😳🤯The hour flew by & none of us noticed!!
🙏🏽 @FogacciJoao for bringing the 🇧🇷 flair to #TumorBoardTuesday & #GastricCancer!!
🏆Remember your🆓CME
Look for Case Wrap Up🎀 04/28/22
📅Mark your calendar for 05/10/22 8pm ET when @FlavioRochaMD joins our #VirtualTumorBoard!!
🙏🏽 @FogacciJoao for bringing the 🇧🇷 flair to #TumorBoardTuesday & #GastricCancer!!
🏆Remember your🆓CME
Look for Case Wrap Up🎀 04/28/22
📅Mark your calendar for 05/10/22 8pm ET when @FlavioRochaMD joins our #VirtualTumorBoard!!
Remember #TumorBoardTuesday education goes beyond Twitter - we offer 🆓 CME!!
Pick up your🏆#CME & NOW #MOC(‼️) by answering quick questions regarding a case similar to @FogacciJoao’s‼️
🔗ALL CME: integrityce.com/tbt
🔗 post rationale: bit.ly/3kcIXdv
🇧🇷🎁🇧🇷
Pick up your🏆#CME & NOW #MOC(‼️) by answering quick questions regarding a case similar to @FogacciJoao’s‼️
🔗ALL CME: integrityce.com/tbt
🔗 post rationale: bit.ly/3kcIXdv
🇧🇷🎁🇧🇷
#PostTest Q1️⃣ #CME #TumorBoardTuesday @MPishvaian
🤔Now that @FogacciJoao schooled us through updates on immunotherapy for #GastricCancer, how would you answer these 2 quick ❓
🧬 Which are potentially useful immunotherapy biomarkers in gastric cancer?
🤔Now that @FogacciJoao schooled us through updates on immunotherapy for #GastricCancer, how would you answer these 2 quick ❓
🧬 Which are potentially useful immunotherapy biomarkers in gastric cancer?
Q2️⃣ #CME #TumorBoardTuesday #OncTwitter @FogacciJoao @MPishvaian
🔗Free CME & MOC: integrityce.com/tbt
🔗 Posttest rationale: bit.ly/3kcIXdv
🧐 What’s *special* about MUTYH mt biallelic tumors? 🧬
🔗Free CME & MOC: integrityce.com/tbt
🔗 Posttest rationale: bit.ly/3kcIXdv
🧐 What’s *special* about MUTYH mt biallelic tumors? 🧬
1/11 #TumorBoardTuesday
🧬Time for this week's Thursday Case🎀
We discussed germline MUTYH and immunotherapy in #Gastriccancer.
👉Get your 🆓#CME (AMA & NOW #MOC(‼️)) credit by answering 2 quick❓
ALL CME eval🔗: integrityce.com/tbteval
CME rationale🔗: bit.ly/3kcIXdv
🧬Time for this week's Thursday Case🎀
We discussed germline MUTYH and immunotherapy in #Gastriccancer.
👉Get your 🆓#CME (AMA & NOW #MOC(‼️)) credit by answering 2 quick❓
ALL CME eval🔗: integrityce.com/tbteval
CME rationale🔗: bit.ly/3kcIXdv
2/11 #TumorBoardTuesday
Thurs Case🎀
Take🏠msgs:
We discussed #Gastric #GEA and when/how to deploy IO:
✅gMUTYH mut are rare–but associate w/ IO efficacy!
✅MUTYH= base excision repair defect-> point mut, including KRAS G12C. Ongoing re: use of🎯targeted 💊+IO, but not yet SOC
Thurs Case🎀
Take🏠msgs:
We discussed #Gastric #GEA and when/how to deploy IO:
✅gMUTYH mut are rare–but associate w/ IO efficacy!
