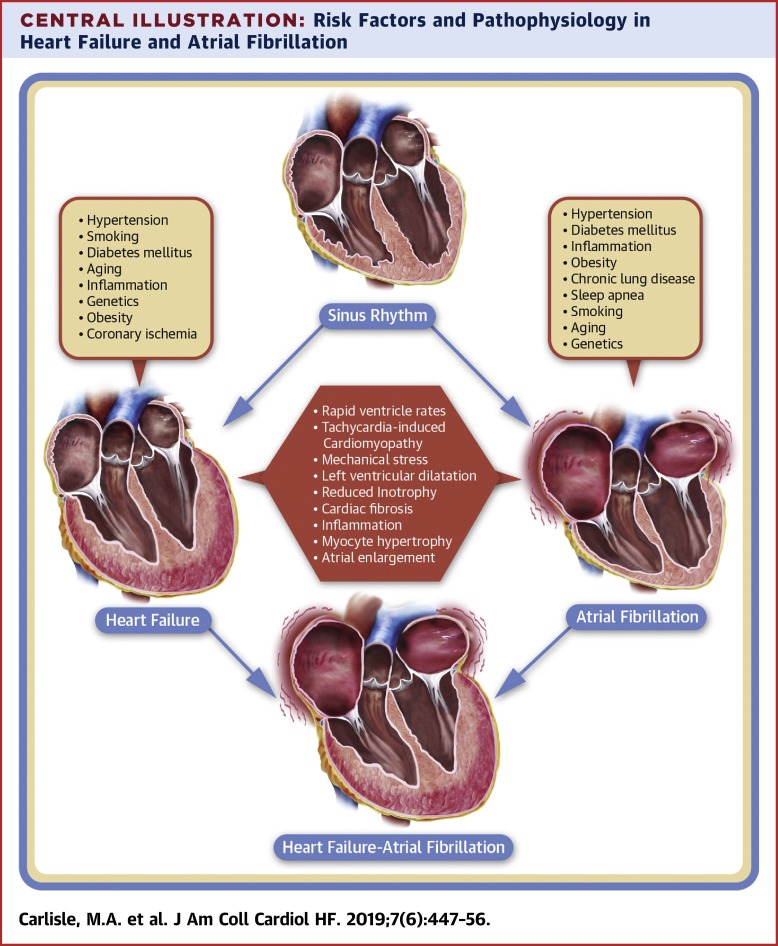
💔Heart failure (tachycardia mediated cardiomyopathy - dilated LV, reversible)
💓Palpitations, chest discomfort/angina
🫁 SOB, exercise intolerance
😫Fatigue, weakness
🧠Pre-syncope
💔Heart failure (tachycardia mediated cardiomyopathy - dilated LV, reversible)

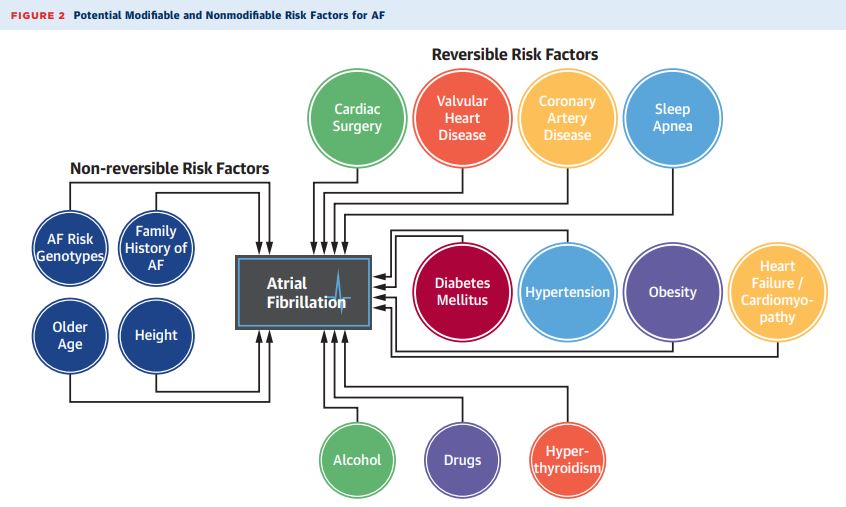
🏴Causes of A.fib?
☠️PIRATES☠️
P ulmonary 🫁: PE, COPD
I schemia (ACS), I diopathic, I atrogenic
R heumatic heart (valvular)
A nemia, A trial myxoma
T hyrotoxicosis 👔
E thanol 🍷, E levated BP
S epsis, S leep apnea 😴, S ick sinus
☠️PIRATES☠️
P ulmonary 🫁: PE, COPD
I schemia (ACS), I diopathic, I atrogenic
R heumatic heart (valvular)
A nemia, A trial myxoma
T hyrotoxicosis 👔
E thanol 🍷, E levated BP
S epsis, S leep apnea 😴, S ick sinus

Time for a quick quiz! 📝
Every patient with rapid A.fib needs an inpatient echocardiogram
Every patient with rapid A.fib needs an inpatient echocardiogram
FALSE!
