
1/ Hello #IDtwitter #IDfellows and Welcome to “Opportunistic Mondays”! For the next few Mondays, @KrutiYagnikDO and @johnhannamd will be presenting interesting OI cases with major teaching points. Enjoy! 
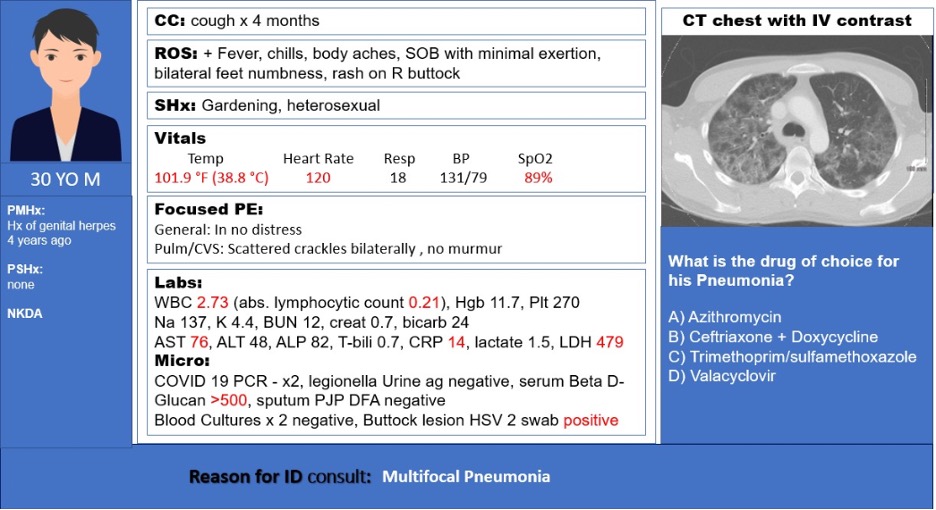
2/ What is the drug of choice for his pneumonia?
3/ + HSV 2 swab from buttock lesion with lymphopenia should prompt HIV screening
HIV ab returned positive; HIV-1 with VL of 790k and CD4 of 10 (5%)
#IDpearls: Pneumocystis Pneumonia (PJP) is the most common respiratory OI in HIV with CD4<200, not on PPx.
HIV ab returned positive; HIV-1 with VL of 790k and CD4 of 10 (5%)
#IDpearls: Pneumocystis Pneumonia (PJP) is the most common respiratory OI in HIV with CD4<200, not on PPx.
4/ In this case, PJP diagnosed as:
- CT w/ widespread heterogeneous pulmonary ground glass opacities & several pulmonary cysts
- Elevated LDH (>200, high sensitivity, low specificity)
- >500 BDG
Check out pubmed.ncbi.nlm.nih.gov/31434728/ regarding pros and cons of BDG
- CT w/ widespread heterogeneous pulmonary ground glass opacities & several pulmonary cysts
- Elevated LDH (>200, high sensitivity, low specificity)
- >500 BDG
Check out pubmed.ncbi.nlm.nih.gov/31434728/ regarding pros and cons of BDG
5/ More #IDpearls
Induced sputum PJP DFA yield is 50-90% in HIV patients. Can’t always rely on this.
BAL PJP DFA yield of >90% in HIV patients.
Both yields are lower in non-HIV patients. pubmed.ncbi.nlm.nih.gov/24667822/
Induced sputum PJP DFA yield is 50-90% in HIV patients. Can’t always rely on this.
BAL PJP DFA yield of >90% in HIV patients.
Both yields are lower in non-HIV patients. pubmed.ncbi.nlm.nih.gov/24667822/
6/ Imaging for PJP:
Typically: bilateral interstitial infiltrates. Can also see cysts, nodules, pneumothorax
However, LAD or pleural effusion are not typically seen with PJP
CT chest is much more sensitive, so a negative CT chest likely rules this diagnosis out
Typically: bilateral interstitial infiltrates. Can also see cysts, nodules, pneumothorax
However, LAD or pleural effusion are not typically seen with PJP
CT chest is much more sensitive, so a negative CT chest likely rules this diagnosis out
7/ PJP Treatment in HIV: ABx + ART (if possible) +/- steroids (based on severity)
ABx choice: TMP/SXZ (15-20mg/kg/d of TMP in 3-4 doses) PO or IV x 21d.
Alternatives: (Clindamycin + primaquine) or (Dapsone + TMP) [for mild-mod] or atovaquone [mild] or IV pentamidine-severe
ABx choice: TMP/SXZ (15-20mg/kg/d of TMP in 3-4 doses) PO or IV x 21d.
Alternatives: (Clindamycin + primaquine) or (Dapsone + TMP) [for mild-mod] or atovaquone [mild] or IV pentamidine-severe
8/ Don’t forget the steroids!
Steroids indications for PJP:
-PaO2 <70 on RA
&/or
-A-a O2 gradient >= 35
Steroids indications for PJP:
-PaO2 <70 on RA
&/or
-A-a O2 gradient >= 35
9/ Don’t forget to start PPx after treatment as this is a common cause for relapse!
1ry PPx indicated for CD4 <200 or CD4% <14%
2ry PPx post PJP infection recommended till CD4 >200 for 3m or more
(Agent of choice TMP-SMX; alt: dapsone, atovaquone, inhaled pentamidine)
1ry PPx indicated for CD4 <200 or CD4% <14%
2ry PPx post PJP infection recommended till CD4 >200 for 3m or more
(Agent of choice TMP-SMX; alt: dapsone, atovaquone, inhaled pentamidine)
10/ Guidelines mention that individuals who are consistently virally suppressed > 6 months can consider stopping PJP ppx if CD4 > 100 but fails to rise above 200. This is based on this study: academic.oup.com/cid/advance-ar…
11/ Other distractors:
Azithromycin would be an appropriate choice for atypicals including Legionella
Ceftriaxone + (azithromycin or doxycycline) is the regimen recommended for CAP
Azithromycin would be an appropriate choice for atypicals including Legionella
Ceftriaxone + (azithromycin or doxycycline) is the regimen recommended for CAP
12/ Other distractors:
HSV PNA presents with multifocal ground-glass predominantly peri-bronchial on CT chest.
HSV PNA is rare. IV acyclovir is the most widely used and effective therapy.
HSV PNA presents with multifocal ground-glass predominantly peri-bronchial on CT chest.
HSV PNA is rare. IV acyclovir is the most widely used and effective therapy.
• • •
Missing some Tweet in this thread? You can try to
force a refresh





