1/T
As we get closer to the end of the pandemic, it's worthwhile to look back on false claims that helped make the pandemic worse.
One of these claims was:
COVID-19 is not much of a danger to people outside of nursing homes + other institutions.
As we get closer to the end of the pandemic, it's worthwhile to look back on false claims that helped make the pandemic worse.
One of these claims was:
COVID-19 is not much of a danger to people outside of nursing homes + other institutions.
https://twitter.com/AtomsksSanakan/status/1306744573520236544
2/T
John Ioannidis is a proponent of this claim.
He argued that relatively few SARS-CoV-2-infected people died of the disease COVID-19, outside of nursing homes.
In other words: the infection fatality rate, or IFR, was low outside of nursing homes.
institutefordiseasemodeling.github.io/nCoV-public/an…
John Ioannidis is a proponent of this claim.
He argued that relatively few SARS-CoV-2-infected people died of the disease COVID-19, outside of nursing homes.
In other words: the infection fatality rate, or IFR, was low outside of nursing homes.
institutefordiseasemodeling.github.io/nCoV-public/an…

3/T
He defended this idea since at least early May 2020. And he continued to defend it in his most recent work:
"in Europe and the Americas (~0.2% among community-dwelling non-institutionalized people)"
onlinelibrary.wiley.com/doi/10.1111/ec…
medrxiv.org/content/10.110…
sciencedirect.com/science/articl…
He defended this idea since at least early May 2020. And he continued to defend it in his most recent work:
"in Europe and the Americas (~0.2% among community-dwelling non-institutionalized people)"
onlinelibrary.wiley.com/doi/10.1111/ec…
medrxiv.org/content/10.110…
sciencedirect.com/science/articl…

4/T
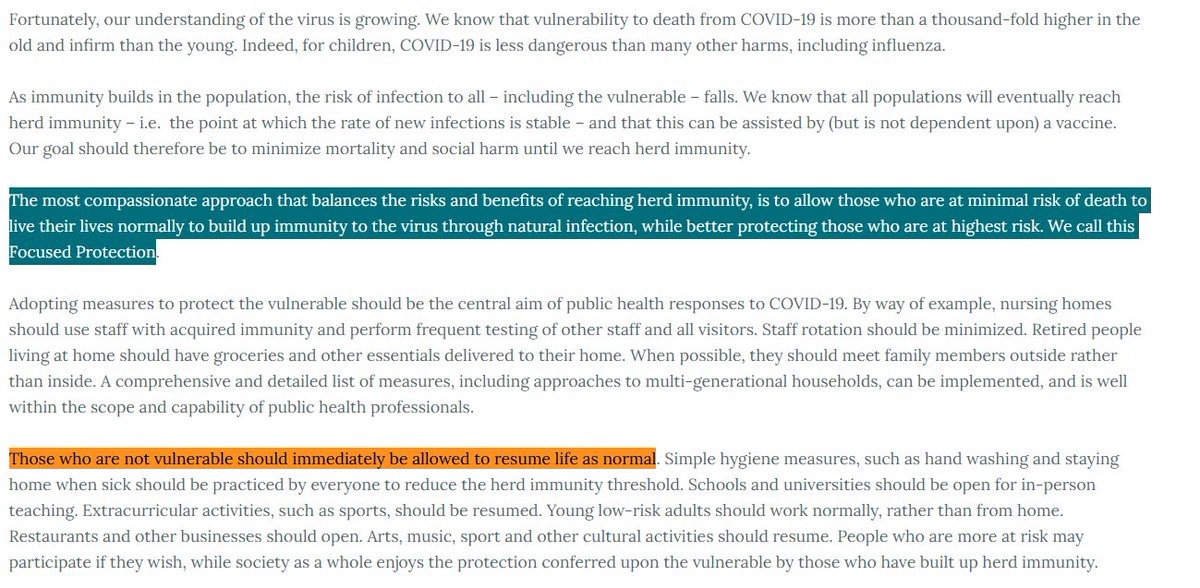
Ioannidis' idea then led to the "focused protection" strategy of the Great Barrington Declaration:
Protect 'vulnerable' people in nursing homes and elsewhere. But impose almost no restrictions on the general population of less 'vulnerable' people.
Ioannidis' idea then led to the "focused protection" strategy of the Great Barrington Declaration:
Protect 'vulnerable' people in nursing homes and elsewhere. But impose almost no restrictions on the general population of less 'vulnerable' people.
https://twitter.com/AtomsksSanakan/status/1368251778114985991

