A #tweetorial on Perioperative risk assessment for Non-cardiac surgeries for #FITsurvivalguide
⚠️NOT "clearance"!
Purpose of consult
-Evaluate pt`s medical status
-Risk assessment
-Management recs
-Treat modifiable risk factors
-"Team" approach for shared decision making
⚠️NOT "clearance"!
Purpose of consult
-Evaluate pt`s medical status
-Risk assessment
-Management recs
-Treat modifiable risk factors
-"Team" approach for shared decision making
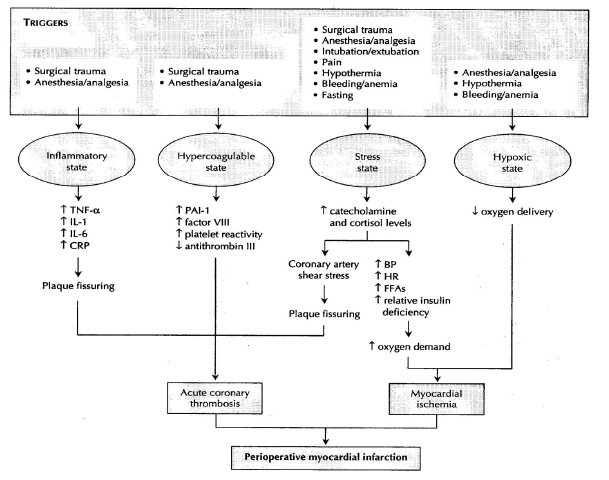
2/ Triggers for perioperative myocardial injury
-Inflammatory state
-Hypercoagulable state
-Stress state
-Hypoxic state
All predispose to ischemia and coronary thrombosis.
-Inflammatory state
-Hypercoagulable state
-Stress state
-Hypoxic state
All predispose to ischemia and coronary thrombosis.
3/ Think about- 🤔
-Should pt have surgery? Emergent or not?
-Type of surgery and type of anesthesia?
-Functional status of the pt?
-Relevant medical hx and any ongoing cardiac sx?
-Review the meds.
-Prior cardiac w/u.
Focus on good history and PE, can save a lot of tests & 💸
-Should pt have surgery? Emergent or not?
-Type of surgery and type of anesthesia?
-Functional status of the pt?
-Relevant medical hx and any ongoing cardiac sx?
-Review the meds.
-Prior cardiac w/u.
Focus on good history and PE, can save a lot of tests & 💸
4/ ACC/AHA and @escardio guidelines for perioperative risk 2014.
Very thorough and informative 📃.
Assess pt`s clinical risk
💠ACC 2009- Low, medium or high risk.
💠ACC 2014 update- Low risk ( <1% risk of MACE) or elevated risk (>1% MACE)
Very thorough and informative 📃.
Assess pt`s clinical risk
💠ACC 2009- Low, medium or high risk.
💠ACC 2014 update- Low risk ( <1% risk of MACE) or elevated risk (>1% MACE)
5/ Assessing Functional Capacity (pic below)
💠1MeT- Resting or basal oxygen consumption of a 40–year-old, 70-kg man.
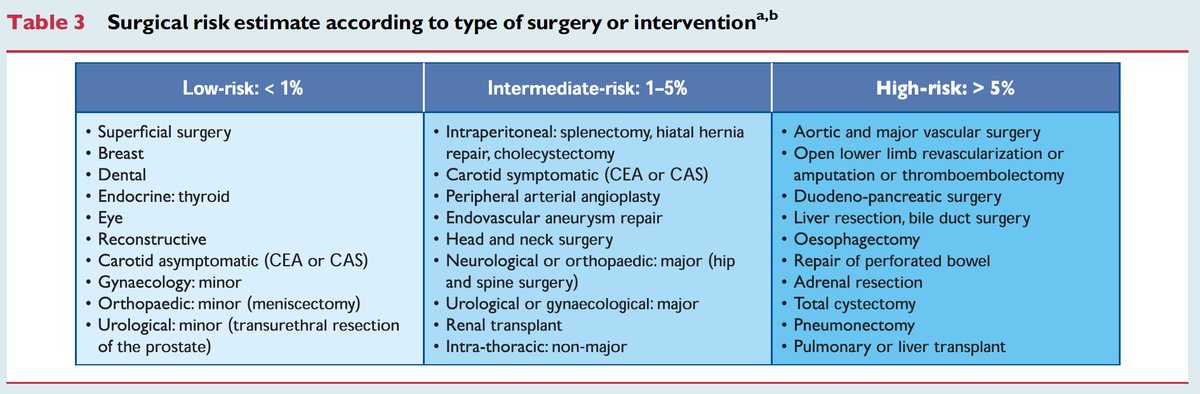
Risk of surgery (pic below)
Low, Intermediate and High risk.
