So where are we on the rare clotting disorder linked to AZ and J&J shots? What do we know? How do risks and benefits compare? What does it mean long-term and around the world?
@GretchenVogel1 and I tried to answer some questions, thread to come in a bit.
sciencemag.org/news/2021/05/w…
@GretchenVogel1 and I tried to answer some questions, thread to come in a bit.
sciencemag.org/news/2021/05/w…
First off:
This is complex and I‘m tired of people pretending it‘s all obvious.
So a few general points about the decisions that have to be made here:
This is complex and I‘m tired of people pretending it‘s all obvious.
So a few general points about the decisions that have to be made here:
They are
- local, but with global implications
- based on imperfect data in an evolving pandemic
- about individual decisions as well as population-level effects (and these two things can point in opposite directions)
- local, but with global implications
- based on imperfect data in an evolving pandemic
- about individual decisions as well as population-level effects (and these two things can point in opposite directions)
- about rational arguments on risk, when humans are often irrational about risks
- dependent on what alternatives are available
- about perception and politics as well as evidence
- about trust in the processes ensuring vaccine safety as much as trust in one particular vaccine
- dependent on what alternatives are available
- about perception and politics as well as evidence
- about trust in the processes ensuring vaccine safety as much as trust in one particular vaccine
One more note: After VIPIT, then VITT, the name that seems to be taking hold is TTS (thrombosis with thrombocytopenia syndrome) and I’ll use this from now on.
So let’s take AZ (where we have the most data) and look at population level first:
The rate of #TTS observed in countries seems to be somewhere between 1 in 40,000 vaccinations (Norway, Denmark) and 1 in 150,000 (Sri Lanka).
About 1 in 5 of these patients have died.
The rate of #TTS observed in countries seems to be somewhere between 1 in 40,000 vaccinations (Norway, Denmark) and 1 in 150,000 (Sri Lanka).
About 1 in 5 of these patients have died.
The risk of severe #covid19 in the population is clearly higher.
So at a population level the benefits of vaccination with AZ clearly outweigh not vaccinating at all as long as there is transmission.
(Note that this does not apply to say New Zealand which is now using Pfizer)
So at a population level the benefits of vaccination with AZ clearly outweigh not vaccinating at all as long as there is transmission.
(Note that this does not apply to say New Zealand which is now using Pfizer)
This is essentially what WHO’s expert group SAGE said recently:
“In countries with ongoing SARS-CoV-2 transmission, the benefit of vaccination in protecting against COVID-19 far outweighs the risks.”
who.int/publications-d…
“In countries with ongoing SARS-CoV-2 transmission, the benefit of vaccination in protecting against COVID-19 far outweighs the risks.”
who.int/publications-d…
They did add:
“However, benefit–risk assessments may differ from country to country, and countries should consider their epidemiological situation, individual and population-level risks, availability of other vaccines, and alternate options for risk mitigation.”
Context matters!
“However, benefit–risk assessments may differ from country to country, and countries should consider their epidemiological situation, individual and population-level risks, availability of other vaccines, and alternate options for risk mitigation.”
Context matters!
It is more complicated when you get to an individual’s benefit-risk assessment.
First, the risk:
While there is uncertainty about the exact frequency of TTS, it’s essentially a fixed number, on the order of somewhere around 1 in 100,000 say.
First, the risk:
While there is uncertainty about the exact frequency of TTS, it’s essentially a fixed number, on the order of somewhere around 1 in 100,000 say.
Can we identify groups that are at higher risk?
Not yet. Researchers say there is no strong evidence that women or men or younger or older people are at a higher risk. Nor is there a sign that a previous history of blood clotting or even HIT increases risk.
Not yet. Researchers say there is no strong evidence that women or men or younger or older people are at a higher risk. Nor is there a sign that a previous history of blood clotting or even HIT increases risk.
What about the benefit of immunization?
That is clearly higher the older someone is and the higher the level of infections around them.
