
TODAY’S (6月20日) #COVID19 update for #Taiwan 🇹🇼
📉107 local + 2 imported cases 📉trend
📉11 deaths 📉trend
📈0.6% test positive rate
📈4.1% case fatality rate (CFR) since May 1
🧪20k tests ⤵️capacity
⚠️Fewer cases BUT many fewer tests, higher positivity, and higher CFR. ⬇️ 1/6
📉107 local + 2 imported cases 📉trend
📉11 deaths 📉trend
📈0.6% test positive rate
📈4.1% case fatality rate (CFR) since May 1
🧪20k tests ⤵️capacity
⚠️Fewer cases BUT many fewer tests, higher positivity, and higher CFR. ⬇️ 1/6

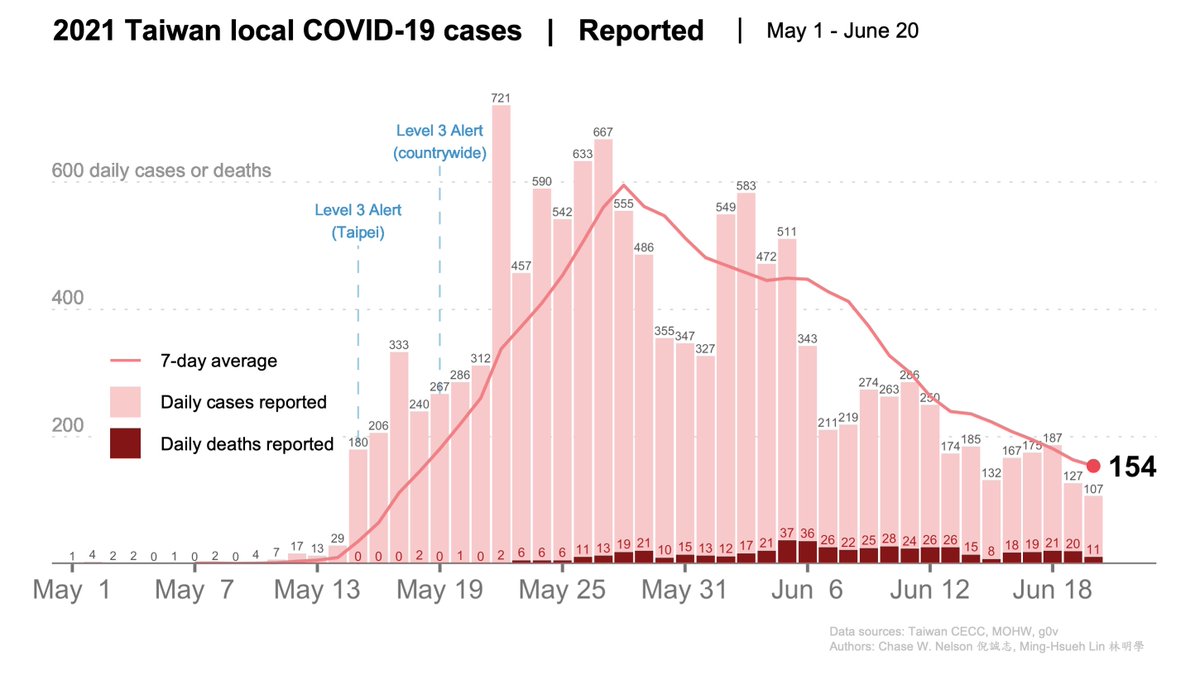
DAILY CASES REPORTED (pink bars) and their 7-DAY AVERAGE (pink line), where each day is the mean of itself and the previous six. DEATHS (crimson red bars) at the bottom.
AGE DISTRIBUTION OF DEATHS for May 1-June 20:
🔴64% are ≥70
🔴26% are 60-69
🔴10% are 30-59 years
2/6
AGE DISTRIBUTION OF DEATHS for May 1-June 20:
🔴64% are ≥70
🔴26% are 60-69
🔴10% are 30-59 years
2/6
AGE DISTRIBUTION OF CASES. Local cases from May 1-June 19 (age data for cases lag by a day), including those with missing locations. Only a single category is provided for ages >70, which constitute 14% of all cases. DATA ➡️ data.cdc.gov.tw/en/dataset/ags… 3/6

Our local case fatality rate for May 1-June 19 is 4.1%—sadly another new record for us, and higher than the world average of 1-3%. This is at least partly due to a disproportionate number of older cases, but also possibly indicative of undetected cases. 4/6

CASES & DEATHS and their 7-DAY AVERAGE BY AGE for May 1-June 19 (latest age-matched data available). Mostly good news. Keeping eyes peeled for 1) a spike 1-2 weeks after Dragon Boat, when some traveled of necessity and 2) workplace clusters due to lack of #WorkFromHome. 5/6

I'm a migrant. So are many of you. Some of us are being packed in #Miaoli #Taiwan dorm rooms while forbidden to go outside or speak. Stop turning a blind eye and END this GROSS HUMAN RIGHTS VIOLATION and international disgrace, @iingwen @eballgogogo. nytimes.com/2021/06/18/wor… 6/6
• • •
Missing some Tweet in this thread? You can try to
force a refresh