🔥Indications for echo🔥:
🟣First episode of A.fib
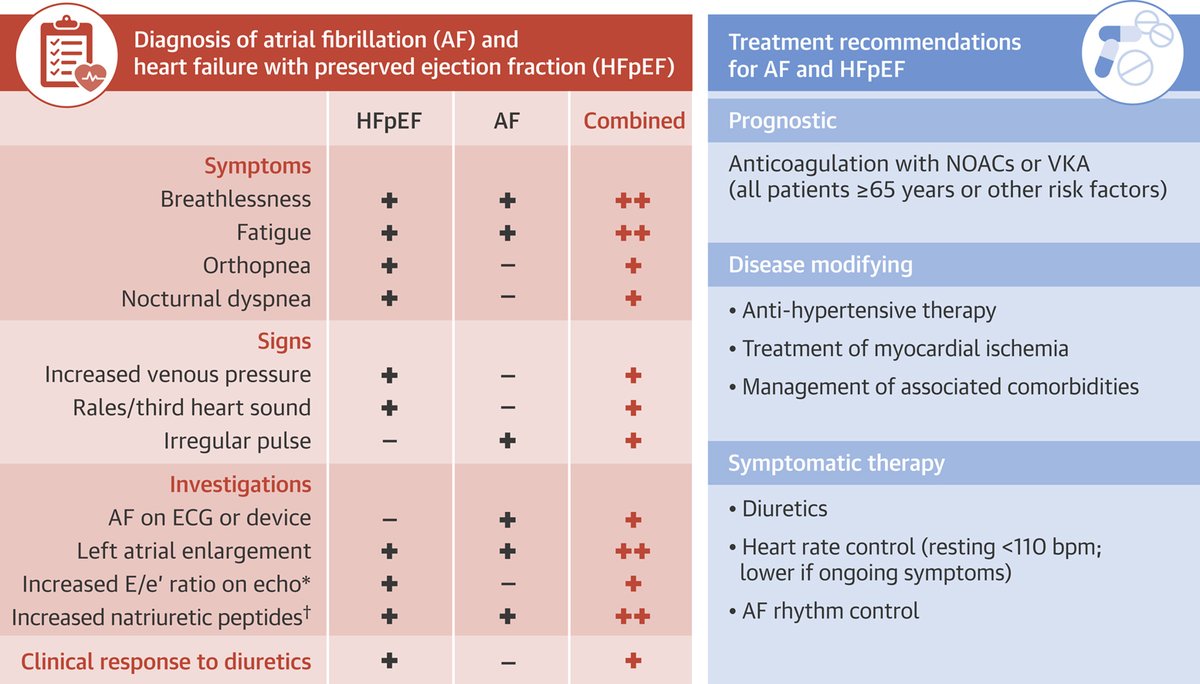
🟣New onset concurrent HF (HFpEF and A.fib can be vicious twins!)
🟣Suspected new onset ischemia
🟣TEE to rule out thrombus before cardioversion
Check out @medicine_strong video on acute A.fib: bit.ly/3iFpCAh
🔥Indications for echo🔥:
🟣First episode of A.fib
🟣New onset concurrent HF (HFpEF and A.fib can be vicious twins!)
🟣Suspected new onset ischemia
🟣TEE to rule out thrombus before cardioversion
Check out @medicine_strong video on acute A.fib: bit.ly/3iFpCAh
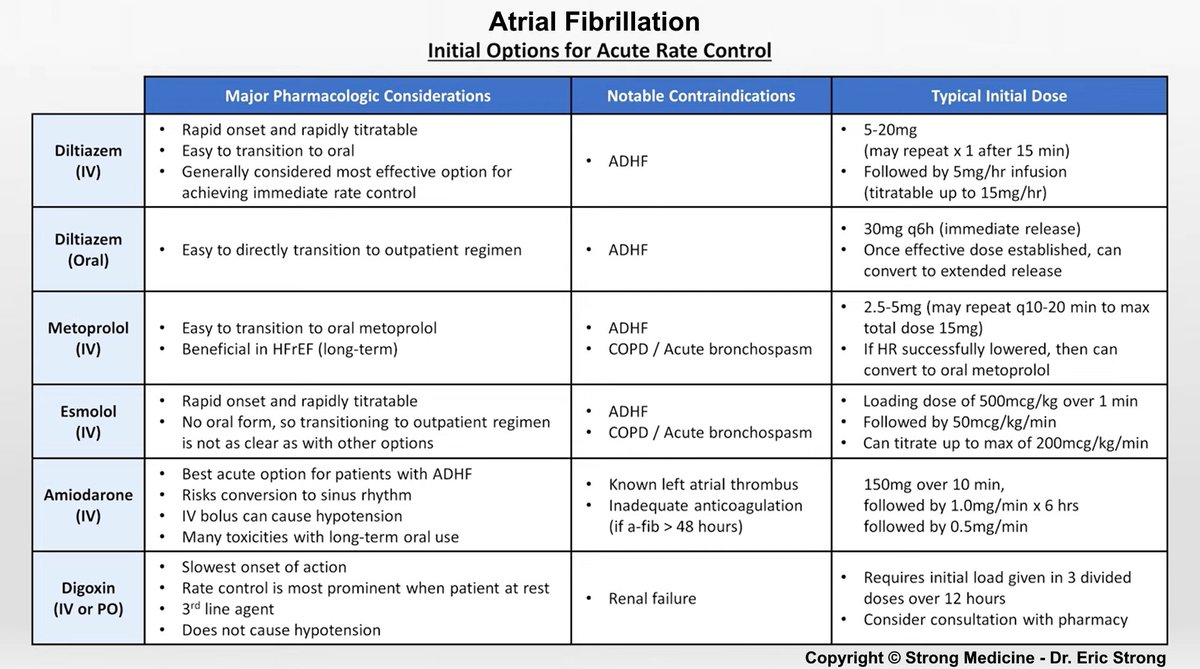
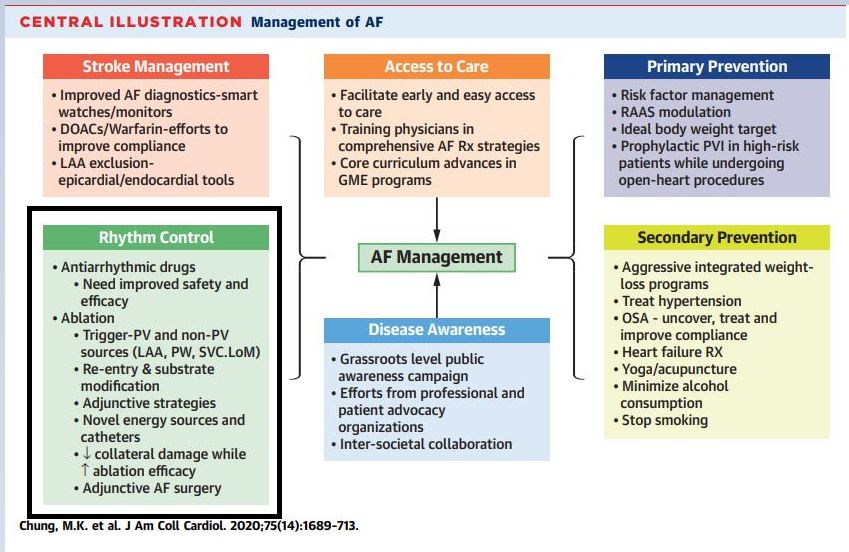
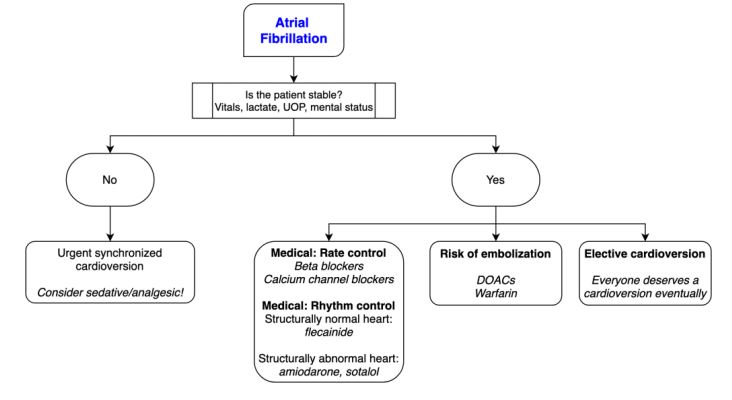
