NEXT Adaptive and Platform trial designs by @Lennie333 #datascience #ai #ml #icudata
#LIVES2022 #ventilation
@ESICM
we assume "large effect sizes" in ICU trials
#LIVES2022 #ventilation
@ESICM
we assume "large effect sizes" in ICU trials
@Lennie333 @ESICM this is because otherwise we will need large "n" and long time for trials.
e.g., anti-hypertensives - you dont want to test one drug at one dose. you want to test a range of doses and a range of duration.
third-thing : we struggle to find a end-point especially in critical care
e.g., anti-hypertensives - you dont want to test one drug at one dose. you want to test a range of doses and a range of duration.
third-thing : we struggle to find a end-point especially in critical care
@Lennie333 @ESICM huge effort doing RCT but we use "mortality" yes/no as a very binary endpoint. For patient, length of stay, quality of life after d/c important end points beyond survival.
in RCT, we cant learn whilst the trials are still running. in classic RCT.
in RCT, we cant learn whilst the trials are still running. in classic RCT.
A bit like going on holiday in 90. You look at map and you set destination. Close your eyes and open when ya reach there. No change midway through etc 

what can we do ?
- make a really big trouble "more pts" e.g., ANZAC's Rox trial
- do Metaanalysis
- or harmonize trials
- or core outcome sets (so trials are comparable)
- or smarter statistics
OR
PLATFORM TRIAL . It is not a "scary thing" newer form of RCT. #adaptivetrials
- make a really big trouble "more pts" e.g., ANZAC's Rox trial
- do Metaanalysis
- or harmonize trials
- or core outcome sets (so trials are comparable)
- or smarter statistics
OR
PLATFORM TRIAL . It is not a "scary thing" newer form of RCT. #adaptivetrials
In RCT adapative platform format, you need "master protocols" and "adaptive trials"
pubmed.ncbi.nlm.nih.gov/28679092/
pubmed.ncbi.nlm.nih.gov/28679092/
Here if ya compare these in a traditional format it will take a long time and cost.

