Yesterday, Premier Moe said #COVID19 cases in Saskatchewan are more frequent in the vaccinated vs. those who aren't.
THUS, vaccines DON'T prevent infection with or transmission of Omicron.
The Premier's conclusions are INCORRECT. But why?
It's complicated. Here we go.
🧵 /1
THUS, vaccines DON'T prevent infection with or transmission of Omicron.
The Premier's conclusions are INCORRECT. But why?
It's complicated. Here we go.
🧵 /1
The Premier's incorrect conclusion stems from a simplistic interpretation of the data. 'Base rate fallacy' is one problem, but there are MANY other factors at play.
We explained 'base rate fallacy' with cases & vax status back in August. See below. /2
We explained 'base rate fallacy' with cases & vax status back in August. See below. /2
https://twitter.com/awong37/status/1429084212276178951
For 'base rate fallacy' & #COVID19 & hospitalizations, this is the diagram EVERYONE uses (thx @MarcRummy).
MANY more people are fully vaccinated now, so even though a small proportion of them go to hospital, the absolute numbers are the same as those unvaccinated. See below. /3
MANY more people are fully vaccinated now, so even though a small proportion of them go to hospital, the absolute numbers are the same as those unvaccinated. See below. /3

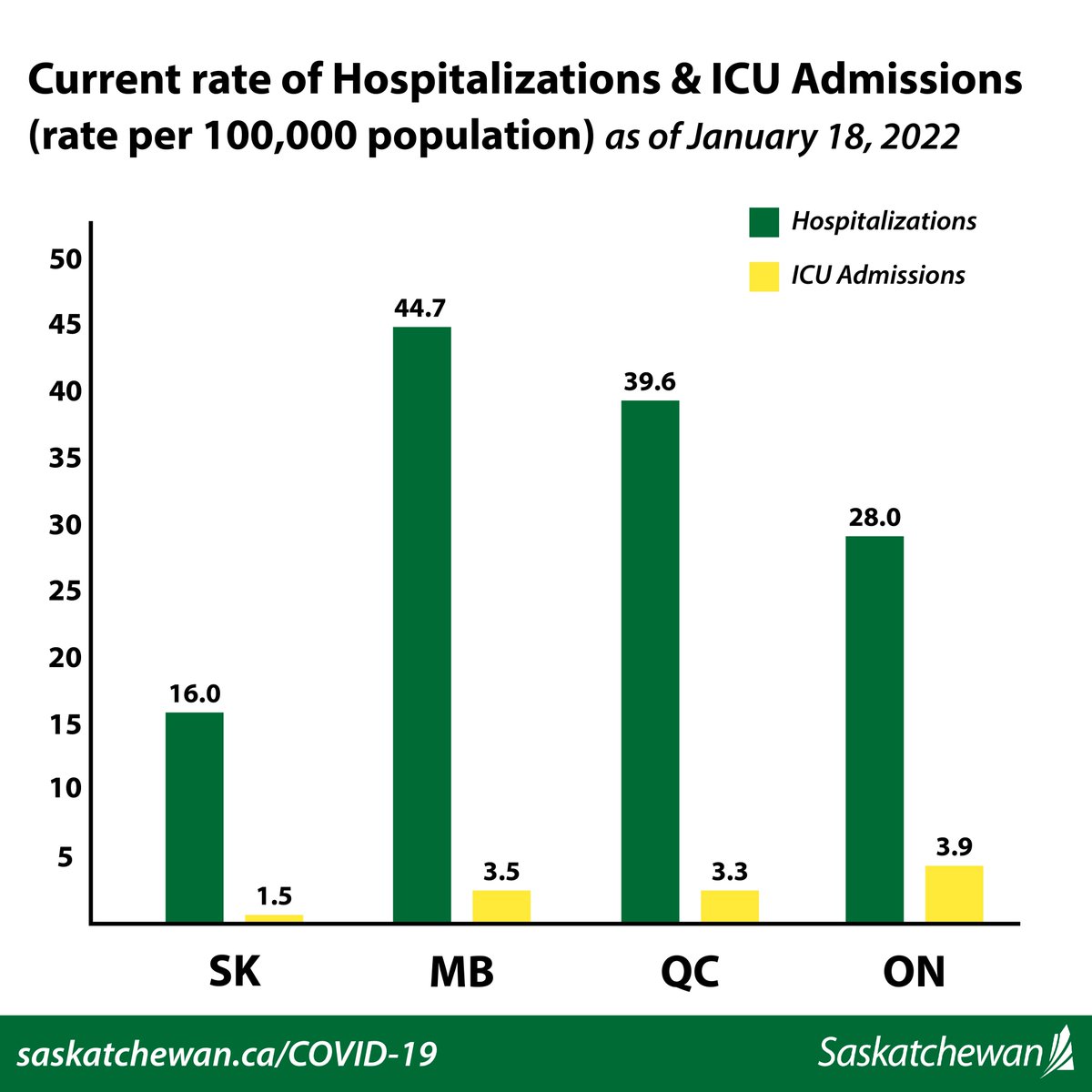
Premier Moe HAS said #COVID19 vaccines DO significantly reduce severe illness & hospitalizations. 100% correct.