🏥A.fib Management🏥
Assess for instability: hypotension, lactate, AMS, decreased urine output
Unstable --> ⚡️Synchronized Cardioversion⚡️
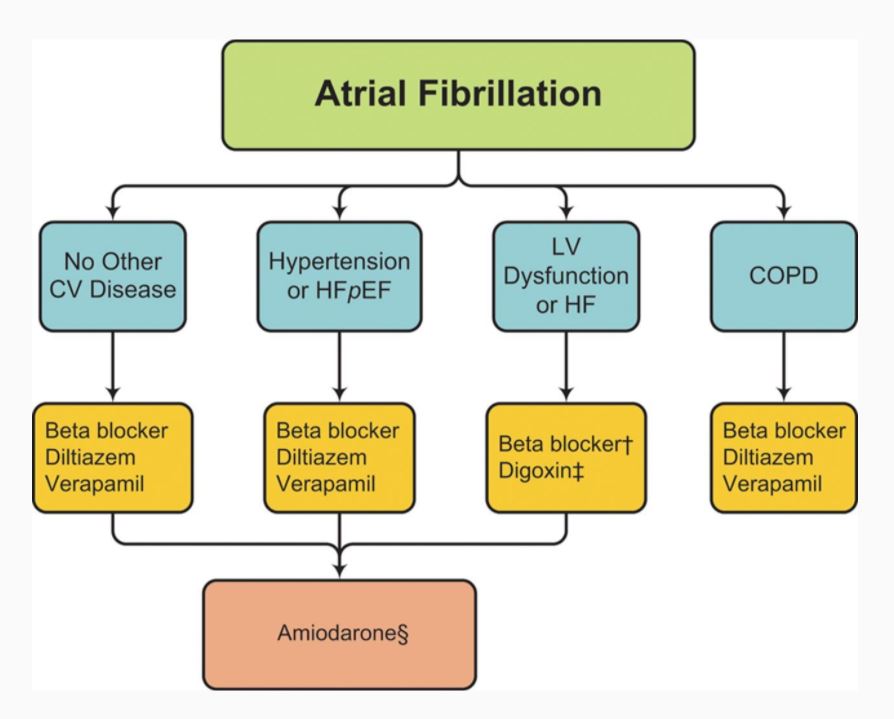
🏃Rate control🏃: beta-blocker, Ca channel blocker, amiodarone
🎯Goal: <80bpm if symptomatic/HF, <110bpm if normal LV and asymptomatic
Assess for instability: hypotension, lactate, AMS, decreased urine output
Unstable --> ⚡️Synchronized Cardioversion⚡️
🏃Rate control🏃: beta-blocker, Ca channel blocker, amiodarone
🎯Goal: <80bpm if symptomatic/HF, <110bpm if normal LV and asymptomatic
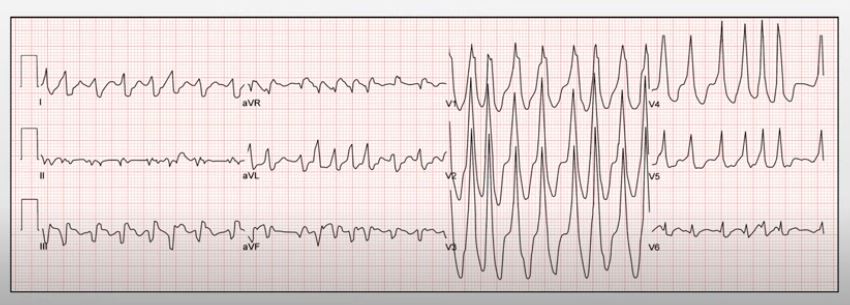
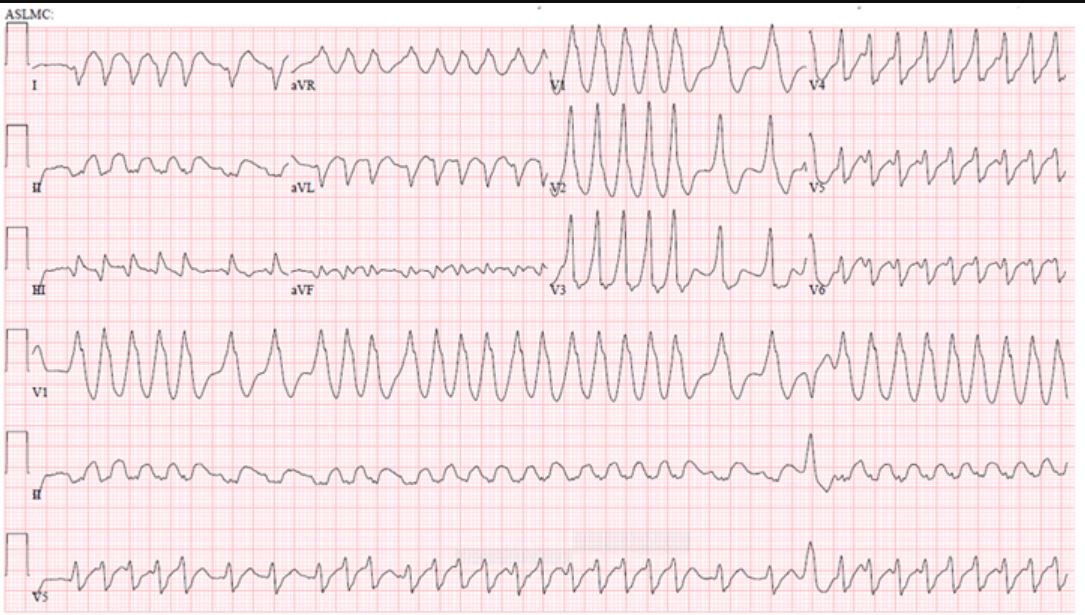
Now, let's consider you are seeing a patient with an irregularly irregular rhythm and an EKG as shown below 👇
(EKG from @medicine_strong)
(EKG from @medicine_strong)
Which agent would you chose for initial acute *rate* control?
🏃💊🏃
🏃💊🏃
Answer?
🔥Procainamide🔥
EKG shows:
🔸irregularly irregular rhythm
🔹wide QRS complex
🔸rapid rate ➡️ pre-excited A-fib (A-fib + WPW)
Accessory pathway that bypasses AV node
◽️can NOT use AV nodal blocking agents; may trigger V.fib!
◾️use Procainamide or Ibutilide instead
🔥Procainamide🔥
EKG shows:
🔸irregularly irregular rhythm
🔹wide QRS complex
🔸rapid rate ➡️ pre-excited A-fib (A-fib + WPW)
Accessory pathway that bypasses AV node
◽️can NOT use AV nodal blocking agents; may trigger V.fib!