⚠️In RCRI, high risk includes suprainguinal vascular, intra-thoracic and –abdominal.
💠1MeT- Resting or basal oxygen consumption of a 40–year-old, 70-kg man.
Risk of surgery (pic below)
Low, Intermediate and High risk.
⚠️In RCRI, high risk includes suprainguinal vascular, intra-thoracic and –abdominal.

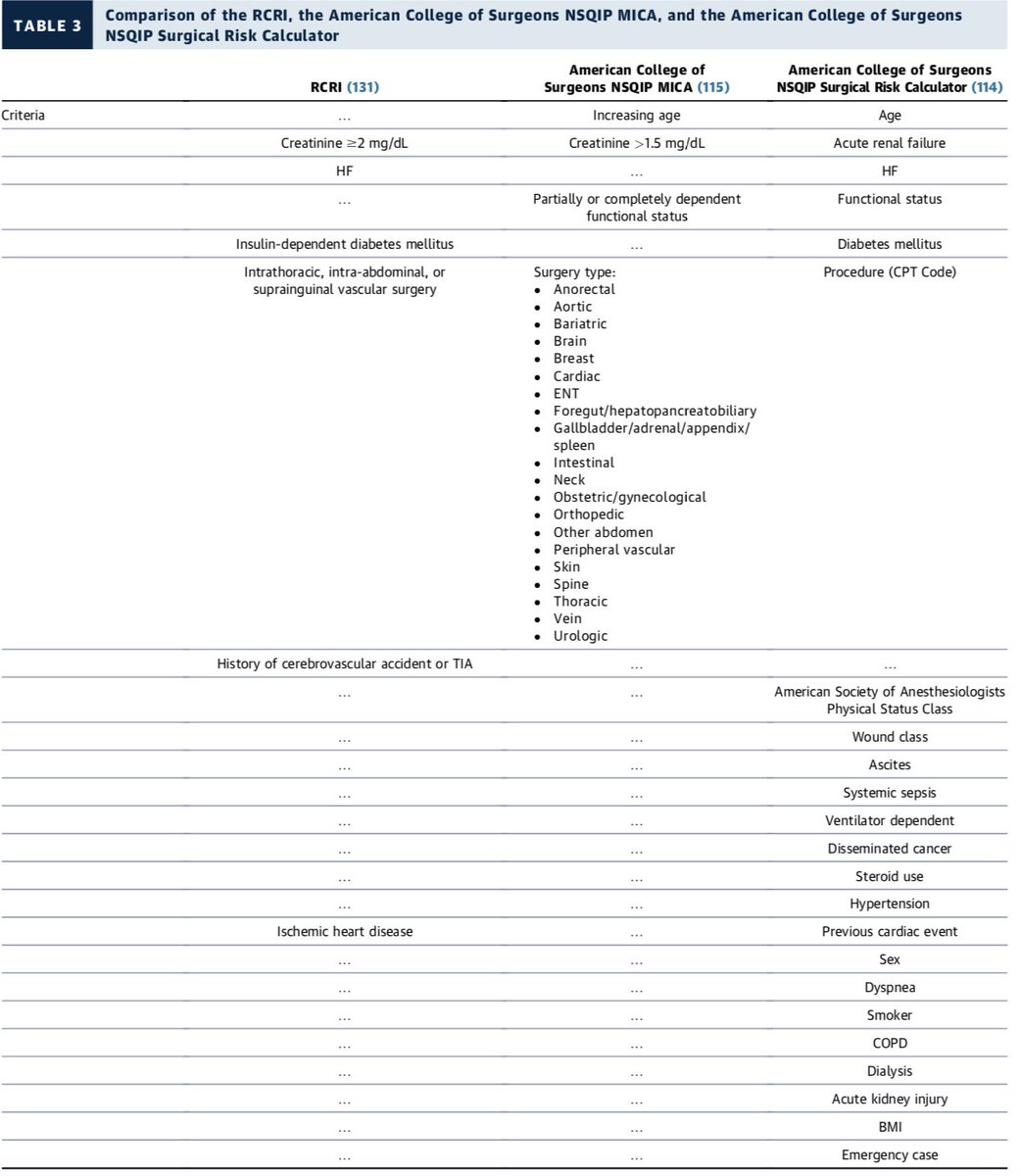
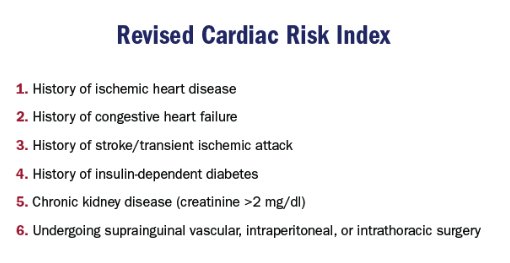
6/ Risk prediction models
💠Revised Cardiac Risk Index (RCRI)-simple, widely accepted
• 0-1 low risk, >1 elevated risk
💠ACS NSQIP MICA
• (surgicalriskcalculator.com/miorcardiacarr…)
💠ACS NSQIP Surgical Risk Calculator