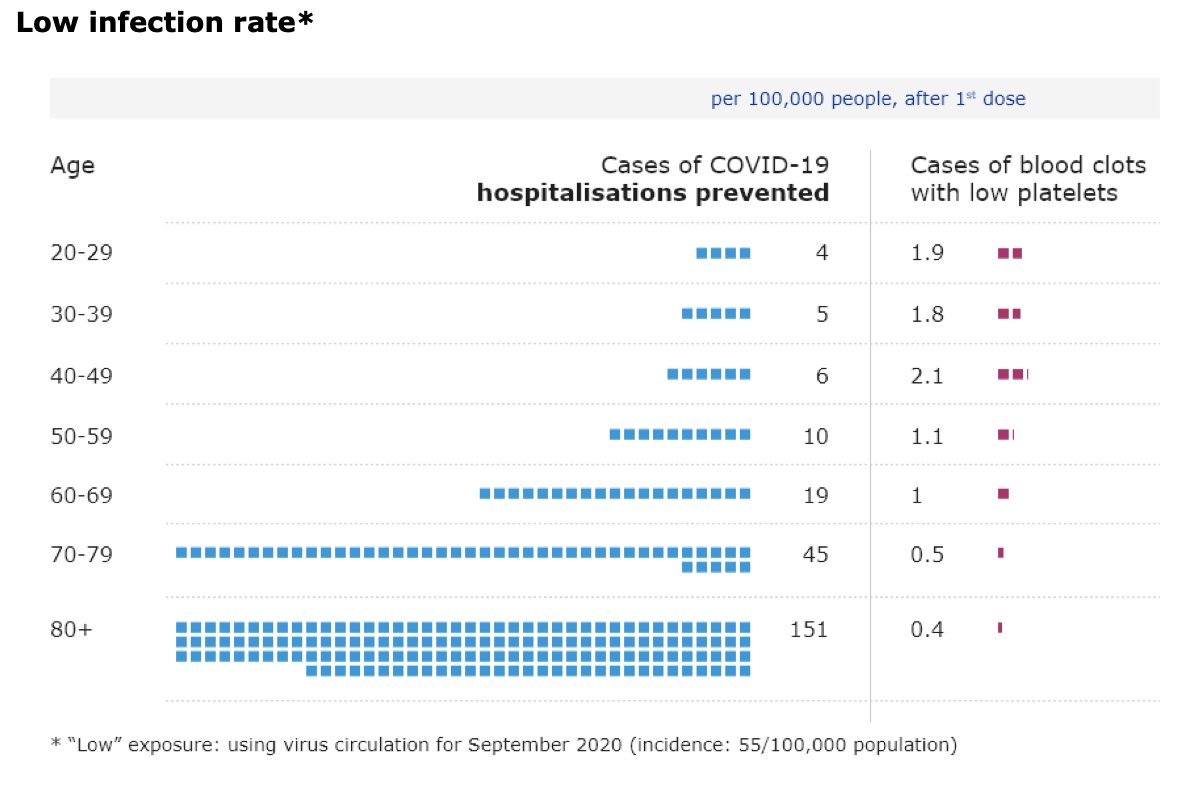
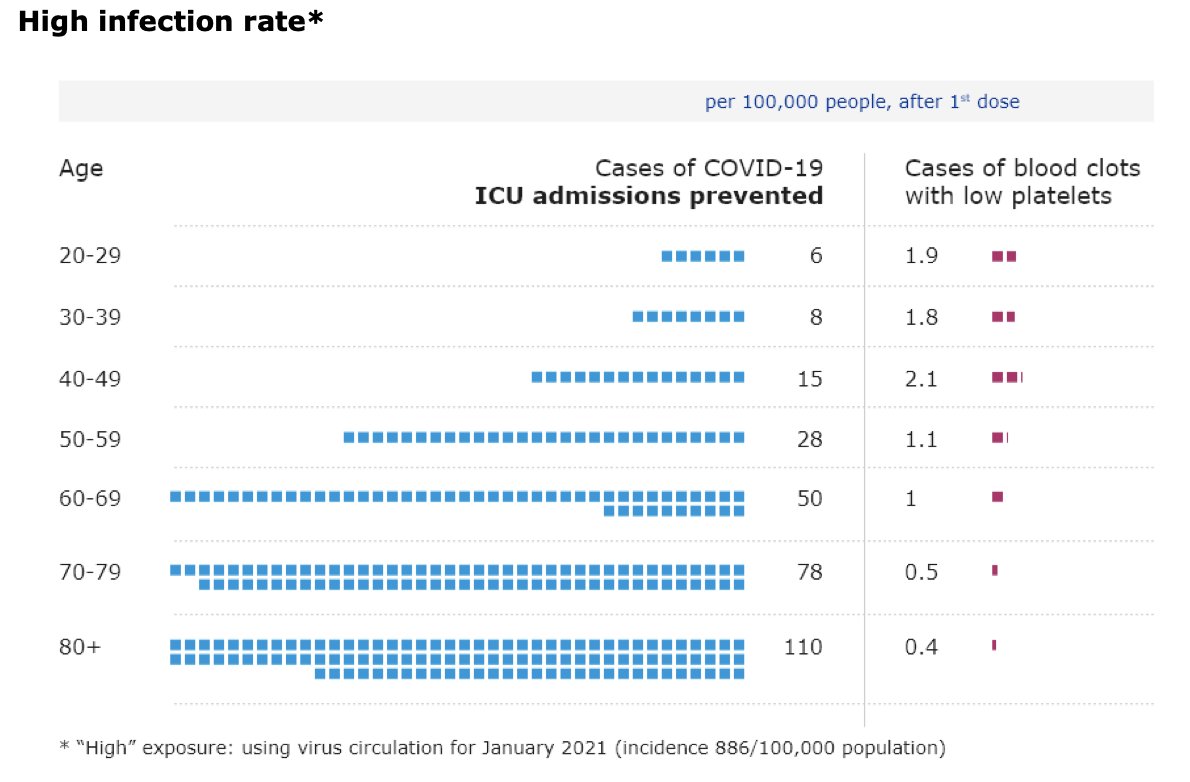
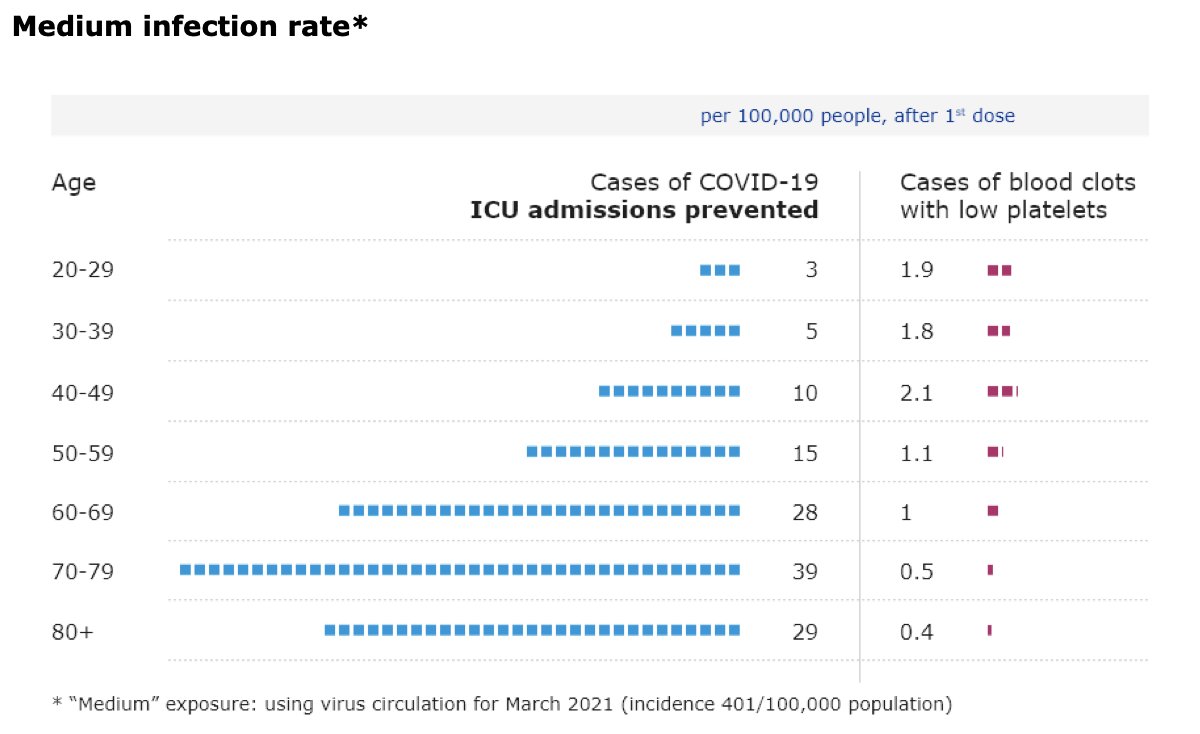
