1/
HOW long do you live with #cirrhosis?
WHERE did MELD Score come from?
WHAT is a "TIPS"?
ARE you ready for re-#tweetorial
#livertwitter #medtwitter #meded
HOW long do you live with #cirrhosis?
WHERE did MELD Score come from?
WHAT is a "TIPS"?
ARE you ready for re-#tweetorial
#livertwitter #medtwitter #meded

2/
Imagine you are a patient with variceal bleed in 1940
🚫EGDs
🚫Banding
🚫hope
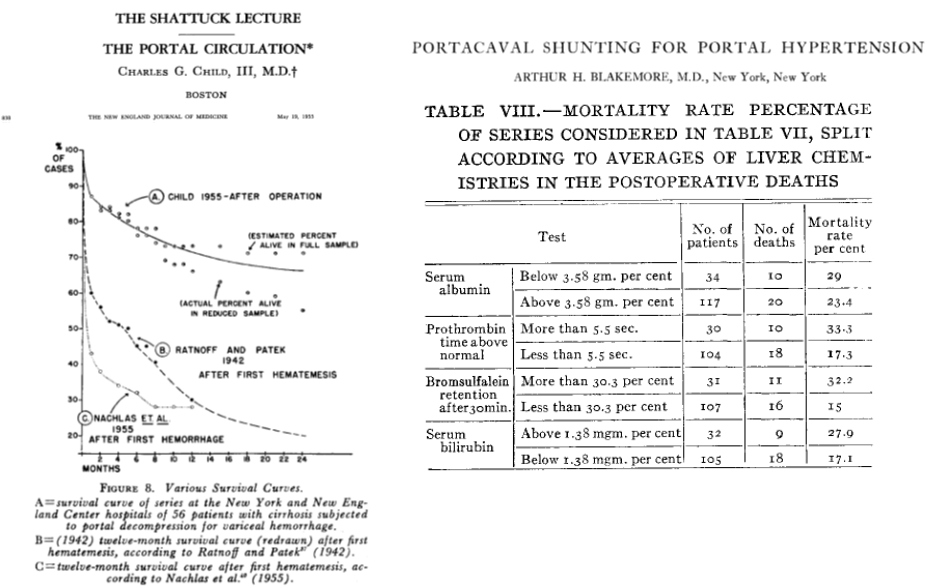
Then came portosystemic shunt surgery. A treatment!
The catch?
Lots of people still died after surgery
Imagine you are a patient with variceal bleed in 1940
🚫EGDs
🚫Banding
🚫hope
Then came portosystemic shunt surgery. A treatment!
The catch?
Lots of people still died after surgery



