Excited to share our recently published point-counterpoint paper on halting implantation of the @bostonsci subcutaneous-ICD
The paper is now open access.
A brief thread
The paper is now open access.
A brief thread
https://twitter.com/JACCJournals/status/1370457134194917381
Background:
I have used the S-ICD. It has *potential* advantages over the traditional trans-venous ICD system
But it is the newcomer. A #MedicalConservative believes proponents of new stuff must show more than *potential* benefits over the tried and true.
I have used the S-ICD. It has *potential* advantages over the traditional trans-venous ICD system
But it is the newcomer. A #MedicalConservative believes proponents of new stuff must show more than *potential* benefits over the tried and true.
Recent Issues w the S-ICD:
In the first part of the commentary @bogdienache and I focus our argument around:
-Two Class 1 FDA recalls of the S-ICD
-Serious concerns over the PRAETORIAN trial-- the only trial RCT comparing transvenous ICD (standard) to S-ICD
In the first part of the commentary @bogdienache and I focus our argument around:
-Two Class 1 FDA recalls of the S-ICD
-Serious concerns over the PRAETORIAN trial-- the only trial RCT comparing transvenous ICD (standard) to S-ICD
The most concerning of the FDA recalls involves a lead fracture that could lead to either inappropriate shocks or ineffective shocks in the event of death.
Both are bad outcomes. You say: just use a different lead.
Problem: there isn't a different lead.
Both are bad outcomes. You say: just use a different lead.
Problem: there isn't a different lead.
As for the PRAETORIAN critical appraisal, we focus on three issues
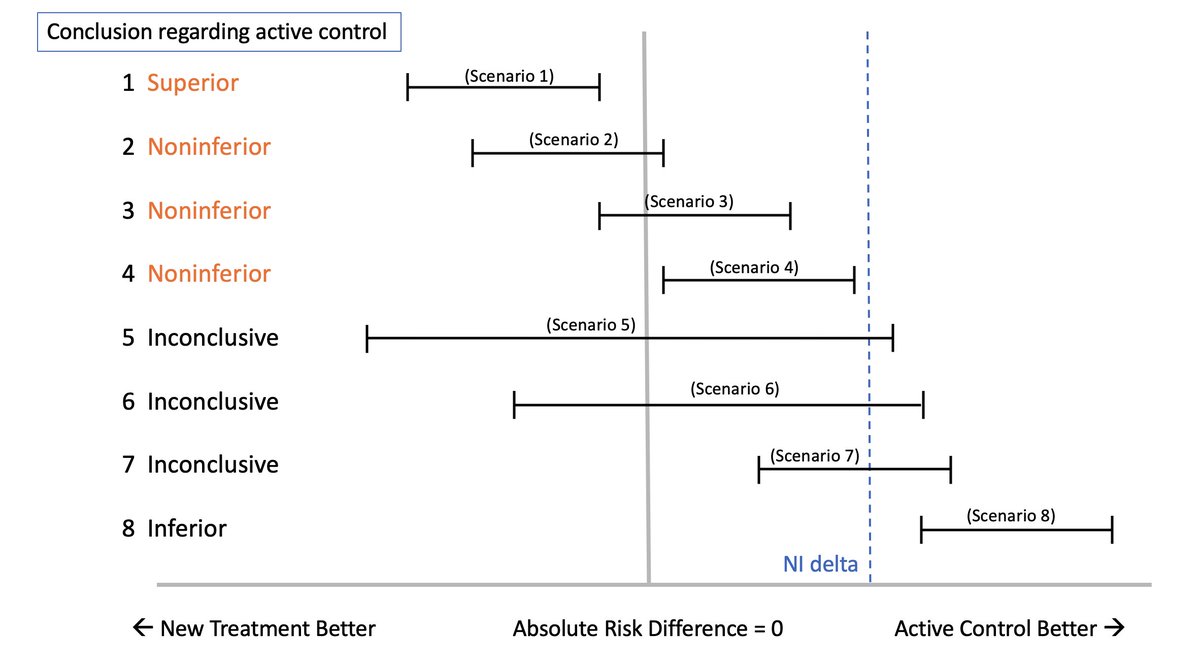
--First was brought out by @WFMMD et al in a NEJM letter to the editor. Basically, you bias a non-inferiority trial if you include endpoints that go in opposite directions.
PRAETORIAN did this. See below>
--First was brought out by @WFMMD et al in a NEJM letter to the editor. Basically, you bias a non-inferiority trial if you include endpoints that go in opposite directions.