✅MUTYH= base excision repair defect-> point mut, including KRAS G12C. Ongoing re: use of🎯targeted 💊+IO, but not yet SOC
2.5/11
#TumorBoardTuesday
Thurs Case🎀
Take🏠msgs- cont’d:
✅Checkpoint inhib provide benefit in gastric CA, but controversy over PD-L1 cut-off
✅PD-L1 assessment is hard; tumor often w high variability
📚We captured as much as we could in this moment:
twitter.com/i/events/15138…
#TumorBoardTuesday
Thurs Case🎀
Take🏠msgs- cont’d:
✅Checkpoint inhib provide benefit in gastric CA, but controversy over PD-L1 cut-off
✅PD-L1 assessment is hard; tumor often w high variability
📚We captured as much as we could in this moment:
twitter.com/i/events/15138…
3/11 #TumorBoardTuesday
Thurs Case🎀
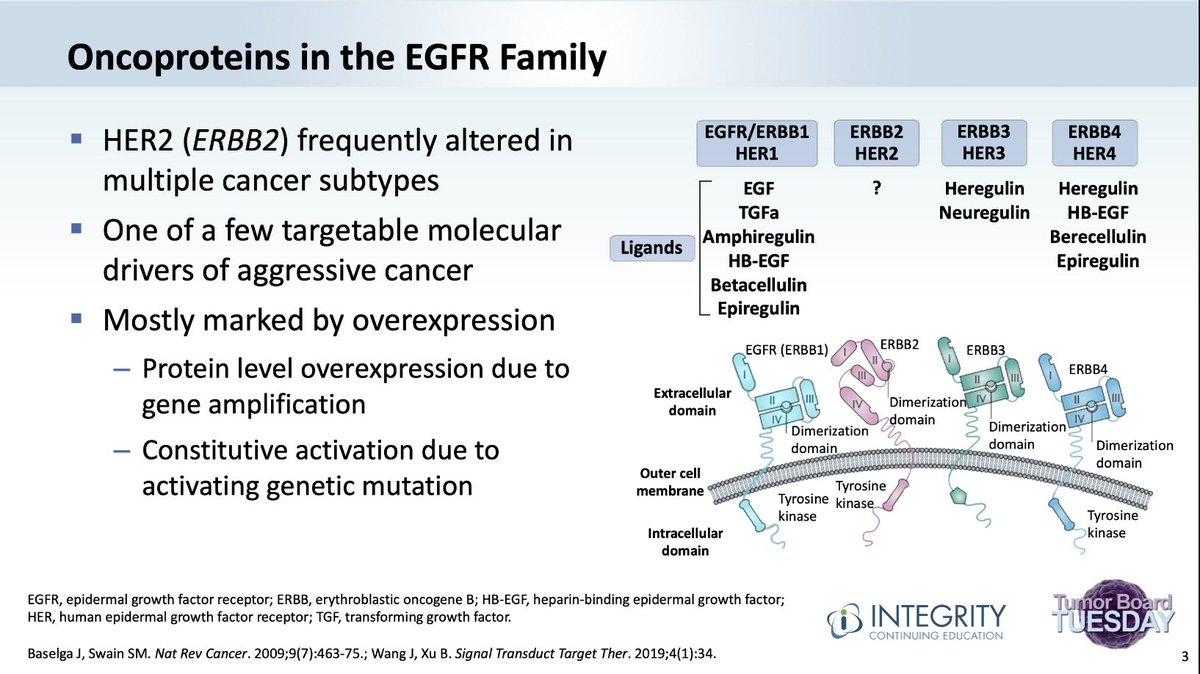
@FoggaciJoao presents case of 22 yo👩, who already had cancer twice (🫁 & CRC), now w new gastric adeno w peritoneal nodule. pMMR; HER2-; no tissue for PD-L1 eval
➡️What chemo? Can we incorporate IO? Here’s what the crowd thought:
Thurs Case🎀
@FoggaciJoao presents case of 22 yo👩, who already had cancer twice (🫁 & CRC), now w new gastric adeno w peritoneal nodule. pMMR; HER2-; no tissue for PD-L1 eval
➡️What chemo? Can we incorporate IO? Here’s what the crowd thought:

4/11 #TumorBoardTuesday
Thurs Case🎀
Good discussion re: role of PD-L1 biomarker in #GastricCancer.