3/
What do we want to know so we can select the patients who will benefit from shunt surgery?
Options
🤔Liver function?
🤔Do they look & feel well?
🎉Why not both!?
Wantz & Payne developed an A-B-C score using
1⃣Albumin
2⃣Bili
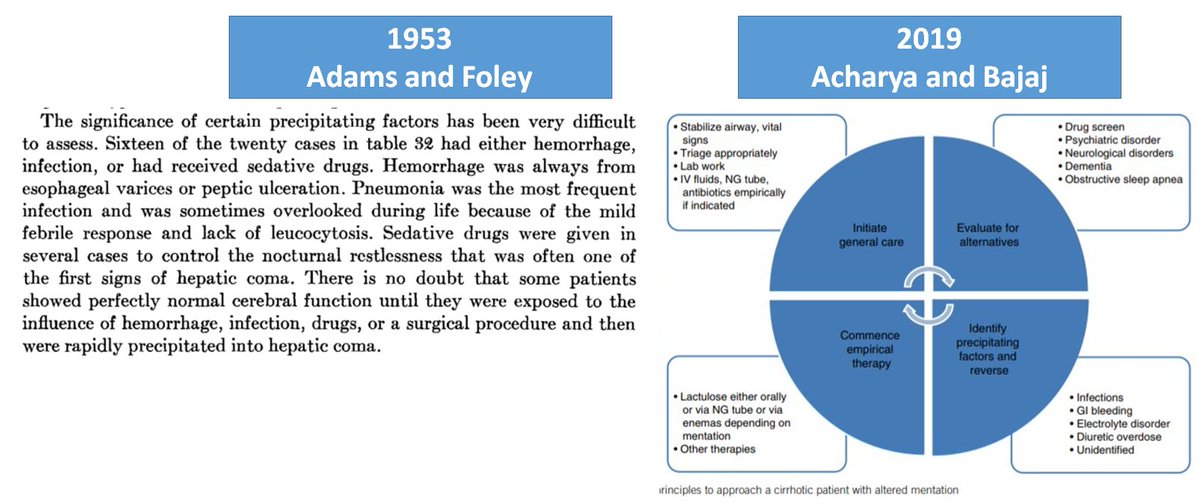
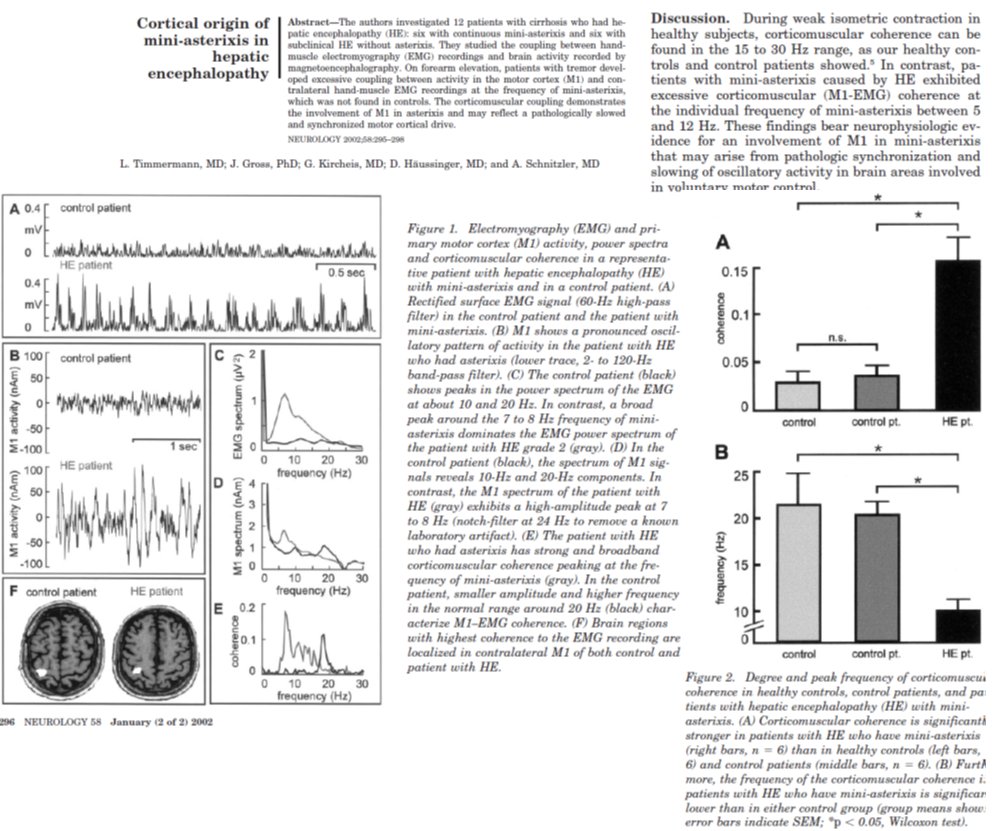
3⃣Encephalopathy
4⃣Ascites
