Bloody Hell: GI Bleed Management in the ED at #ACEP21 

Upper vs Lower GIB at #ACEP21
Low BP = Assume UGIB
BRBPR w/Clots = LGIB
BUN/Cr >30 = UGIB
NGL = NOT Helpful
Low BP = Assume UGIB
BRBPR w/Clots = LGIB
BUN/Cr >30 = UGIB
NGL = NOT Helpful

EVEN GI guidelines don't support NGL #ACEP21
The American College of Gastroenterology 2012 guidelines state NGL is not required in pts with UGIB for diagnosis, prognosis, visualization, or therapeutic effect
The American College of Gastroenterology 2012 guidelines state NGL is not required in pts with UGIB for diagnosis, prognosis, visualization, or therapeutic effect

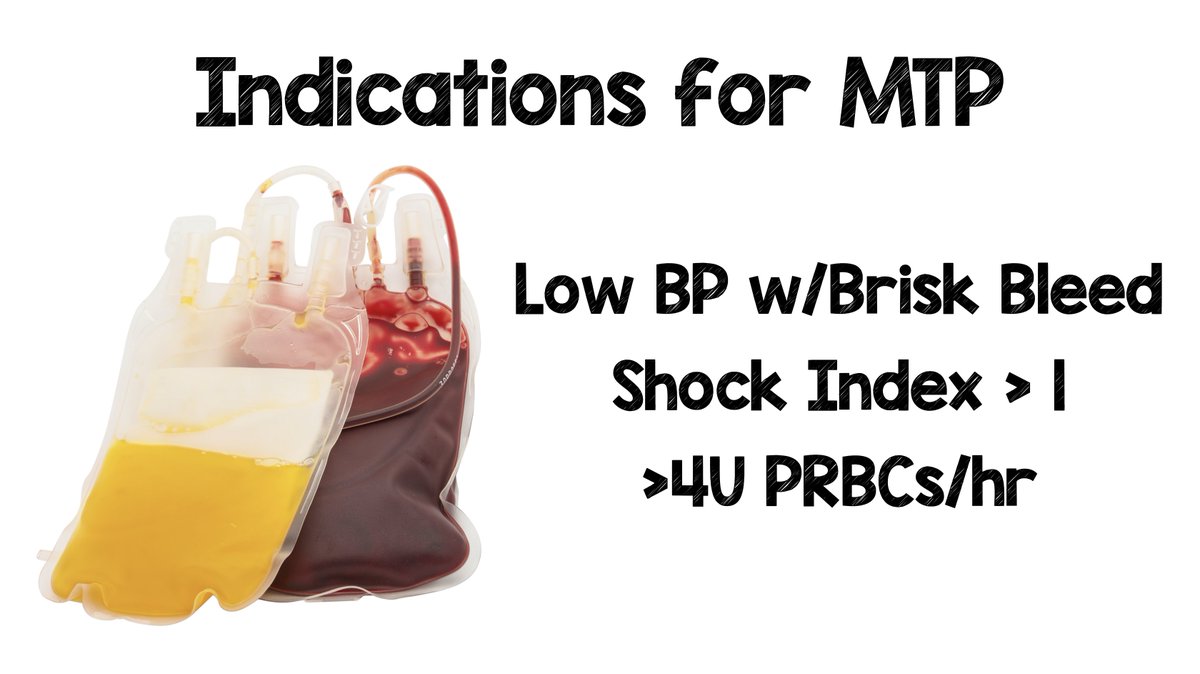
Indications for Massive Transfusion Protocol (MTP) in GIB #ACEP21
-Low BP w/Brisk Bleed
-Shock Index >1
- >4U PRBCs/hr
-Low BP w/Brisk Bleed
-Shock Index >1
- >4U PRBCs/hr
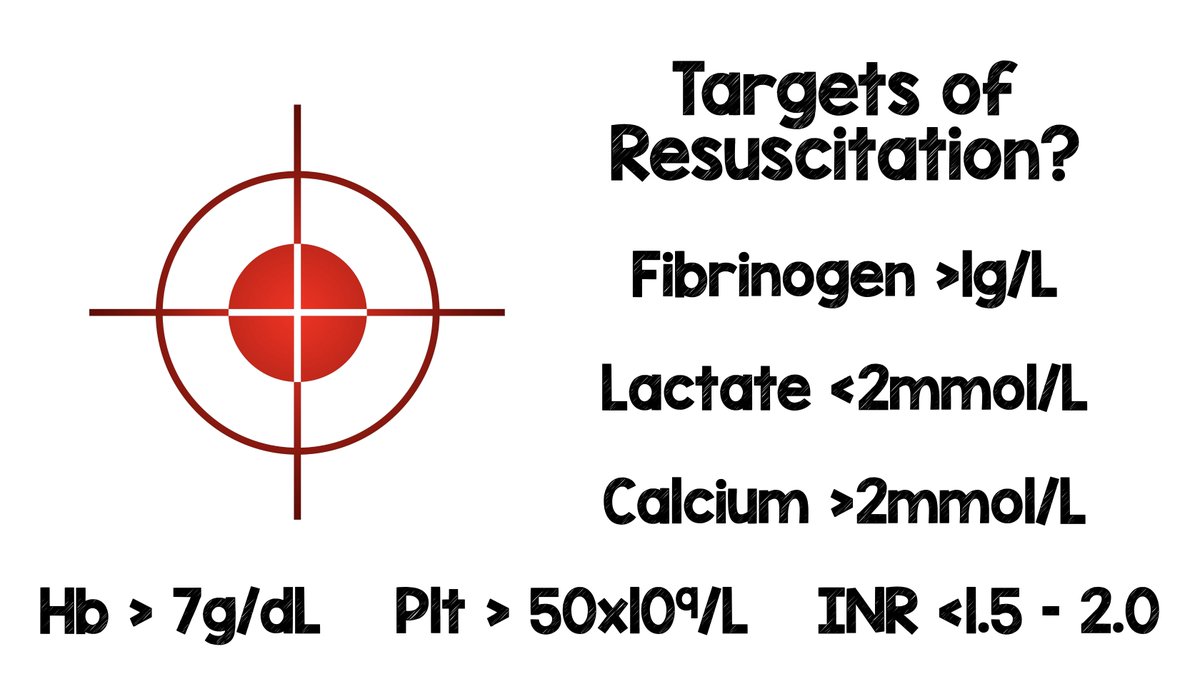
Targets of Resuscitation for GIB #ACEP21
-Extrapolated from Trauma Lit
-Hb >7g/dL
-Plt >50k
-INR <1.5 - 2.0
-Fibrinogen >1g/L
-Lactate <2mmol/L
-Calcium >2mmol/L
-Extrapolated from Trauma Lit
-Hb >7g/dL
-Plt >50k
-INR <1.5 - 2.0
-Fibrinogen >1g/L
-Lactate <2mmol/L
-Calcium >2mmol/L
What to Transfuse in GIB #ACEP21
-Hb <7 --> PRBCs
-Plt <50k --> Plts
-INR >1.8 --> FFP
-Fibrinogen <1 --> Cryo
-Hb <7 --> PRBCs
-Plt <50k --> Plts
-INR >1.8 --> FFP
-Fibrinogen <1 --> Cryo