PRAETORIAN did this. See below>

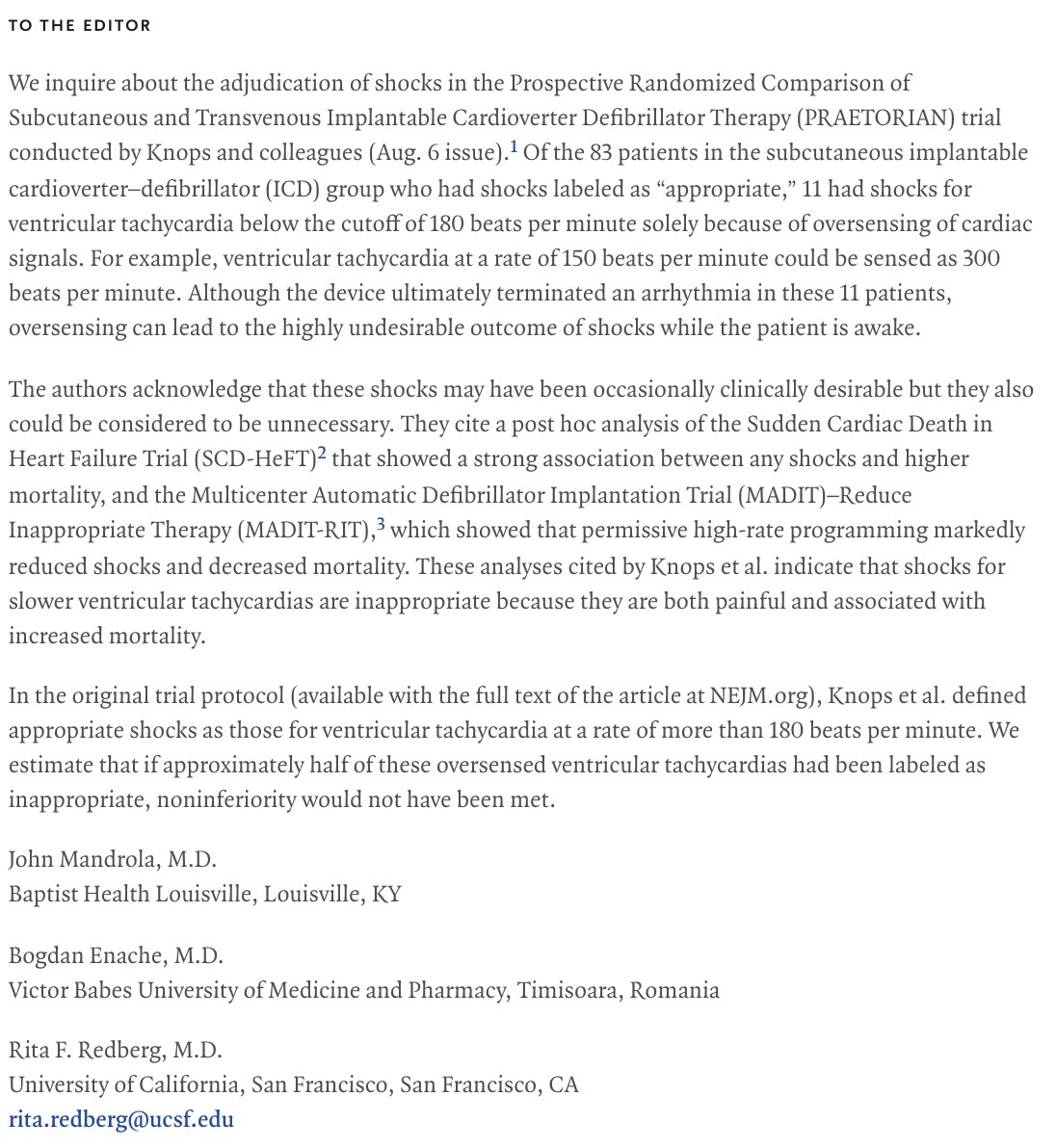
Second issue w PRAETORIAN was adjudication of shocks. 11 of 83 "appropriate" shocks in the S-ICD arm were for slower VTs < 180 bpm.
You are curious why a VT under 180bpm was sensed as appropriate and shocked by SICD
A: the S-ICD oversensed or double-counted all 11.
Cont/
You are curious why a VT under 180bpm was sensed as appropriate and shocked by SICD
A: the S-ICD oversensed or double-counted all 11.
Cont/
@RFRedberg and @bogdienache and I published this concern as a LTE in NEJM.
See image -
Problem w calling shocks as over-sensed VT is that strong data suggests permissive programming to REDUCE shocks improves mortality (MADIT-RIT trial)
See image -
Problem w calling shocks as over-sensed VT is that strong data suggests permissive programming to REDUCE shocks improves mortality (MADIT-RIT trial)
Thus, based on the FDA recalls and a trial that would have not have met non-inferiority without biased endpoints and biased endpoint adjudication, we strongly favor a pause in SICD implants.
Larger lesson: perhaps docs and FDA need more caution in acceptance of new tech
Larger lesson: perhaps docs and FDA need more caution in acceptance of new tech
Finally,
#JACCEP and @JACCJournals rightly published this as a point-counterpoint article.
I say rightly b/c interpretation of science is a human endeavor and other smart people can see things differently.
Drs. Raul Weiss and Emile Daoud wrote the rebuttal. Take a look.
#JACCEP and @JACCJournals rightly published this as a point-counterpoint article.
I say rightly b/c interpretation of science is a human endeavor and other smart people can see things differently.
Drs. Raul Weiss and Emile Daoud wrote the rebuttal. Take a look.
Thanks to @shivkumarmd
Interested in thoughts from #EPeeps #cardiotwitter
And other trial and regulatory luminaries -- @califf001 @ScottGottliebMD @hmkyale @kaulcsmc @rwyeh
Please read the arguments--this is only a cursory summary.
Interested in thoughts from #EPeeps #cardiotwitter
And other trial and regulatory luminaries -- @califf001 @ScottGottliebMD @hmkyale @kaulcsmc @rwyeh
Please read the arguments--this is only a cursory summary.
correction ..in the event of *sudden cardiac* death
• • •
Missing some Tweet in this thread? You can try to
force a refresh