1/10 As someone who struggles with test-taking, I made a framework for tackling some common test-taking hurdles. I had the opportunity to go over this with all our @uclaimchiefs housestaff and decided to make it into a 🧵 #MedTwitter #MedStudentTwitter #FOAMed
2/ Test scores are important because they are what you need to become board-certified. Scores are often conflated with competency - that is quite a fallacy as so many other factors go into competency.
3/ Here is a non-comprehensive set of examples of test-taking hurdles. Let’s go through each of them systematically in a way that resonates with internists - problem listing! FYI, all of these end of overlapping a lot 

4/ First we have impaired ⏲️ management. Opening up lab references will split your screen, so you don’t have to read the questions all the way across the monitor (this can help ⬇️ fatigue).

5/ Next up is getting stuck between choices. Finding a trusted individual is really important for your growth in this domain.

6/ Next is ⬇️ stamina. Steadily lengthening the block of practice questions can help.

7/ Finally we have ⬇️ focus, which overlaps greatly with ⬇️ stamina

8/ To mitigate these issues, create lots of SMART goal that are context-dependent (the rigors of your ICU rotations are different than those of your clinic rotations). Consider creating 🗓️ events to schedule time to study/take questions.

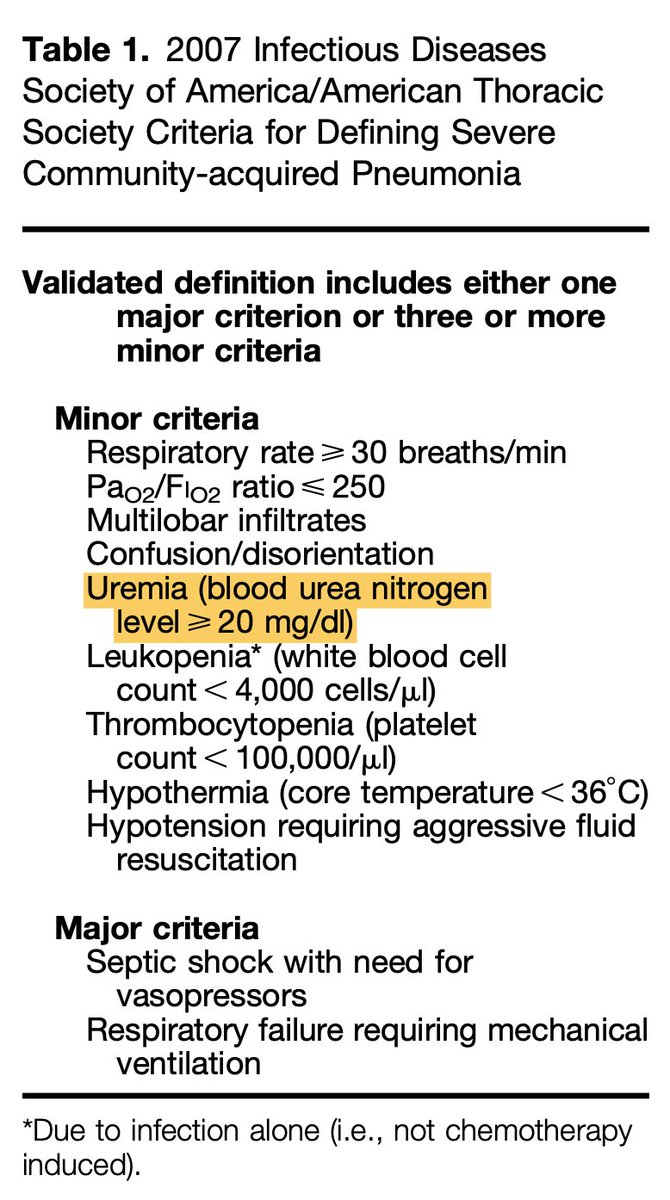
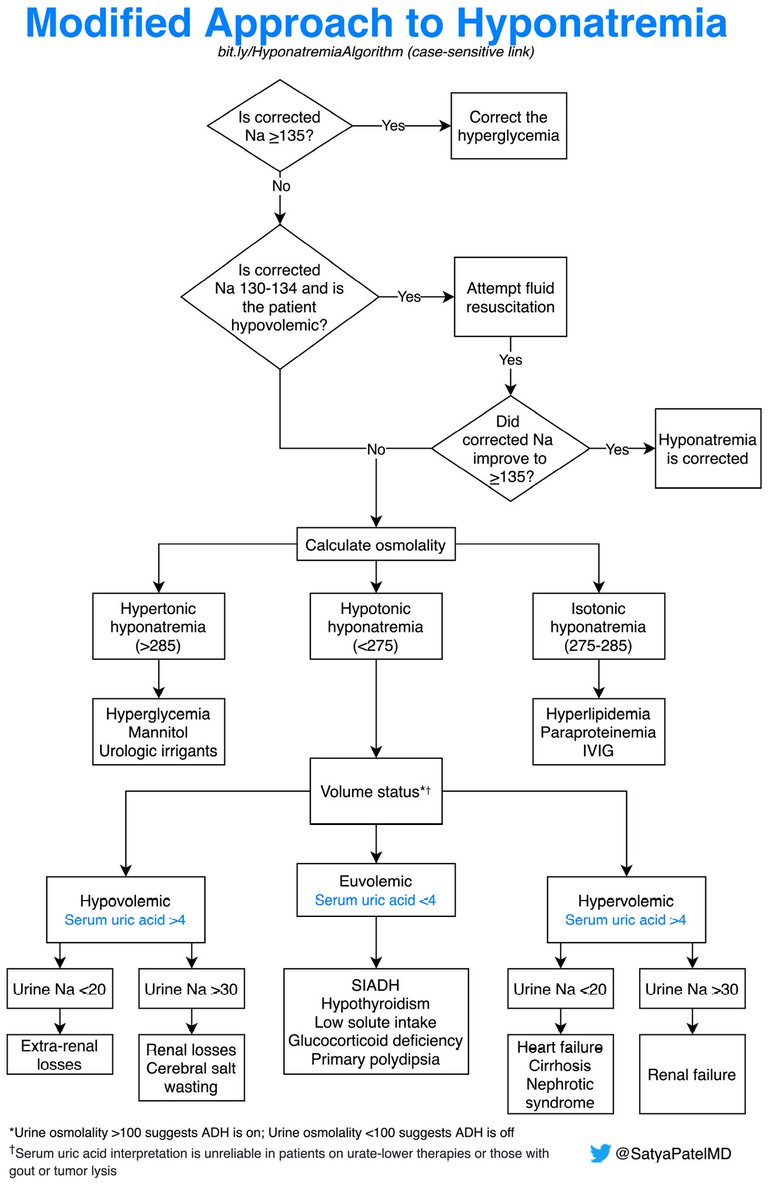
9/ Finally, it is worth keeping a log of reflections and learning points as your own reference to peruse at your leisure. Here is an example of my log from when I was studying for my boards.

10/10
In summary
✴️Invest time in diagnosing your test-taking issues
✴️Develop a #growthmindset when doing practice questions
✴️Keep a log of questions that helps inform and identify your test-taking issues
Would love to hear what others have to say!
In summary
✴️Invest time in diagnosing your test-taking issues
✴️Develop a #growthmindset when doing practice questions
✴️Keep a log of questions that helps inform and identify your test-taking issues
Would love to hear what others have to say!
And a big thank you to @rachelpbrookmd for allowing me to be involved in helping residents navigate these issues!
• • •
Missing some Tweet in this thread? You can try to
force a refresh