
A change in definitions of vaccinated status & new raw data from @IsraelMOH demanded a refreshed approach to my #Israel's #SARS2 charts. I start with general population totals of the four available daily datasets: NEW cases, severely ill & deaths, and ACTIVE severely ill.
1/
1/

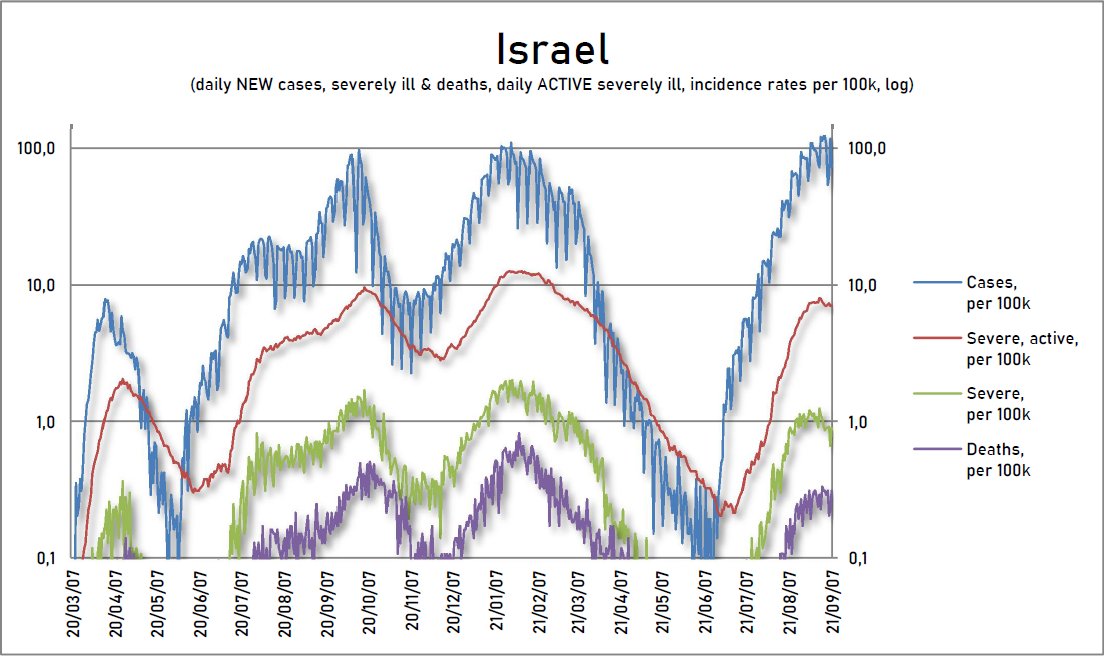


Due to the different sizes of these categories, I had to use log charts. Daily NEW cases, severe & deaths jump around wildly depending on the day of the week, so I'll (mostly) use the standard 7-day rolling averages of both the absolute numbers & the incidence rates.
2/
2/

It's fascinating to see how much the beginnings of this & last year's waves resemble each other. After a prolonged period of new cases below active severely ill, a sudden outbreak above that range signals the start of a huge new wave. A policy reaction is a must at THAT point.
3/
3/

Infections lead with significant time lags on the way up, in logical order. Less so on the way down! If a wave is truly subsiding (not just some testing quirk), EVERY measure should start falling soon, though cases much more pronounced than severe hospitalizations & deaths.
4/
4/

Looking at incidence, Israel topped out again at 100 per 100k. Confirmed infections depend on testing (which Israel does a lot), but, curiously, this level of daily cases of 1‰ (one permille, 1/1000, or 0.1%) of the total population often acts as a ceiling in this pandemic.
5/
5/

In the worst managed outbreaks, daily cases breach this 1‰ of the population ceiling, but the wave has a hard time staying above it before exhausting itself.
Also, 1 per 100k incidence for severe & deaths often delineates how is a country handling its current #SARSCoV2 wave.
6/
Also, 1 per 100k incidence for severe & deaths often delineates how is a country handling its current #SARSCoV2 wave.
6/