Octreotide #ACEP21
-In sickest pts, until better data refutes...
-DECREASES bleeding
-DECREASES need for surgery
-NO real mortality data
-In sickest pts, until better data refutes...
-DECREASES bleeding
-DECREASES need for surgery
-NO real mortality data

Proton Pump Inhibitors (PPIs) #ACEP21
-PPI + PUD --> No Diff in Mort; Reduces rebleeding
-PPI + Undiff UGIB --> No Diff in mortality or rebleeding
-PPI Bolus = Drip
-PPI + PUD --> No Diff in Mort; Reduces rebleeding
-PPI + Undiff UGIB --> No Diff in mortality or rebleeding
-PPI Bolus = Drip

Antibiotic Prophylaxis in Cirrhotic Patients #ACEP21
-REDUCES: Mortality, Bacterial Infxns, Rebleeding, & Hospital LOS
-Mortality NNT = 22
-Bacterial Infections NNT = 4
-REDUCES: Mortality, Bacterial Infxns, Rebleeding, & Hospital LOS
-Mortality NNT = 22
-Bacterial Infections NNT = 4


Erythromycin in UGIB #ACEP21
-250mg, 30min prior to EGD IMPROVES:
-Visualization
-Decreased need for 2nd EGD
-Need for PRBCs
-Hospital LOS
-250mg, 30min prior to EGD IMPROVES:
-Visualization
-Decreased need for 2nd EGD
-Need for PRBCs
-Hospital LOS