👉CM-649 =benefit, 🚫stratify by PD-L1
@rcavalhoonco points out meta analysis by Zhao et al: 👍IO only when CPS>=5. But, ORIENT-16 shows 👍in Asia even CPS<5.
NCCN= 5 as cut-off
Thurs Case🎀
Good discussion re: role of PD-L1 biomarker in #GastricCancer.
👉CM-649 =benefit, 🚫stratify by PD-L1
@rcavalhoonco points out meta analysis by Zhao et al: 👍IO only when CPS>=5. But, ORIENT-16 shows 👍in Asia even CPS<5.
NCCN= 5 as cut-off
5/11 #TumorBoardTuesday
Thursday Case🎀
🕵️Which led us to a closer look at how we use PD-L1 IHC and eval CPS.
🔬Turns out PD-L1 is heterogenously expressed in tumor/stroma–and depending on where tumor is sampled, can get very different results!
nature.com/articles/s4141…
Thursday Case🎀
🕵️Which led us to a closer look at how we use PD-L1 IHC and eval CPS.
🔬Turns out PD-L1 is heterogenously expressed in tumor/stroma–and depending on where tumor is sampled, can get very different results!
nature.com/articles/s4141…

6/11 #TumorBoardTuesday
Thursday Case🎀
Back to the case
🙅♀️Pt says no to chemotherapy; has already been through so much.
🤔What to do now❓❓❓
💡✅ It’s TBT, so we think NGS is (almost always) a great idea
Thursday Case🎀
Back to the case
🙅♀️Pt says no to chemotherapy; has already been through so much.
🤔What to do now❓❓❓
💡✅ It’s TBT, so we think NGS is (almost always) a great idea
7/11 #TumorBoardTuesday
Thursday Case🎀
Tumor NGS shows:
⏫ High TMB (89!)
🧬 MUTYH c536A > G (present in germline!)
🧬 BLM c3427G > A heterozygous, VUS
🤔Is there a chemo free option here?
Thursday Case🎀
Tumor NGS shows:
⏫ High TMB (89!)
🧬 MUTYH c536A > G (present in germline!)
🧬 BLM c3427G > A heterozygous, VUS
🤔Is there a chemo free option here?
8/11 #TumorBoardTuesday
Thursday Case🎀
🗝Maybe– KEYNOTE-062= pembro monotx non-inferior to chemo in pts w advanced #GastricCancer w PD-L1 CPS >1. CPS>10 trended📈toward best outcomes, as did pts w MSI-H disease.
🔹Caveat: most of study pop w CPS>10.
jamanetwork.com/journals/jamao…
Thursday Case🎀
🗝Maybe– KEYNOTE-062= pembro monotx non-inferior to chemo in pts w advanced #GastricCancer w PD-L1 CPS >1. CPS>10 trended📈toward best outcomes, as did pts w MSI-H disease.
🔹Caveat: most of study pop w CPS>10.
jamanetwork.com/journals/jamao…

9/11 #TumorBoardTuesday
Thursday Case🎀
👨🏫 Which led to @FogacciJoao’s tweetorials focused on IO as well as how certain mutations, such as 🧬gMUTYH can create the right environment for IO to work.