If I use 7-day averages for new cases, severe & deaths, the dynamics of this pandemic are more clearly visible. It also shows how #SARS2 manages to fool everyone by falling so low to appear beaten and then exponentially exploding x1000 higher in incidence in just two months.
7/
7/

Sometimes I'll use rolling weekly totals for new severe & deaths because daily zeros mess up calculations & plots. It this chart, it's even better visible how low the numbers fell, just as the current outbreak was, in fact, beginning.
#SARSCoV2 is playing mind games with us!
8/
#SARSCoV2 is playing mind games with us!
8/

Also, look at how weekly totals of new severe mirror active severe when a wave is rising. But, the moment the trend breaks, NEW severe cases separate downward & start decreasing first. That is happening now in Israel. With boosters, they managed to speed up this downtrend.
9/
9/
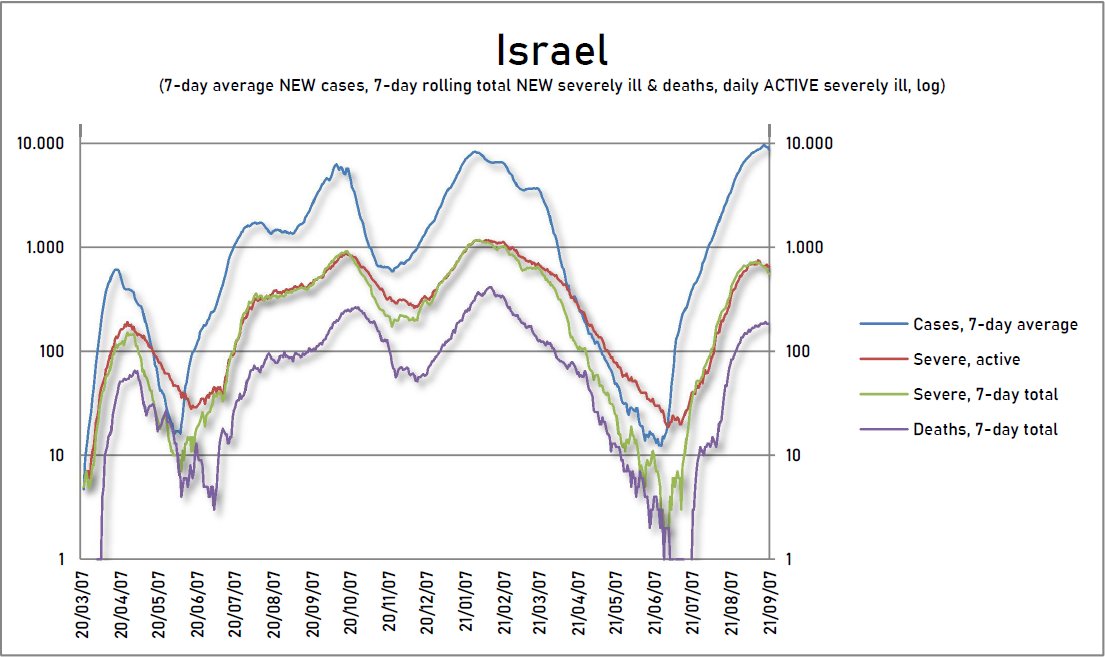
Finally, thanks to the first-class data & the use of logic, #Israel spotted the problem quickly, and without much waiting, implemented a booster campaign while deaths were STILL VERY LOW, at only around 10 per week. If they reacted slower, the consequences would be harsher.
10/
10/

These are the links to my previous threads about #Israel's raw data, containing the history, sources & my methodology for calculating & plotting all these charts.
11/11
https://twitter.com/x2IndSpeculator/status/1434864237214674946?s=20
https://twitter.com/x2IndSpeculator/status/1433034771114889224?s=20
https://twitter.com/x2IndSpeculator/status/1424544518632771584?s=20
11/11
• • •
Missing some Tweet in this thread? You can try to
force a refresh






