1. Most of us do not really appreciate how resilient children and their immune systems are when they encounter #sarscov2. Most kids don’t even realize they have been exposed, which leads to ⬆️⬆️⬆️ over-estimation of the long-term effects of #COVID19 in children
Here’s why … 🧵
Here’s why … 🧵
2/ when asked, most parents don’t even realize when they child was exposed to #SARS_CoV_2 because most kids either remain asymptomatic or have such a mild and transient illness that parents don’t even associate the illness with #COVID19
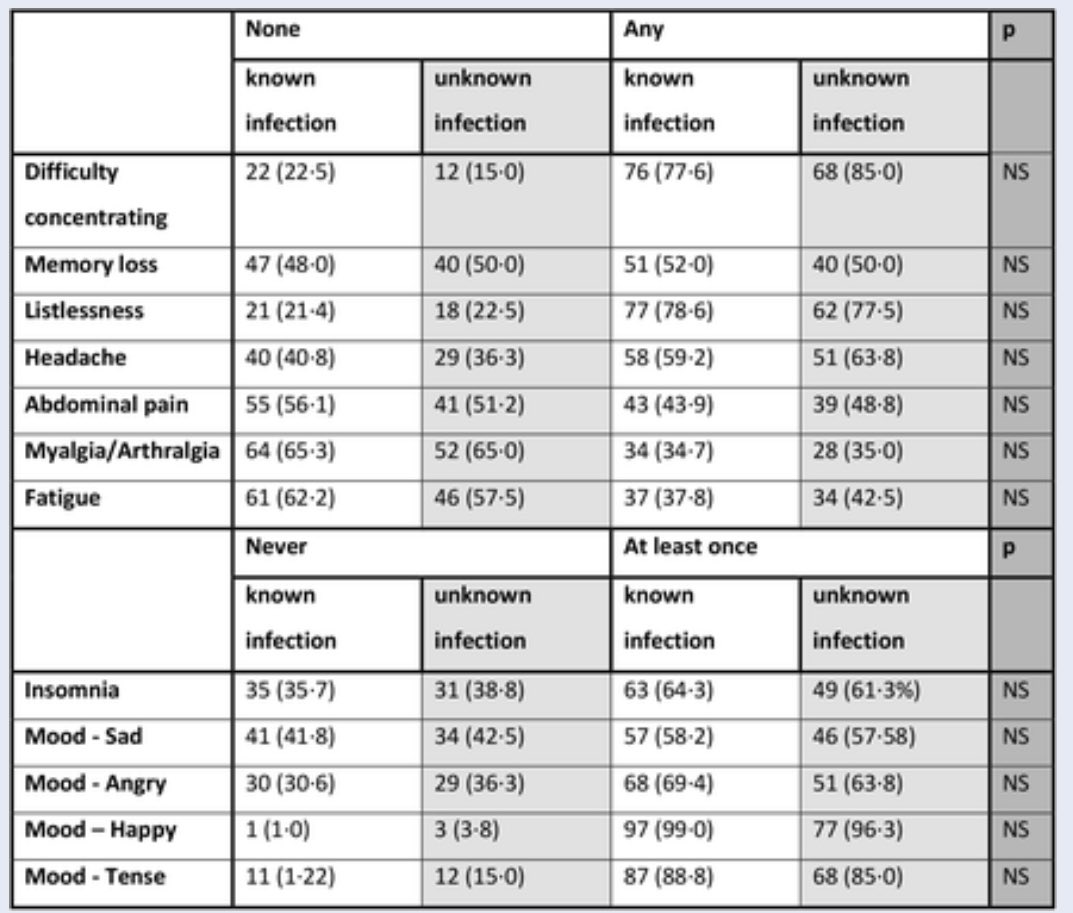
3/ In our primary schools study, although small numbers, parents reported no symptoms in 85% of kids who didn’t have #SARS_CoV_2 antibodies at start of the study & then developed antibodies during the study (ie. got infected) compared to 47% of staff
👉 thelancet.com/journals/lanch…
👉 thelancet.com/journals/lanch…
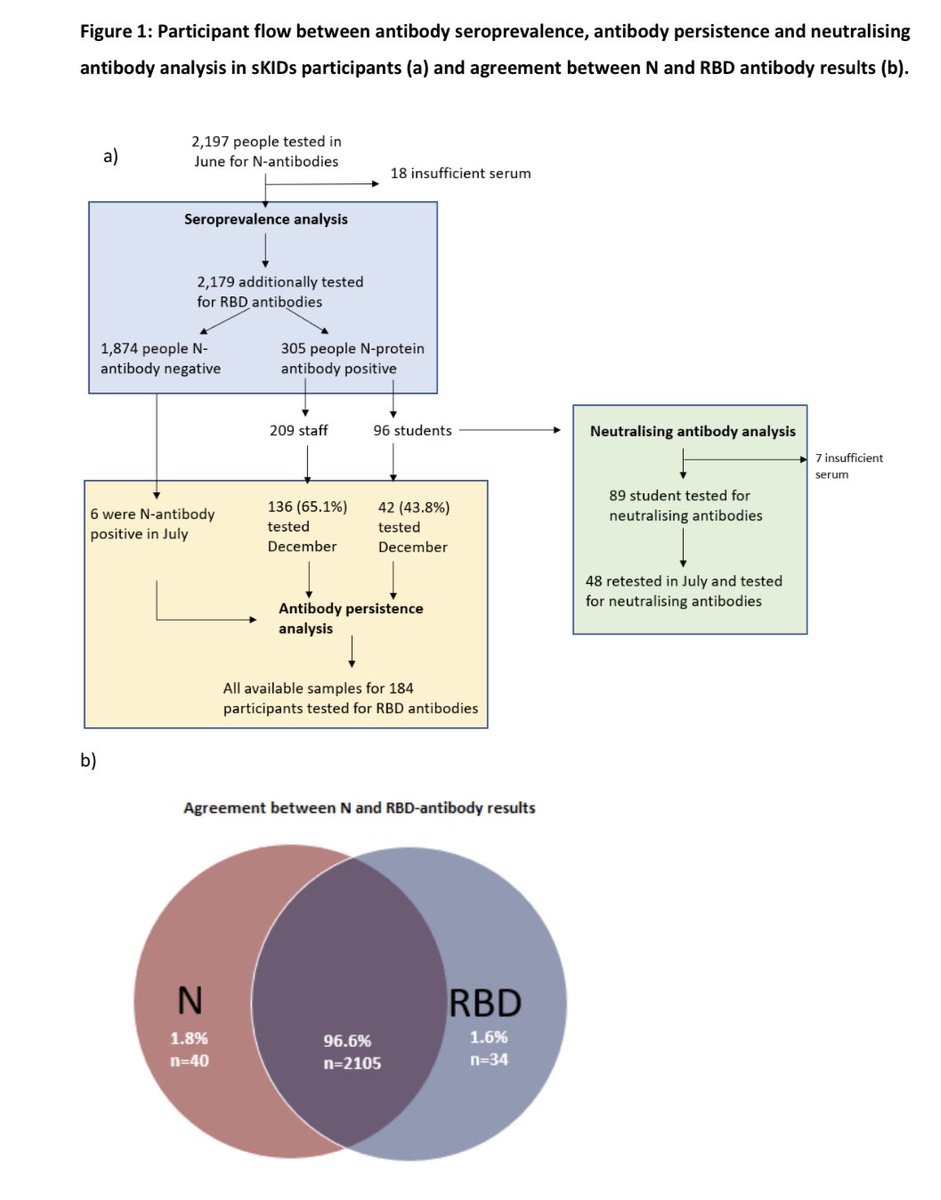
4/ In secondary schools too, although small numbers again, 67% of students who seroconverted (got infected & developed #SARSCoV2 antibodies) during the study reported having no symptoms at all compared to 24% of staff
👉 thelancet.com/journals/eclin…
👉 thelancet.com/journals/eclin…
5/ Importantly, antibody responses after symptomatic & asymptomatic infection in students were indistinguishable 👉 even asymptomatic infection leads to robust immune responses in kids, both in terms of amount of antibody & their ability to kill virus 👉 medrxiv.org/content/10.110…
6/ Also, some kids appear to have T cell (cellular) immunity against #SARS_CoV_2 even without antibodies against the virus. We think this might reflect cross-protection from previous coronavirus infections but this needs further work for confirmation 👉 medrxiv.org/content/10.110… 

7/ So, when trying to estimate risk of severe #COVID19 or #LongCovid, remember that most kids do not even develop any symptoms after virus exposure & some kids may be inherently protected from cellular immunity. Surely these kids can’t be at risk of severe or long covid.
End
End
• • •
Missing some Tweet in this thread? You can try to
force a refresh