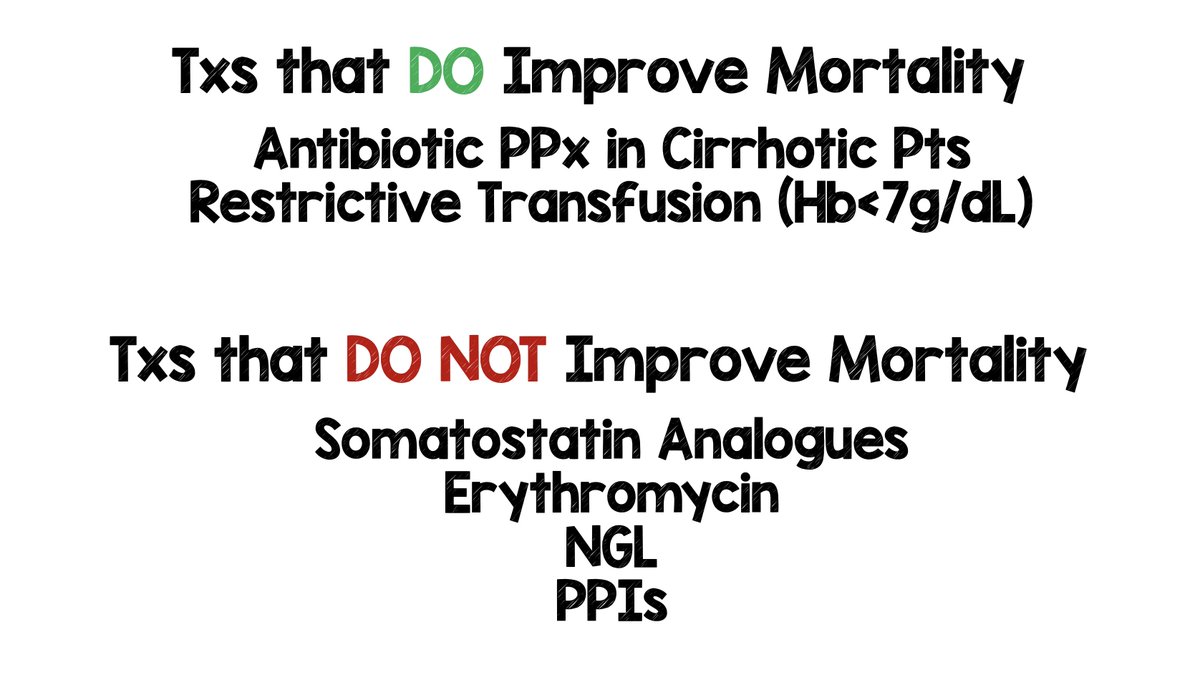
Treatments that DO & DO NOT Improve Mortality in GIB #ACEP21
-DO IMPROVE
-Antibiotic PPx in Cirrhotic Pts
-Restrictive Transfusion (Hb<7g/dL) in HD stable pts
-DO NOT IMPROVE
-Somatostatin Analogues
-Erythromycin
-NGL
-PPIs
-DO IMPROVE
-Antibiotic PPx in Cirrhotic Pts
-Restrictive Transfusion (Hb<7g/dL) in HD stable pts
-DO NOT IMPROVE
-Somatostatin Analogues
-Erythromycin
-NGL
-PPIs
TAKE HOME MESSAGES in GIB #ACEP21
-HD Unstable, Hematemesis, BUN/Cr >30 = Assume UGIB
-BRPBR + Clots = Assume LGIB
-NGL = Painful and Doesn't Help
-HD Unstable, Hematemesis, BUN/Cr >30 = Assume UGIB
-BRPBR + Clots = Assume LGIB
-NGL = Painful and Doesn't Help
TAKE HOME MESSAGES in GIB #ACEP21
-Abx PPx in Cirrhotics = Saves Lives
-Octreotide = Decreases Bleeding and Need for Surgery
-PPI: Bolus = Drip
-Erythromycin = Helps with Visualization During EGD
-Abx PPx in Cirrhotics = Saves Lives
-Octreotide = Decreases Bleeding and Need for Surgery
-PPI: Bolus = Drip
-Erythromycin = Helps with Visualization During EGD

TAKE HOME MESSAGES in GIB #ACEP21
-HD Stable GIB = Restrictive Transfusion (Hb<7)
-HD Unstable GIB = Transfuse Regardless of Hb
-Know Indications for Massive Transfusion Protocol
-HD Stable GIB = Restrictive Transfusion (Hb<7)
-HD Unstable GIB = Transfuse Regardless of Hb
-Know Indications for Massive Transfusion Protocol
• • •
Missing some Tweet in this thread? You can try to
force a refresh