363 are in #SK hospitals, 112 are NOT fully vaccinated. 251 are. What?
Does that mean vaccines DON'T work to prevent hospitalization? No! BECAUSE of *base* rates. /4
363 are in #SK hospitals, 112 are NOT fully vaccinated. 251 are. What?
Does that mean vaccines DON'T work to prevent hospitalization? No! BECAUSE of *base* rates. /4
OK, let's sort vaccine numbers for Saskatchewan. As of today, 2,293,176 doses have been administered in total. So:
- 216,513 (18.35%) are unvaccinated
- 67,374 (5.71%) have 1 dose
- 462,273 (39.18%) have 2 doses
- 433,752 (36.76%) have 3 or more doses
/5
- 216,513 (18.35%) are unvaccinated
- 67,374 (5.71%) have 1 dose
- 462,273 (39.18%) have 2 doses
- 433,752 (36.76%) have 3 or more doses
/5
Let's look at case numbers now. I can't find historic case numbers by vaccine status on #SK dashboard. Thankfully, @OkayArbiter has recorded them day-by-day.
Today's graph is below. The graphs show the *prevalence* of cases per 100,000 persons by vaccine status. /6
Today's graph is below. The graphs show the *prevalence* of cases per 100,000 persons by vaccine status. /6

Extrapolating @OkayArbiter's chart data from today:
0 doses: ~110 per 100,000
1 dose: ~70 per 100,000
2+ doses: ~140 per 100,000
3+ doses: ~80 per 100,000
So currently the highest rate of cases is occurring in persons w/ 2+ doses. The lowest is in persons with 1 dose.
Huh? /7
0 doses: ~110 per 100,000
1 dose: ~70 per 100,000
2+ doses: ~140 per 100,000
3+ doses: ~80 per 100,000
So currently the highest rate of cases is occurring in persons w/ 2+ doses. The lowest is in persons with 1 dose.
Huh? /7
Here's where it gets complicated.
We need to understand the caveats & limitations of the data in question.
It's NOT just base rate fallacy any longer, otherwise the numbers above wouldn't make sense.
We need to think about Omicron, waning immunity, and PCR testing in #SK. /8
We need to understand the caveats & limitations of the data in question.
It's NOT just base rate fallacy any longer, otherwise the numbers above wouldn't make sense.
We need to think about Omicron, waning immunity, and PCR testing in #SK. /8
First, Omicron.
2 doses, esp. if your 2nd dose was given >5-6 months ago, likely provides MINIMAL protection vs. Omicron infection.
Pre-print data from #ON colleagues suggests ZERO protection vs. Omicron infection w/ 2 doses >180 days post 2nd dose. /9
medrxiv.org/content/10.110…
2 doses, esp. if your 2nd dose was given >5-6 months ago, likely provides MINIMAL protection vs. Omicron infection.
Pre-print data from #ON colleagues suggests ZERO protection vs. Omicron infection w/ 2 doses >180 days post 2nd dose. /9
medrxiv.org/content/10.110…
Similar data has been published worldwide. Unfortunately, vaccine effectiveness vs. Omicron infection wanes quickly following a 2nd dose of vaccine.
In the #ON study between 7-59 days post 2nd dose, only 36% protection was achieved vs Omicron infection. /10
In the #ON study between 7-59 days post 2nd dose, only 36% protection was achieved vs Omicron infection. /10
However, protection against Omicron infection increases SUBSTANTIALLY after a 3rd dose of vaccine.
In the #ON study, protection against Omicron infection increased to 61% >=7 days following a 3rd dose.
THIS is why getting your 3rd dose if eligible is SO critical w/ Omicron. /11
In the #ON study, protection against Omicron infection increased to 61% >=7 days following a 3rd dose.
THIS is why getting your 3rd dose if eligible is SO critical w/ Omicron. /11
Omicron is super contagious. We all know this.
If you don't have 3 doses of vaccine your protection vs Omicron infection is very low. THIS is why we need to be encouraging 3rd doses for as many persons as we can.
Only ~1/3rd of #SK residents have 3+ doses. That's too low. /12
If you don't have 3 doses of vaccine your protection vs Omicron infection is very low. THIS is why we need to be encouraging 3rd doses for as many persons as we can.
Only ~1/3rd of #SK residents have 3+ doses. That's too low. /12
What proportion of people w/ 2 doses in Saskatchewan had a 2nd dose in July or August of last year? Probably a big number.