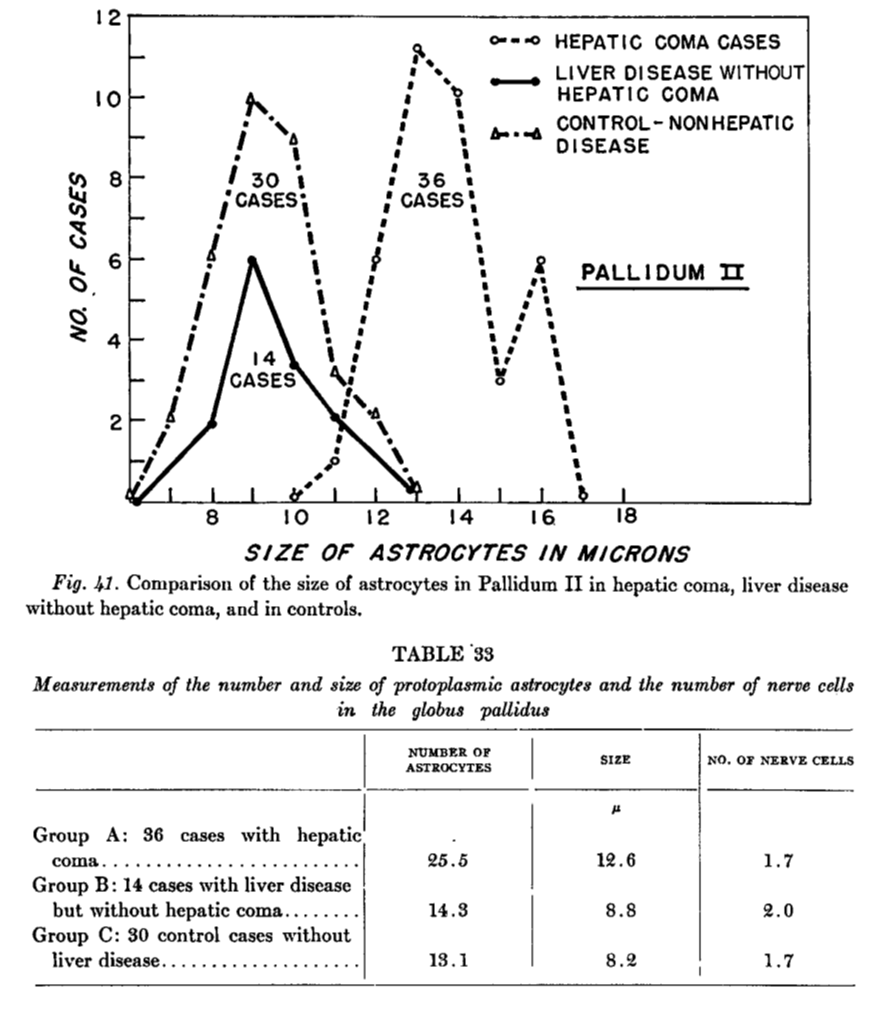
5⃣Muscle wasting
What do we want to know so we can select the patients who will benefit from shunt surgery?
Options
🤔Liver function?
🤔Do they look & feel well?
🎉Why not both!?
Wantz & Payne developed an A-B-C score using
1⃣Albumin
2⃣Bili
3⃣Encephalopathy
4⃣Ascites
5⃣Muscle wasting


