Today, the headlines enjoyed the @CommonsPAC report on COVID19: Test, Track and Trace (part 1).
Some reflections that don't focus on the ££ detail. 🧵1/11
committees.parliament.uk/publications/4…
Some reflections that don't focus on the ££ detail. 🧵1/11
committees.parliament.uk/publications/4…
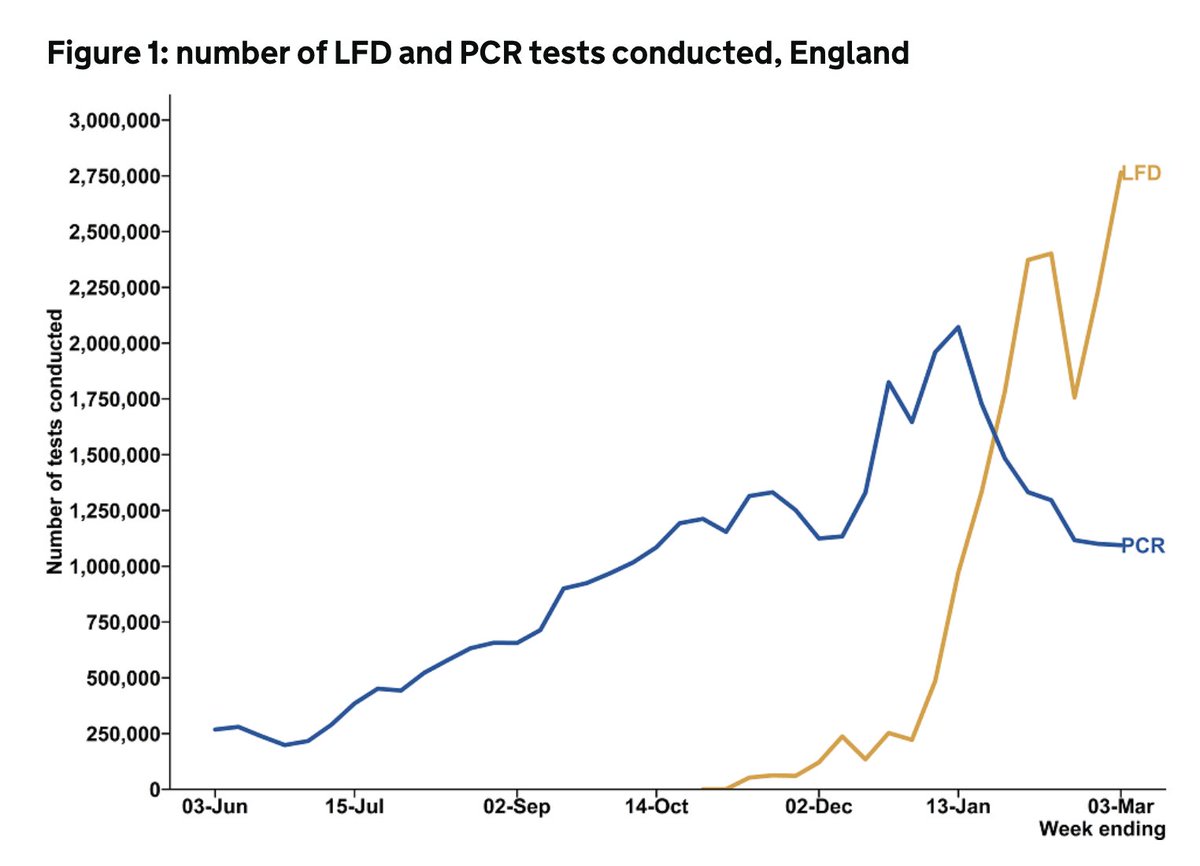
The T&T budget is massive, and it's right that it has scrutiny. The vast majority (perhaps around 80%) has gone on testing and the achievements here are pretty significant.
Regularly >5% of population are tested for a disease that we didn't know existed around a yr ago. 2/
Regularly >5% of population are tested for a disease that we didn't know existed around a yr ago. 2/
But by the same token relatively little has been spend on the contact tracing and isolation support.
We can't test our way out of the pandemic - it has to go hand in hand with tracing contacts and ensuring people have the support they need to isolate. 3/
We can't test our way out of the pandemic - it has to go hand in hand with tracing contacts and ensuring people have the support they need to isolate. 3/
The weekly T&T data don't tell us who doesn't get tested despite having symptoms (COVID Social Study suggests that only around 1/3 regular test if symptomatic)
and who struggles to adhere to isolation guidance (CORSAIR study suggests perhaps as little as 1 in 5 fully adhere). 4/
and who struggles to adhere to isolation guidance (CORSAIR study suggests perhaps as little as 1 in 5 fully adhere). 4/
We address these specific points around testing, contact tracing, isolation, and inequalities in our original @HealthFdn submission to the @CommonsPAC.
Can read more here:
health.org.uk/news-and-comme… 5/
Can read more here:
health.org.uk/news-and-comme… 5/
The PAC report usefully highlights that local gov should have been more directly involved early on & recommends more engagement with public health and local stakeholders.
And whilst a lot has changed since T&T launched, local gov and community engagement will remain critical 6/
And whilst a lot has changed since T&T launched, local gov and community engagement will remain critical 6/
COVID's exposed and exacerbated inequalities across society.
Moving forward, test/trace/isolation policies need to be co-designed with the local authorities and communities that have been most impacted by COVID, and who have the most to gain from the reopening of society. 7/
Moving forward, test/trace/isolation policies need to be co-designed with the local authorities and communities that have been most impacted by COVID, and who have the most to gain from the reopening of society. 7/
This needs to happen alongside a coordinated cross gov approach to the deep structural drivers of inequalities & enduring transmission across more deprived parts of the country.
With local gov/regional flexibility & resource to address their ongoing local challenges. 8/
With local gov/regional flexibility & resource to address their ongoing local challenges. 8/
Without this, the parts of the country that are least able to cope will have ongoing transmission, more lockdowns, more economic and social isolation, more direct and indirect harm, more variants, and more inequalities.
As a society, this shouldn't in any way be tolerable. 9/
As a society, this shouldn't in any way be tolerable. 9/
So while the report makes some very helpful T&T-specific recommendations, the success of NHS T&T and the broader COVID response also depends on the gov meaningfully engaging in the wider structural drivers of inequalities in England 10/ 

And many of the necessary policy actions and investments required are dealt with here:
health.org.uk/publications/b… 11/11
health.org.uk/publications/b… 11/11
• • •
Missing some Tweet in this thread? You can try to
force a refresh