Those people likely think they're protected because they're "fully vaccinated", but that protection against Omicron infection is actually VERY LOW now. /13
Those people likely think they're protected because they're "fully vaccinated", but that protection against Omicron infection is actually VERY LOW now. /13
Note the case rate per 100,000 in persons w/ 3+ doses in #SK is only 80 per 100,000.
Compared to the 2+ dose rate (140 per 100,000), this fits with our expectations: 3 doses is pretty good vs. Omicron infection, but NOT perfect. /14
Compared to the 2+ dose rate (140 per 100,000), this fits with our expectations: 3 doses is pretty good vs. Omicron infection, but NOT perfect. /14
Why are 1 dose case rates per capita also low at only 70 per 100,000?
It's likely an artifact as a result of statistical variation.
Only ~5.7% of the entire #SK population falls into this category, and testing availability is all over the place, so hard to interpret. /15
It's likely an artifact as a result of statistical variation.
Only ~5.7% of the entire #SK population falls into this category, and testing availability is all over the place, so hard to interpret. /15
So that brings us to the last issue: PCR testing in Saskatchewan.
Availability of PCR testing has been problematic. Many persons are self-diagnosing with rapid tests.
Current guidelines in #SK suggest if you test positive on RAT, to self-isolate & generally NOT to seek PCR. /16
Availability of PCR testing has been problematic. Many persons are self-diagnosing with rapid tests.
Current guidelines in #SK suggest if you test positive on RAT, to self-isolate & generally NOT to seek PCR. /16
Case numbers depend on people GOING to get tested. PCR testing is being increasingly limited to high-risk settings, health care workers, etc.
Most persons are not bothering any longer to get PCR testing done - it's a pain. So we don't REALLY know what true case numbers are. /17
Most persons are not bothering any longer to get PCR testing done - it's a pain. So we don't REALLY know what true case numbers are. /17
Lastly, I don't have any data to support this, but it stands to reason that persons who are not vaccinated are LESS LIKELY to access PCR testing (or rapid testing) compared to persons with 2/3/4 doses.
I'm just inferring this based on personal experience and common sense. /18
I'm just inferring this based on personal experience and common sense. /18
If that's actually the case, then the number of cases being diagnosed via PCR and ending up in the "official" provincial case count is likely much lower for unvaccinated persons compared to other vaccinated groups.
You can't count cases if people aren't getting tested. /19
You can't count cases if people aren't getting tested. /19
My bottom line is case data right now in Saskatchewan is messy and largely uninterpretable for the reasons above.
It's the old statistical adage: garbage in, garbage out.
If the data you're putting in is crap, then conclusions you try to draw from that data are also crap. /20
It's the old statistical adage: garbage in, garbage out.
If the data you're putting in is crap, then conclusions you try to draw from that data are also crap. /20
There may be other factors at play that I haven't explained or thought of. But regardless, the data we have around cases in Saskatchewan IS CRAP.
If we care about basing policy decisions on high quality scientific evidence, case data shouldn't be used in any way. /21
If we care about basing policy decisions on high quality scientific evidence, case data shouldn't be used in any way. /21
All of this stuff is SUPER complicated.
The Premier has access to squadrons of statistical & public health experts within the Ministry of Health.
I am CERTAIN that if they had been consulted, they would have been able to provide him with the insights in this thread. /22
The Premier has access to squadrons of statistical & public health experts within the Ministry of Health.
I am CERTAIN that if they had been consulted, they would have been able to provide him with the insights in this thread. /22
To conclude, I'll be blunt.
NONE of the decisions around #COVID19 policy in Saskatchewan are being driven any longer by science or evidence, or a desire to minimize death or suffering from COVID infection.
To pretend they are, openly insults the majority of the electorate. /23
NONE of the decisions around #COVID19 policy in Saskatchewan are being driven any longer by science or evidence, or a desire to minimize death or suffering from COVID infection.
To pretend they are, openly insults the majority of the electorate. /23
Elected officials with no qualifications shouldn't pretend to be epidemiologists any more than I should pretend to know how to fix my car or play politics.
It's both dangerous & irresponsible when someone doesn't know limits.
IMO, smart people ask for AND accept help. /24
It's both dangerous & irresponsible when someone doesn't know limits.
IMO, smart people ask for AND accept help. /24
To conclude:
- It's NOT as simple as 'base rate fallacy', but yes, Saskatchewan's case data is crap.
- Trying to justify policy using crap data is dumb at best, reckless at worst.
#SK hospitals/ICUs are in all kinds of trouble. No help is coming.
We're on our own, #SK. /end.
- It's NOT as simple as 'base rate fallacy', but yes, Saskatchewan's case data is crap.
- Trying to justify policy using crap data is dumb at best, reckless at worst.
#SK hospitals/ICUs are in all kinds of trouble. No help is coming.
We're on our own, #SK. /end.
• • •
Missing some Tweet in this thread? You can try to
force a refresh