4/
Kinda sounds a lot like the Child-Turcotte score, right?
Yep
Same outcomes too
So...why is it "Child" but not "Payne Class"?
I do not know
But I want you to meet Dr. Mary Ann Payne, someone whom I learned more about thanks to @docberza
Kinda sounds a lot like the Child-Turcotte score, right?
Yep
Same outcomes too
So...why is it "Child" but not "Payne Class"?
I do not know
But I want you to meet Dr. Mary Ann Payne, someone whom I learned more about thanks to @docberza
https://twitter.com/docberza/status/1291231379909496832?s=20


5/
There were 2 problems with Payne/Child Class:
1⃣Any 1 bad feature = Class C
2⃣Muscle wasting / Nutritional status was subjective
Enter Pugh
⭐️PT/INR in - nutrition out
⭐️Classes now based on 15pt scale
🎆Bam: Liverworld changed forever
There were 2 problems with Payne/Child Class:
1⃣Any 1 bad feature = Class C
2⃣Muscle wasting / Nutritional status was subjective
Enter Pugh
⭐️PT/INR in - nutrition out
⭐️Classes now based on 15pt scale
🎆Bam: Liverworld changed forever

6/
Deeper problems with Payne/Child/Pugh Class
1⃣Still has subjective parts (HE, Ascites)
2⃣Cannot provide probability of mortality over a specific timeframe
Something was about to happen that would force us to improve our prognostic skills
That thing?
TIPS
Deeper problems with Payne/Child/Pugh Class
1⃣Still has subjective parts (HE, Ascites)
2⃣Cannot provide probability of mortality over a specific timeframe
Something was about to happen that would force us to improve our prognostic skills
That thing?
TIPS
7/
TIPS (Tranjugular intrahepatic portosystemic shunt):
a brief history
😢Shunt surgery = super morbid
🤔1969: Maybe a transjugular teflon shunt?
🤔1982: Maybe just balloon dilated tract?
😢Both shunts shut down
😀How about this fancy balloon-expanded stent?
Game on
TIPS (Tranjugular intrahepatic portosystemic shunt):
a brief history
😢Shunt surgery = super morbid
🤔1969: Maybe a transjugular teflon shunt?
🤔1982: Maybe just balloon dilated tract?
😢Both shunts shut down
😀How about this fancy balloon-expanded stent?
Game on




8/
TIPS was a game changer
There was just one problem.
Lots of people were dying after TIPS
We needed a better way to select patients again!
TIPS was a game changer
There was just one problem.
Lots of people were dying after TIPS
We needed a better way to select patients again!


9/
Enter MELD
The Mayo score for 'Endstage' Liver Disease:
1⃣A nomogram that avoids math (bring your ruler though)
2⃣Predicted mortality in ALL-COMERS w/Child B-C
3⃣Was the first score to go online for all to use
Enter MELD
The Mayo score for 'Endstage' Liver Disease:
1⃣A nomogram that avoids math (bring your ruler though)
2⃣Predicted mortality in ALL-COMERS w/Child B-C
3⃣Was the first score to go online for all to use


10/
Right place, right time
Just as MELD came on the scene, the Government demanded a new, objective way to allocate organs on the waitlist
In 2002, MELD got a job promotion
For more on MELD in transplant, check out @aly_kaplanMD's liverfellow.org/post/meld-scor…
Right place, right time
Just as MELD came on the scene, the Government demanded a new, objective way to allocate organs on the waitlist
In 2002, MELD got a job promotion
For more on MELD in transplant, check out @aly_kaplanMD's liverfellow.org/post/meld-scor…

11/
MELD is awesome but can still be improved
1⃣Hyponatremia =
⬆️mortality
⬆️risk of hepatorenal syndrome
So how about MELD-Na?!
2⃣Creatinine-based scores low-ball risk for🙋♀️
How about the MELD-GRAIL-Na which uses GFR instead?
MELD is awesome but can still be improved
1⃣Hyponatremia =
⬆️mortality
⬆️risk of hepatorenal syndrome
So how about MELD-Na?!
2⃣Creatinine-based scores low-ball risk for🙋♀️
How about the MELD-GRAIL-Na which uses GFR instead?