What we are interested is not a treatment A vs. treatment B. That is useful but an inferior question to "what is the optimal treatment" for this patient?
so you need "patient", "domain", "intervention", "regimen".
Domain is effectively "area of treatment".
so you need "patient", "domain", "intervention", "regimen".
Domain is effectively "area of treatment".
This especially work in ICU -- it is a "syndrome based" job.
by having a "broad inclusion criteria" , you can stratify in many ways.
pubmed.ncbi.nlm.nih.gov/33206201/
by having a "broad inclusion criteria" , you can stratify in many ways.
pubmed.ncbi.nlm.nih.gov/33206201/
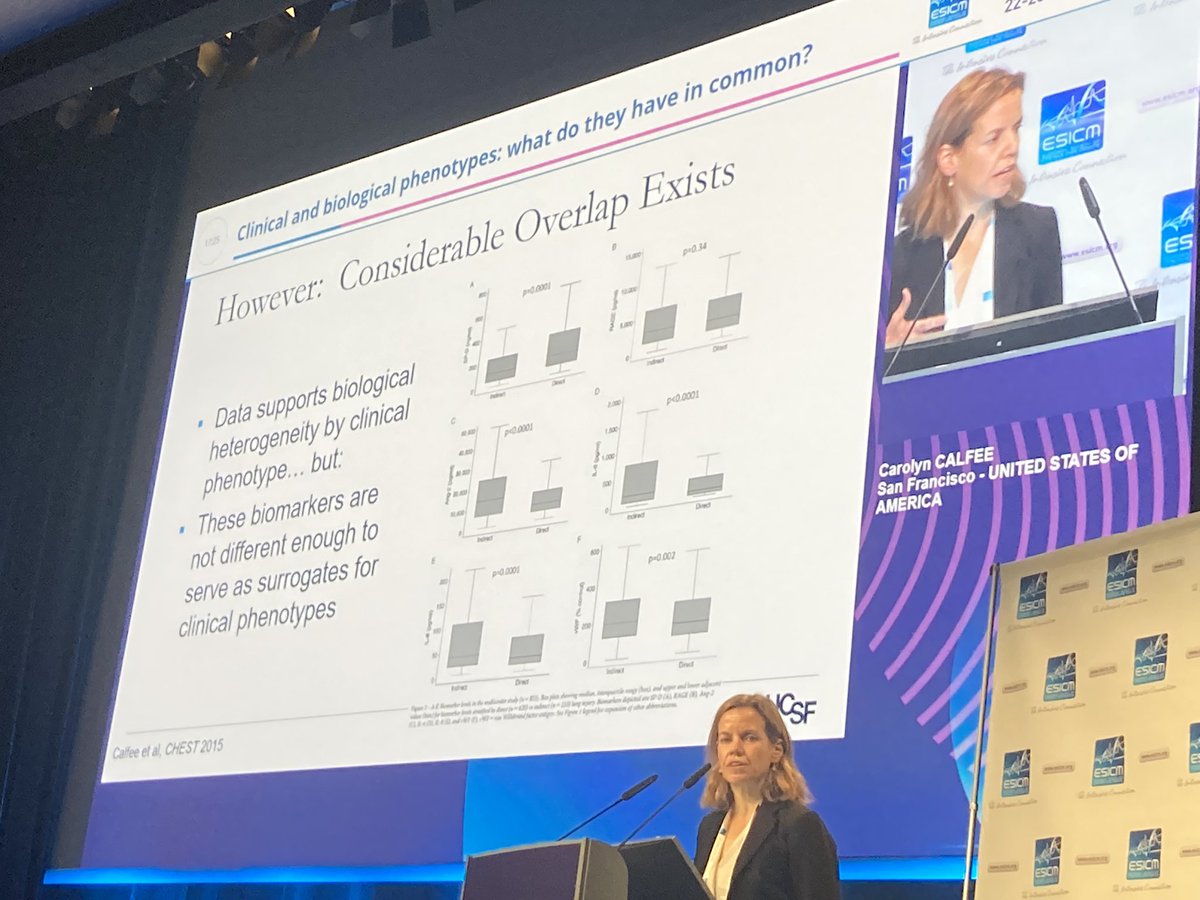
Despite the heterogeneity, you can also quantify the heat maps of these patients and you can stratify bsed on this.
nature.com/articles/s4159…
nature.com/articles/s4159…
So far we talked about "platform" part of adaptive platform trials.
What about "adaptive" bit?
What about "adaptive" bit?
In adaptive trials we move in circles. Not in linear lines. If you meet criteria you exit or re circulate

If the probability of treatment 2 is superior than 1, you dont stop a trial, you re-assign next recruits in comparison so it evaluates against 2. if it is inferior, you can stop that particular domain for randomisation. see next image for graphical representation



Of course one need to talk about "Bayesian " approach . see graphics above.
Essentially it updates based on posterior probability.
This sounds fancy but we do it everyday when we cross the road.
Essentially it updates based on posterior probability.
This sounds fancy but we do it everyday when we cross the road.
-- So adaptive platform trials are great BUT
- adaptive platform cost a lot of time to set up for making sure model behaves well
- adaptive platform trial need simulation to test out the model
Long setup time, high start up cost, pre-trial simulations, practical hurdles,
- adaptive platform cost a lot of time to set up for making sure model behaves well
- adaptive platform trial need simulation to test out the model
Long setup time, high start up cost, pre-trial simulations, practical hurdles,
and all of this means NEED MORE FUNDING which is usually for 5-year slot. Adaptive platform trials help address heterogeneity o treatment effects ,lose ineffective therapies
@ESICM #datascience #ai #ml #icudata
#adaptiveplatformtrial
@ESICM #datascience #ai #ml #icudata
#adaptiveplatformtrial
• • •
Missing some Tweet in this thread? You can try to
force a refresh