Thursday Case🎀
👨🏫 Which led to @FogacciJoao’s tweetorials focused on IO as well as how certain mutations, such as 🧬gMUTYH can create the right environment for IO to work.
https://twitter.com/FogacciJoao/status/1519113135973670913
10/11 #TumorBoardTuesday
Thursday Case🎀 #GastricCancer
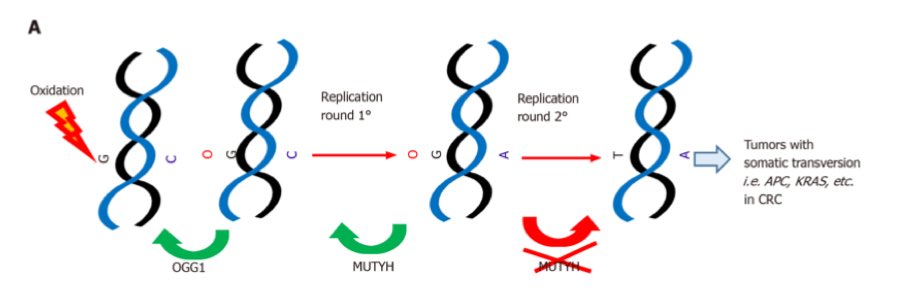
✅MUTYH is a glycosylase that plays a 🗝key role in base excision repair (BER)
✅Tendency toward G:C-> T:A substitutions
✅@ShimaghavimiMD points out that up to 25% of MUTYH mut in #CRC assoc w KRAS G12C mutation!
Thursday Case🎀 #GastricCancer
✅MUTYH is a glycosylase that plays a 🗝key role in base excision repair (BER)
✅Tendency toward G:C-> T:A substitutions
✅@ShimaghavimiMD points out that up to 25% of MUTYH mut in #CRC assoc w KRAS G12C mutation!
11/11 #TumorBoardTuesday
Thurs Case🎀
🙏Pt on pembrolizumab monotx- ongoing stable disease 1 year later!
🤔KRAS G12C might be 🎯 here as well–studies now in🫁ca combining💊+ IO
➡️Join us 05/10/22 at 8pm ET when @FlavioRochaMD presents a case of locally advanced #ColonCancer😀
Thurs Case🎀
🙏Pt on pembrolizumab monotx- ongoing stable disease 1 year later!
🤔KRAS G12C might be 🎯 here as well–studies now in🫁ca combining💊+ IO
➡️Join us 05/10/22 at 8pm ET when @FlavioRochaMD presents a case of locally advanced #ColonCancer😀
@rcarvalhoonco @GIcancerDoc @AJacomeMD @RachelRiechelm2 @KellyBorgesAra2 @giammi107 @RonaYeager @ShimaghavimiMD @fernandbteich @D_B_McConnell @indepso @JamesClearyMD @Alinechaves73 @SunnieSKim @VinciusLorandi1 @CrozrX @Ariltojr @DrR_DUNNE @cissamathias @YLeyfman @W_Park_MD
@DFernandes_MD @Juanma19712012 @nesliHanozDe @asaf_maoz @BenWestphalen @DocLHenry @cofiadeva @StoCANcer @jacobadashek @RyanCMassa @IglesiaMichael @JDekervel @jaypsv @YJanjigianMD @LizzySmyth1 @RenataDAlpino @pashtoonkasi @GillSharlene @oleandromoreno @viniciu_antonio @BiachiTiago
@gabe_a_brooks @drmarcusgomes @GrupoGTG @SBOC_Oncologia @OncBrothers @CathyEngMD @graokane @dralanburguete @TakedaFlavio @duiliorocha_onc @PestanaRC @fireflyann @manjuggm @realbowtiedoc @jebezerraneto @marklewismd @ShaalanBeg @drymtn @dePaulaBHR @JCrespoMD @FlavioRochaMD
Remember #TumorBoardTuesday continues to offer AMA & now MOC credit for FREE! Don’t forget to answer the polls👇🏽
Then click this link to quickly request your credit!
ALL CME eval🔗: integrityce.com/tbt
CME rationale🔗: bit.ly/3kcIXdv
Then click this link to quickly request your credit!
ALL CME eval🔗: integrityce.com/tbt
CME rationale🔗: bit.ly/3kcIXdv
https://twitter.com/tumorboardtues/status/1519125665601179648?s=21&t=oVw70uiIibI57iF3MaI9GQ
• • •
Missing some Tweet in this thread? You can try to
force a refresh