12/
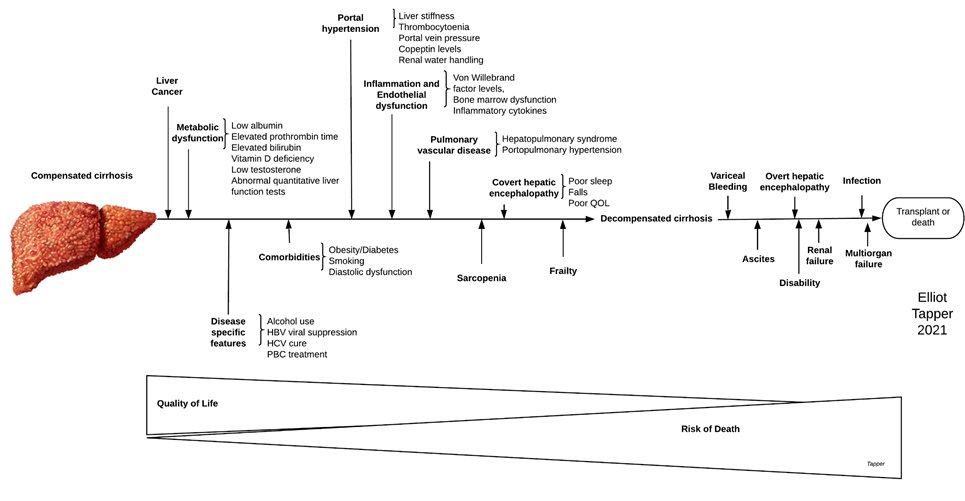
As awesome as MELD becomes, it's still unhelpful for the majority of patients with #cirrhosis who are compensated
This is a 🔥 area, summarized below
Some🔑tools
1⃣Portal pressure, liver stiffness (Fibroscan)
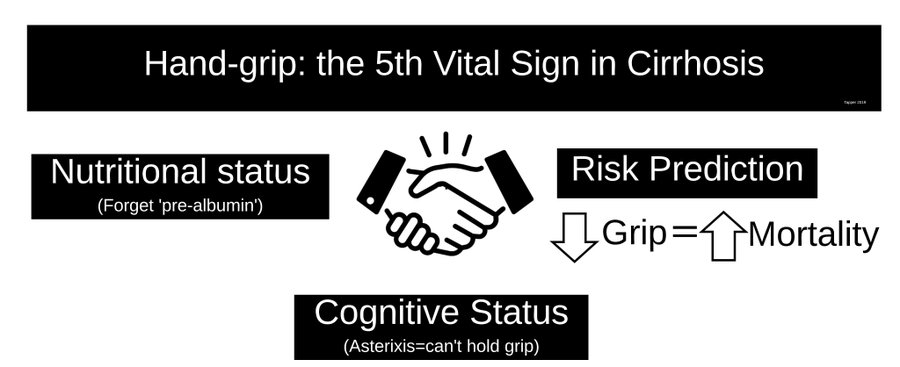
2⃣Payne's original: sarcopenia, frailty!
3⃣🧠function, PROs
As awesome as MELD becomes, it's still unhelpful for the majority of patients with #cirrhosis who are compensated
This is a 🔥 area, summarized below
Some🔑tools
1⃣Portal pressure, liver stiffness (Fibroscan)
2⃣Payne's original: sarcopenia, frailty!
3⃣🧠function, PROs

15/
Summary
1⃣Surgery & TIPS for variceal bleeding led to discovery of prognostic tools for #cirrhosis, like Child (or Payne) class and MELD
2⃣The 1st tool included an eye-ball test for muscle wasting
3⃣MELD improves with better estimates of kidney risk
Summary
1⃣Surgery & TIPS for variceal bleeding led to discovery of prognostic tools for #cirrhosis, like Child (or Payne) class and MELD
2⃣The 1st tool included an eye-ball test for muscle wasting
3⃣MELD improves with better estimates of kidney risk
16/
This concludes a re-#tweetorial on the prognosis of #cirrhosis and interventions for portal hypertension. I wanted to improve and update one I made in 2019. I am thankful for your feedback then and for reading today.
This concludes a re-#tweetorial on the prognosis of #cirrhosis and interventions for portal hypertension. I wanted to improve and update one I made in 2019. I am thankful for your feedback then and for reading today.
• • •
Missing some Tweet in this thread? You can try to
force a refresh