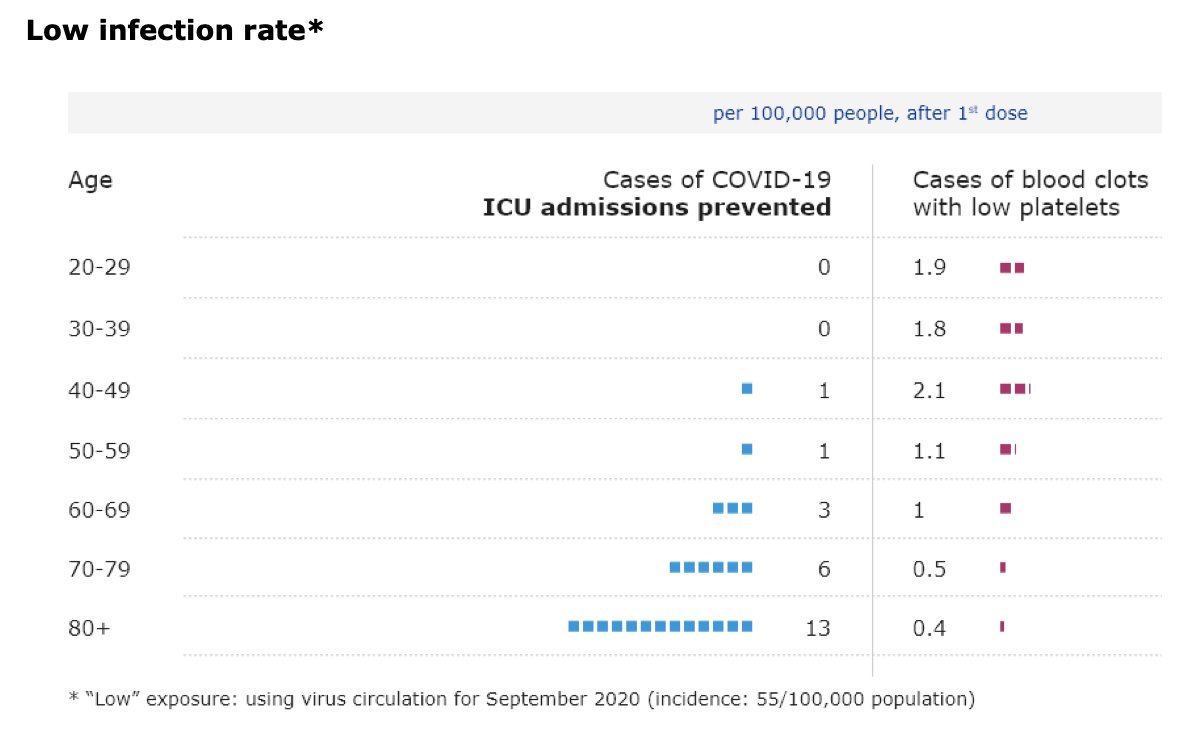
I’ve tweeted graphs from @EMA_News showing how risks and benefits look in different age groups at different infection levels before:
That is clearly higher the older someone is and the higher the level of infections around them.