5/T
So a lot hinges on the idea that IFR is low (≤~0.2%) in the Americas and Europe, outside of nursing homes.
If IFR is higher, then letting many people get infected in the general population would lead to a huge pandemic with many COVID-19 deaths.
So a lot hinges on the idea that IFR is low (≤~0.2%) in the Americas and Europe, outside of nursing homes.
If IFR is higher, then letting many people get infected in the general population would lead to a huge pandemic with many COVID-19 deaths.
https://twitter.com/AtomsksSanakan/status/1368258343366578178

6/T
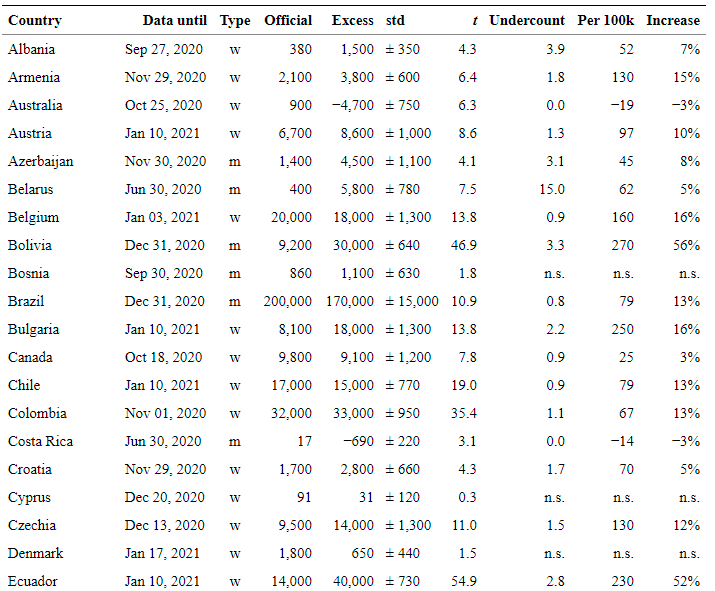
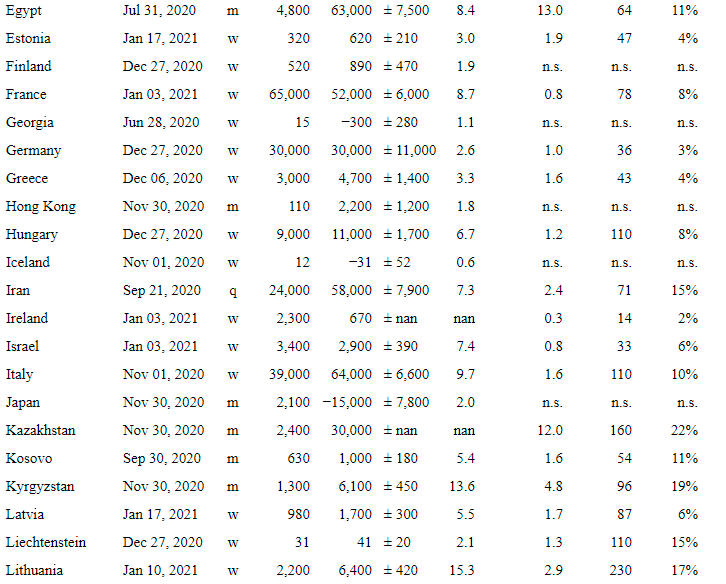
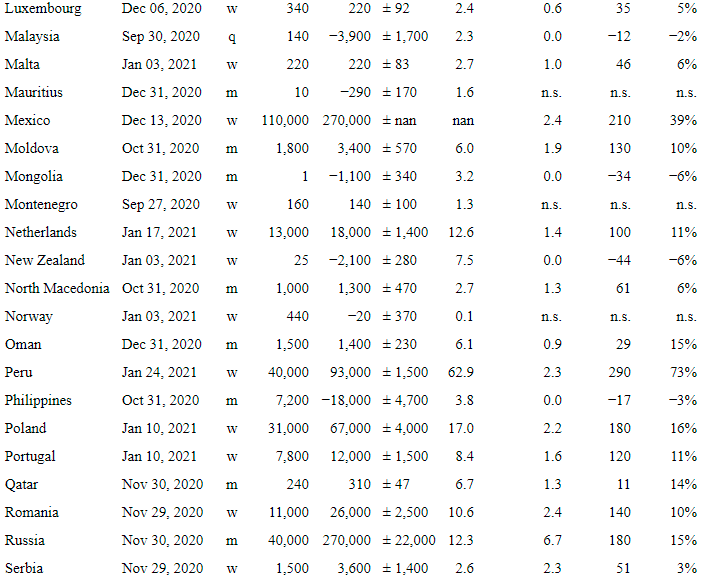
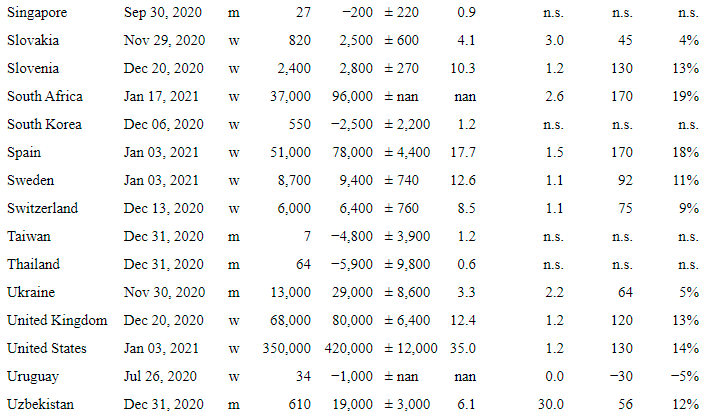
Unfortunately, IFR was ≥0.2% in the Americas + Europe, outside of nursing homes:
0.2% - 0.4%: medrxiv.org/content/10.110…
0.3%: ncbi.nlm.nih.gov/pmc/articles/P… [
0.3%: thelancet.com/journals/lanin… (appendix)
{blue shade: 0.79% (0.68–0.92%)}
nature.com/articles/s4158…
Unfortunately, IFR was ≥0.2% in the Americas + Europe, outside of nursing homes:
0.2% - 0.4%: medrxiv.org/content/10.110…
0.3%: ncbi.nlm.nih.gov/pmc/articles/P… [
https://twitter.com/AtomsksSanakan/status/1301934374842138625]
0.3%: thelancet.com/journals/lanin… (appendix)
{blue shade: 0.79% (0.68–0.92%)}
nature.com/articles/s4158…