◾️use Procainamide or Ibutilide instead
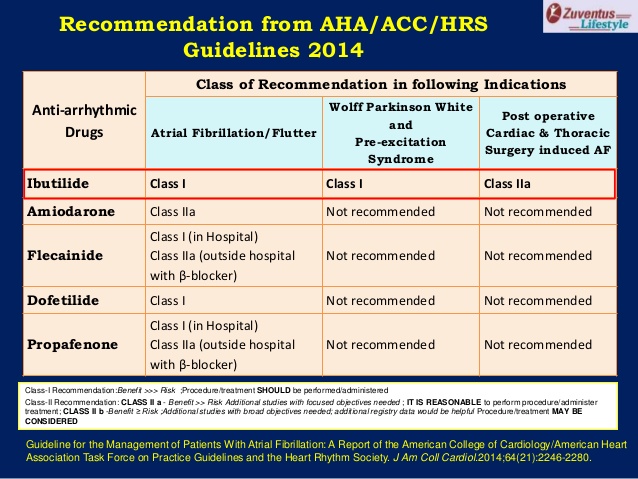
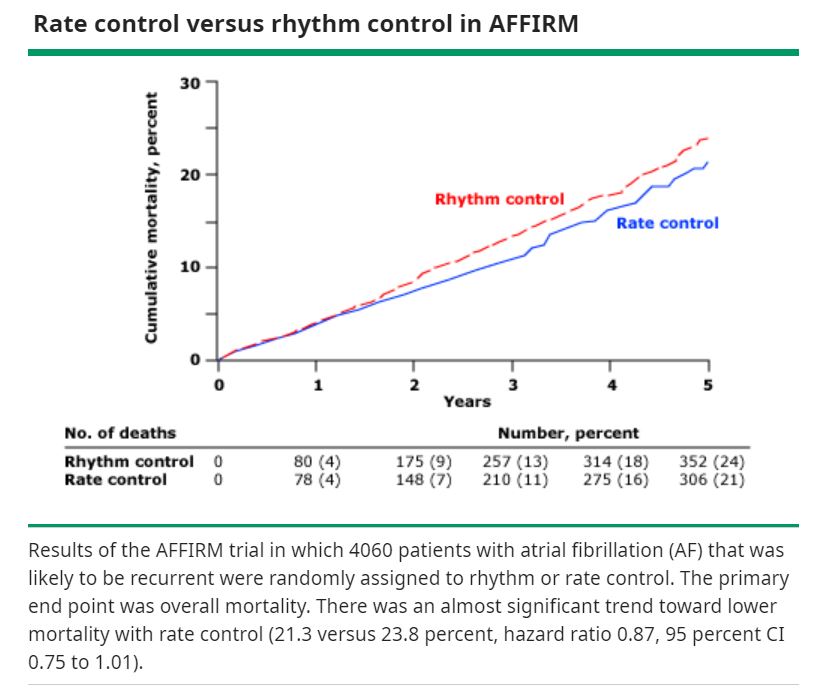
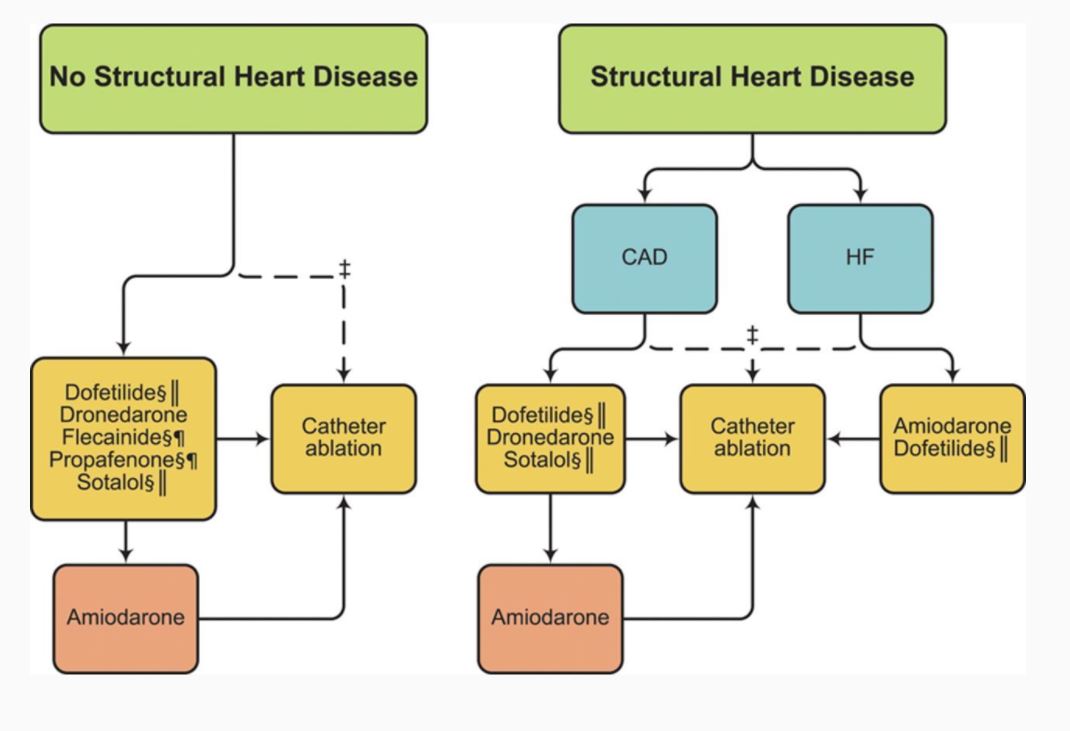
🥁What about Rhythm control?🥁
Use if:
🔹A.Fib is causing hemodynamic instability
🔸Symptoms despite adequate rate control, and/or
🔹Unable to tolerate rate-controlling agents
💊Flecainide, propafenone, sotalol, dronedarone, dofetilide, amiodarone💊
Use if:
🔹A.Fib is causing hemodynamic instability
🔸Symptoms despite adequate rate control, and/or
🔹Unable to tolerate rate-controlling agents
💊Flecainide, propafenone, sotalol, dronedarone, dofetilide, amiodarone💊
🌩️To Cardiovert or not to Cardiovert🌩️
That is the question 🧐
Cardiovert if:
📢Anticoagulation > 3 weeks
📢Less than 48 hours of A.fib
📢TEE does *not* show clot
💊Continue anticoagulation (see below) for 4 weeks after cardioversion
That is the question 🧐
Cardiovert if:
📢Anticoagulation > 3 weeks
📢Less than 48 hours of A.fib
📢TEE does *not* show clot
💊Continue anticoagulation (see below) for 4 weeks after cardioversion

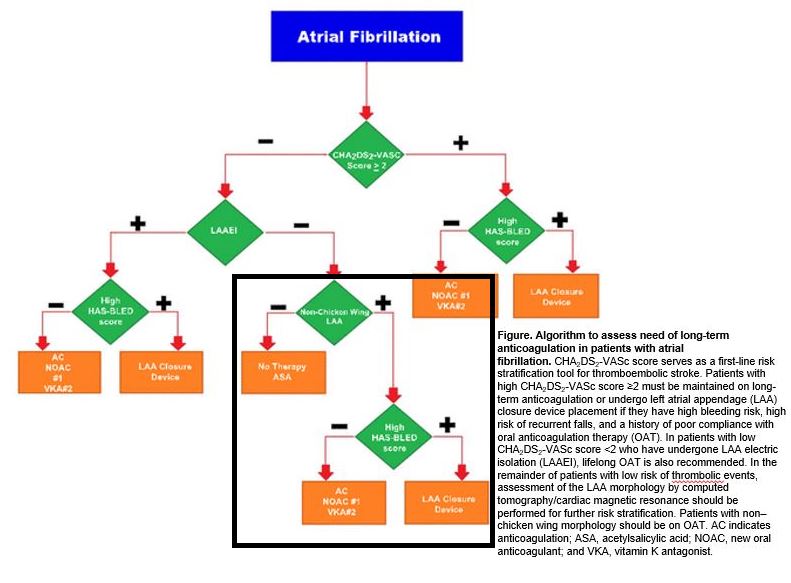
🩸To anticoagulate or not🩸
CHA₂DS₂-VASc score🆚HAS-BLED score
if CHA₂DS₂-VASc >2 men, >3 women ➡️ anticoagulate💊
Non-valvular A.fib:
-DOAC (apixaban, rivaroxaban)
Valvular A.fib:
-Warfarin
To prevent bleeding, no antiplatelets
If on antiplatelets, use PPI to⬇GI bleed