I’ve tweeted graphs from @EMA_News showing how risks and benefits look in different age groups at different infection levels before:
https://twitter.com/kakape/status/1385595174441660422
We tried to condense this into two tables in our story, one for low-risk (55 infections per 100,000 people per month), one for high-risk (886 infections) setting.
Numbers are per 100,000 people over 4 weeks:
Numbers are per 100,000 people over 4 weeks:


You can see that in young people the benefits and risks over 4 weeks at low infection levels are not all that different.
Of course, hospitalisations and deaths are not everything. “Don’t underestimate the impact of Long COVID,” for instance, @JeremyFarrar told me.
Of course, hospitalisations and deaths are not everything. “Don’t underestimate the impact of Long COVID,” for instance, @JeremyFarrar told me.
@JeremyFarrar One way of thinking about the risk-benefit on an individual basis is:
How many weeks of not being vaccinated add up to the same risk of dying from #covid19 as the risk of dying from #TTS when getting the shot?
How many weeks of not being vaccinated add up to the same risk of dying from #covid19 as the risk of dying from #TTS when getting the shot?
@JeremyFarrar The answer in Norway, for a woman aged between 45 and 49 years, is 79 weeks, according to @camisto.
So it makes sense for a 45 year old woman to wait one and a half years for a different vaccine.
Remember: Norway has few infections and has seen high levels of #TTS!
So it makes sense for a 45 year old woman to wait one and a half years for a different vaccine.
Remember: Norway has few infections and has seen high levels of #TTS!
@JeremyFarrar @camisto So this an extreme case but it lays out the crux of the problem clearly:
On a population level you want everyone vaccinated asap. But on an individual level for some people in some places it makes absolute sense to wait for a different shot.
On a population level you want everyone vaccinated asap. But on an individual level for some people in some places it makes absolute sense to wait for a different shot.
@JeremyFarrar @camisto Again: It's about context. In many places waiting for a different vaccine makes little sense.
As @MPaiMD told us: “Crossing the street is a risk. But if there’s a bear running toward you on your side of the street, that risk suddenly looks different. This virus is a bear.”
As @MPaiMD told us: “Crossing the street is a risk. But if there’s a bear running toward you on your side of the street, that risk suddenly looks different. This virus is a bear.”
@JeremyFarrar @camisto @MPaiMD Two things to consider:
1. What happens long-term?
As immunizations ramp up, infections should hopefully go down and more vaccines become available. So over time more and more places will look a bit more like Norway. And so even this very low risk of TTS will loom larger.
1. What happens long-term?
As immunizations ramp up, infections should hopefully go down and more vaccines become available. So over time more and more places will look a bit more like Norway. And so even this very low risk of TTS will loom larger.
@JeremyFarrar @camisto @MPaiMD 2. Global equity
In many places the luxury of different vaccines is a distant dream. Most countries are desperate for any vaccine.
I'll have to tackle what decisions in Europe/US/Canada mean for these countries and for perceptions of vaccine equity in a separate thread.
In many places the luxury of different vaccines is a distant dream. Most countries are desperate for any vaccine.
I'll have to tackle what decisions in Europe/US/Canada mean for these countries and for perceptions of vaccine equity in a separate thread.
• • •
Missing some Tweet in this thread? You can try to
force a refresh