• (riskcalculator.facs.org)
💠Revised Cardiac Risk Index (RCRI)-simple, widely accepted
• 0-1 low risk, >1 elevated risk
💠ACS NSQIP MICA
• (surgicalriskcalculator.com/miorcardiacarr…)
💠ACS NSQIP Surgical Risk Calculator
• (riskcalculator.facs.org)
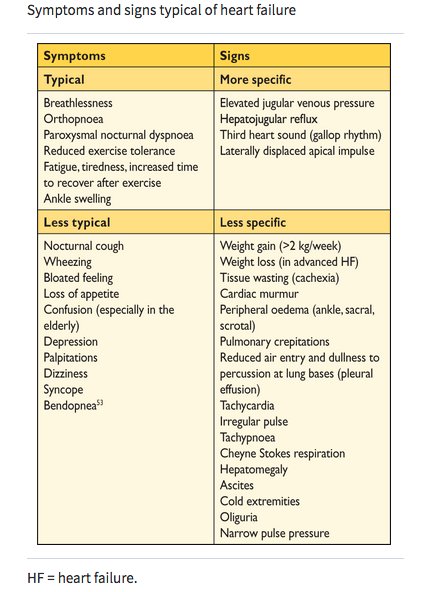
7/ ❌ ignore the “high risk” conditions
⚠️Recent (<30 days) or active MI, unstable or severe.
⚠️Acute decompensated HF
⚠️Severe symptomatic valvular disease
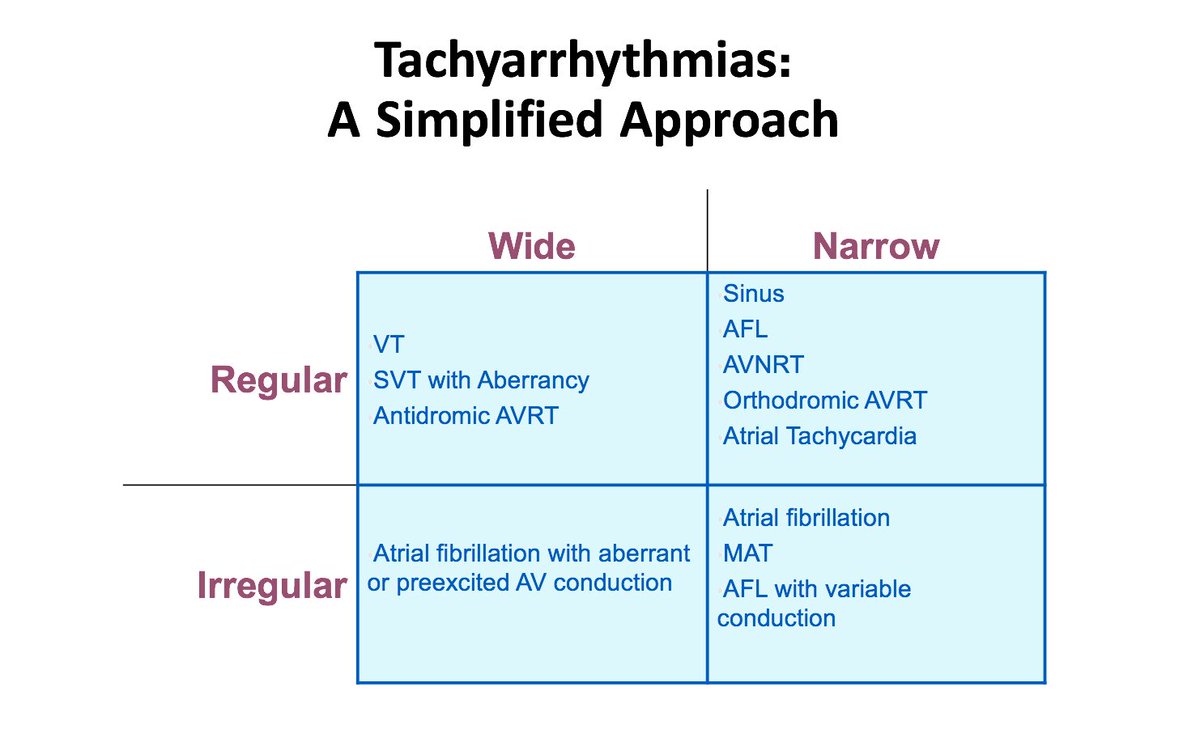
⚠️Significant arrhythmias (tachy/brady)
Consider delaying non-emergent surgery if present.