CHA₂DS₂-VASc score🆚HAS-BLED score
if CHA₂DS₂-VASc >2 men, >3 women ➡️ anticoagulate💊
Non-valvular A.fib:
-DOAC (apixaban, rivaroxaban)
Valvular A.fib:
-Warfarin
To prevent bleeding, no antiplatelets
If on antiplatelets, use PPI to⬇GI bleed


Don't forget rheumatic or acquired mitral stenosis when thinking of "valvular" A.fib!
Check out this awesome case and explanation by @jelevenson 👇
Check out this awesome case and explanation by @jelevenson 👇
https://twitter.com/jelevenson/status/1350865284446490626
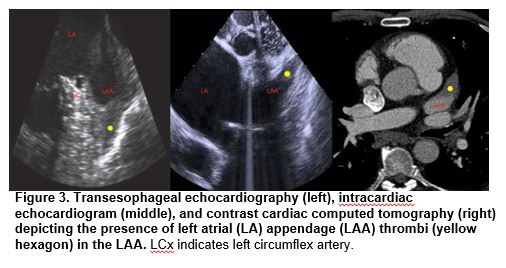
Left atrial appendage (LAA) = embryonic LA remnant
🔹typically has biphasic emptying⌚️
With A.fib ➡️Virchow's triad:
📐endocardial dysfunction
📐abnormal blood stasis
📐altered hemostasis
+
📉Reduced LAA peak flow velocity ➡️ thrombus
Thrombus in LAA leads to stroke risk! 🧠
🔹typically has biphasic emptying⌚️
With A.fib ➡️Virchow's triad:
📐endocardial dysfunction
📐abnormal blood stasis
📐altered hemostasis
+
📉Reduced LAA peak flow velocity ➡️ thrombus
Thrombus in LAA leads to stroke risk! 🧠

Interestingly, some studies show that LAA morphology can be associated with stroke risk
LAA morphologies?
4 most common:
🍗chicken wing
🌵cactus
🌪️windsock
🥦cauliflower
Non-chicken wing morphology may increase risk of thrombus & require oral anticoagulation
LAA morphologies?