7/T
Re: "IFR was ≥0.2% in the Americas + Europe, outside of nursing homes"
0.5%: ncbi.nlm.nih.gov/pmc/articles/P…
0.6%: ncbi.nlm.nih.gov/pmc/articles/P…
0.8%: ncbi.nlm.nih.gov/pmc/articles/P…
0.9%: nature.com/articles/s4146…
1.0%: ncbi.nlm.nih.gov/pmc/articles/P…
1.4%:
medrxiv.org/content/10.110…
Re: "IFR was ≥0.2% in the Americas + Europe, outside of nursing homes"
0.5%: ncbi.nlm.nih.gov/pmc/articles/P…
0.6%: ncbi.nlm.nih.gov/pmc/articles/P…
0.8%: ncbi.nlm.nih.gov/pmc/articles/P…
0.9%: nature.com/articles/s4146…
1.0%: ncbi.nlm.nih.gov/pmc/articles/P…
1.4%:
medrxiv.org/content/10.110…

8/T
Re: "IFR was ≥0.2%"
Parts 6/T + 7/T focused on studies that use representative/randomized sampling.
But even studies with non-representative sampling debunk Ioannidis' idea:
0.6%: medrxiv.org/content/10.110…
0.8%:
medrxiv.org/content/10.110…
Re: "IFR was ≥0.2%"
Parts 6/T + 7/T focused on studies that use representative/randomized sampling.
https://twitter.com/AtomsksSanakan/status/1376002138535563269
But even studies with non-representative sampling debunk Ioannidis' idea:
0.6%: medrxiv.org/content/10.110…
0.8%:
medrxiv.org/content/10.110…

9/T
Ioannidis also performed a misleading comparison of:
- influenza IFR, *including nursing home deaths*
- SARS-CoV-2 IFR, *without nursing home deaths*
That doesn't correct for influenza killing older people in nursing homes.
cdc.gov/flu/about/burd…
Ioannidis also performed a misleading comparison of:
- influenza IFR, *including nursing home deaths*
- SARS-CoV-2 IFR, *without nursing home deaths*
https://twitter.com/AtomsksSanakan/status/1381066842526072832
That doesn't correct for influenza killing older people in nursing homes.
cdc.gov/flu/about/burd…

10/T
So Ioannidis' position, + that of the Great Barrington Declaration, still rests on:
- under-estimating the risk COVID-19 poses to the general population, including outside nursing homes
- misleading comparisons to influenza
So Ioannidis' position, + that of the Great Barrington Declaration, still rests on:
- under-estimating the risk COVID-19 poses to the general population, including outside nursing homes
- misleading comparisons to influenza
https://twitter.com/AtomsksSanakan/status/1378479040877707268
https://twitter.com/AtomsksSanakan/status/1368265513042915332
• • •
Missing some Tweet in this thread? You can try to
force a refresh