4 most common:
🍗chicken wing
🌵cactus
🌪️windsock
🥦cauliflower
Non-chicken wing morphology may increase risk of thrombus & require oral anticoagulation
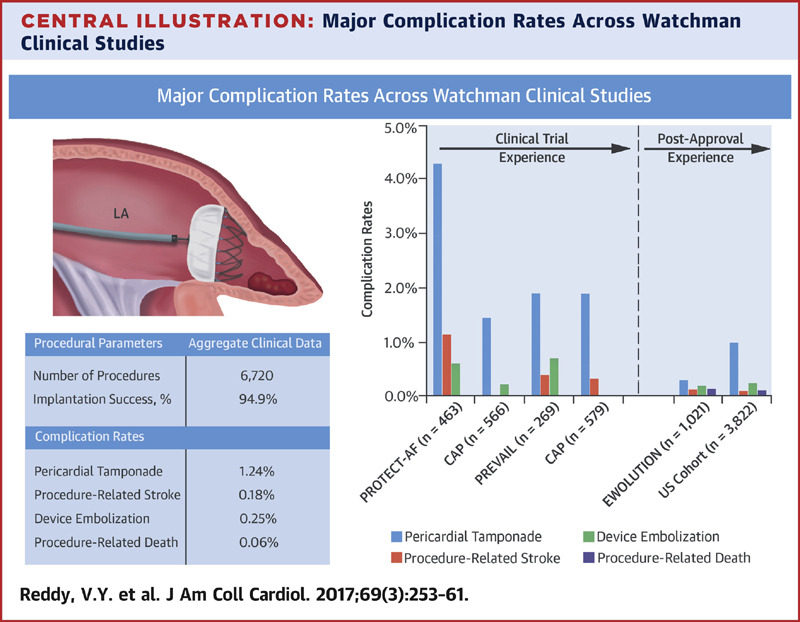
🔪Can perform percutaneous catheter-based endocardial and epicardial LAA closure🔪
Devices such as⌚️WATCHMAN⌚️
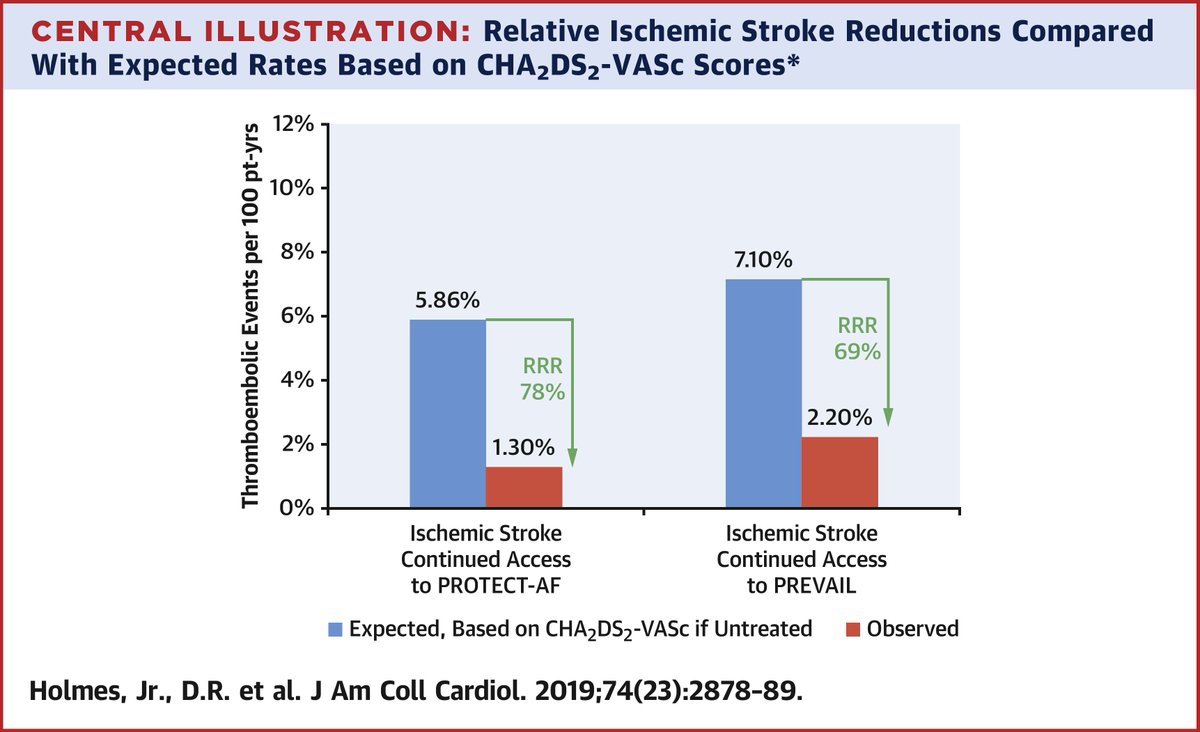
▪️PROTECT-AF trial showed non-inferiority to warfarin
Devices such as⌚️WATCHMAN⌚️
▪️PROTECT-AF trial showed non-inferiority to warfarin

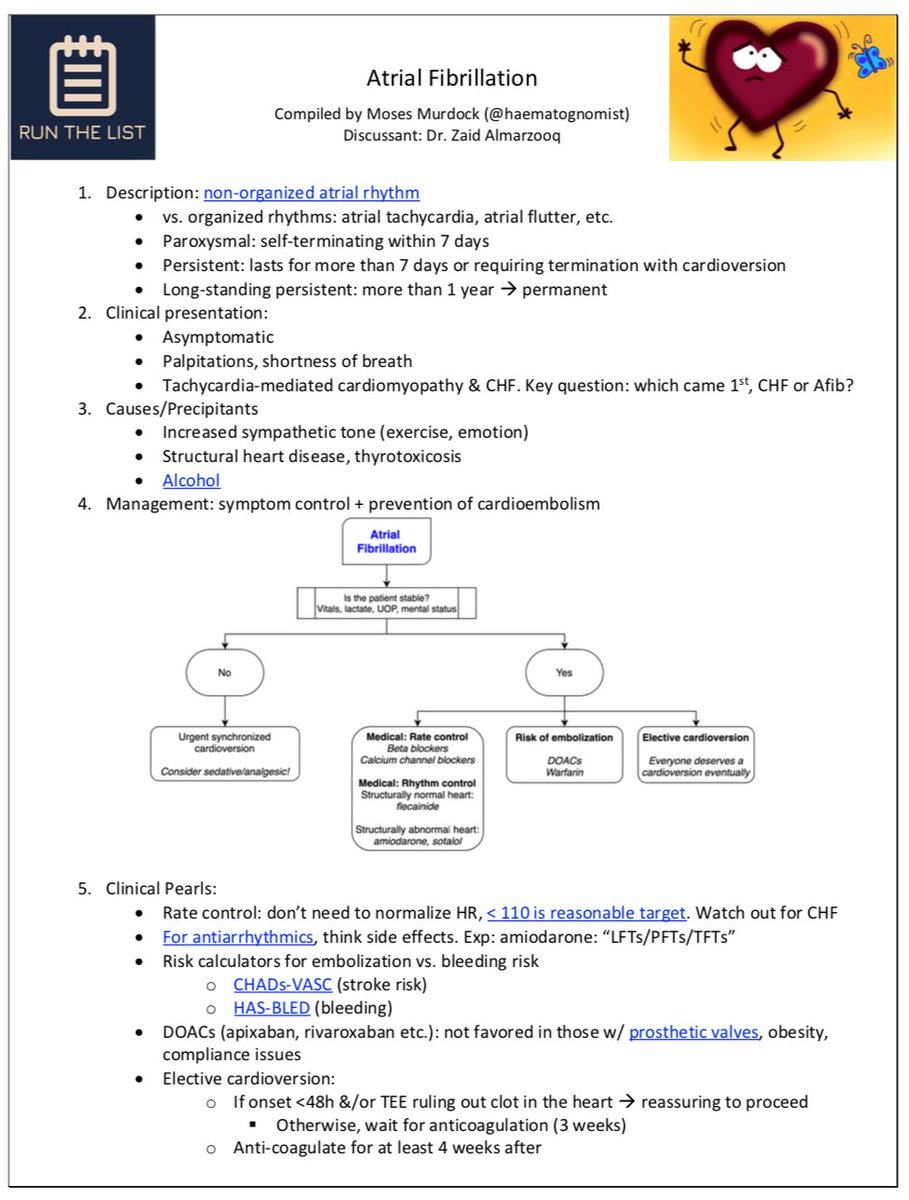
✨Summary for A.fib✨
1. Workup:
-reversible causes (anemia, thyroid, sleep apnea, alcohol, BP, decomp HF)
-💘cardiac causes (LV function, valvular disease, etc)
2. Goals:
-symptom control vs. prevention
3. Think🤔:
-Rate vs Rhythm control and anticoagulation
RTL handout ⤵️
1. Workup:
-reversible causes (anemia, thyroid, sleep apnea, alcohol, BP, decomp HF)
-💘cardiac causes (LV function, valvular disease, etc)
2. Goals:
-symptom control vs. prevention
3. Think🤔:
-Rate vs Rhythm control and anticoagulation
RTL handout ⤵️
Download the one-page A Fib RTL handout (free!) here:
runthelistpodcast.com/s/RTL_Afib_Han…
Listen to Episode 23: Atrial Fibrillation 👇
🍎podcasts: apple.co/2XhpRIU
🎶Spotify: spoti.fi/3caXvV3
RTL🕸️: bit.ly/3b6svs0
#FOAMed #MedEd
runthelistpodcast.com/s/RTL_Afib_Han…
Listen to Episode 23: Atrial Fibrillation 👇
🍎podcasts: apple.co/2XhpRIU
🎶Spotify: spoti.fi/3caXvV3
RTL🕸️: bit.ly/3b6svs0
#FOAMed #MedEd
REFs (1/3)
[2]osmosis.org/learn/Atrial_f…
[2] ] Mikhail Torosoff & Steven A. Fein. "I Read ECGs An interactive practical guide to the electrocardiogram interpretation"
[3,5,12,14,16,18]pubmed.ncbi.nlm.nih.gov/32273035/
[3]litfl.com/atrial-fibrill…
[4]aafp.org/afp/2011/0101/…
[2]osmosis.org/learn/Atrial_f…
[2] ] Mikhail Torosoff & Steven A. Fein. "I Read ECGs An interactive practical guide to the electrocardiogram interpretation"
[3,5,12,14,16,18]pubmed.ncbi.nlm.nih.gov/32273035/
[3]litfl.com/atrial-fibrill…
[4]aafp.org/afp/2011/0101/…
REFs (2/3)
[4]pubmed.ncbi.nlm.nih.gov/31146871/
[5]ahajournals.org/doi/10.1161/ci…
[7,8-11]
[5] jacc.org/doi/full/10.10…
[8,12]ahajournals.org/doi/10.1161/ci…
[11] acc.org/education-and-…
[11]slideshare.net/ramachandrabar…
[12]uptodate.com/contents/rhyth…
[13]aafp.org/afp/2016/0915/…
[4]pubmed.ncbi.nlm.nih.gov/31146871/
[5]ahajournals.org/doi/10.1161/ci…
[7,8-11]
[5] jacc.org/doi/full/10.10…
[8,12]ahajournals.org/doi/10.1161/ci…
[11] acc.org/education-and-…
[11]slideshare.net/ramachandrabar…
[12]uptodate.com/contents/rhyth…
[13]aafp.org/afp/2016/0915/…
REFs (3/3)
[16,17]ahajournals.org/doi/full/10.11…
[18]jacc.org/doi/full/10.10…
[18]pubmed.ncbi.nlm.nih.gov/27816552/
[16,17]ahajournals.org/doi/full/10.11…
[18]jacc.org/doi/full/10.10…
[18]pubmed.ncbi.nlm.nih.gov/27816552/
@MedTweetorials @cardionerds @medicine_strong @CPSolvers @COREIMpodcast @CuriousClinPod @DxRxEdu @rabihmgeha @tony_breu @AvrahamCooperMD @medrants @AmitGoyalMD @Dr_DanMD
• • •
Missing some Tweet in this thread? You can try to
force a refresh