⚠️Recent (<30 days) or active MI, unstable or severe.
⚠️Acute decompensated HF
⚠️Severe symptomatic valvular disease
⚠️Significant arrhythmias (tachy/brady)
Consider delaying non-emergent surgery if present.
8/ Supplemental Preop testing
Remember the important DONTs
❌ECG for asymptomatic pt; low risk surgery
❌Routine eval of LV function
❌Stress test for low risk surgery
❌Routine cors angiography
Remember the important DONTs
❌ECG for asymptomatic pt; low risk surgery
❌Routine eval of LV function
❌Stress test for low risk surgery
❌Routine cors angiography

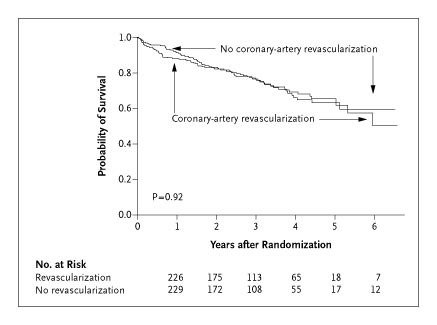
9/ Preoperative revascularization
☑️Prophylactic revascularization no significant ⬇️ MACE (CARP trial below).
Who needs cath? 🤔
-Same indication if you are evaluating for non preop.
-Unstable/sx on 💊
-Stable w/ ⬆️ probability mv-CAD+/-LV dysfnctn for ⬆️risk surgery
☑️Prophylactic revascularization no significant ⬇️ MACE (CARP trial below).
Who needs cath? 🤔
-Same indication if you are evaluating for non preop.
-Unstable/sx on 💊
-Stable w/ ⬆️ probability mv-CAD+/-LV dysfnctn for ⬆️risk surgery
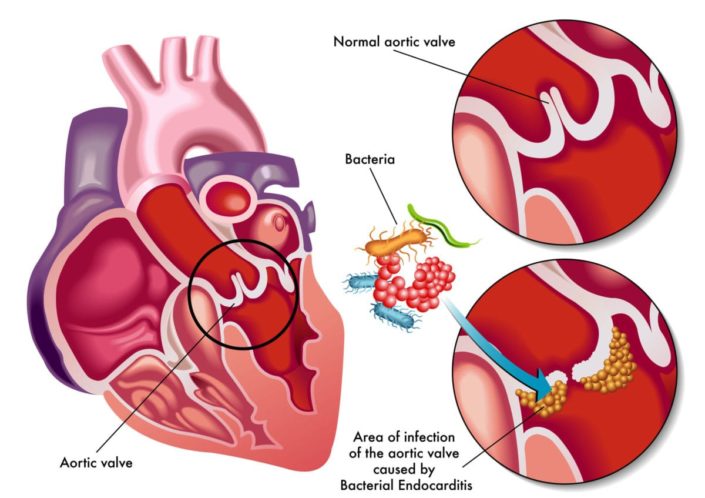
10/ Severe VHD
Symptomatic- Rx before elective surgery
💠Symptomatic AS -⬆️ periop mortality ~10%; Rx prior to surgery
💠Severe, asymptomatic AS-acceptable risk(avoid low preload)
💠Severe MV stenosis- avoid ⬆️HR
💠AR/MR-usually well tolerated
Symptomatic- Rx before elective surgery
💠Symptomatic AS -⬆️ periop mortality ~10%; Rx prior to surgery
💠Severe, asymptomatic AS-acceptable risk(avoid low preload)
💠Severe MV stenosis- avoid ⬆️HR
💠AR/MR-usually well tolerated
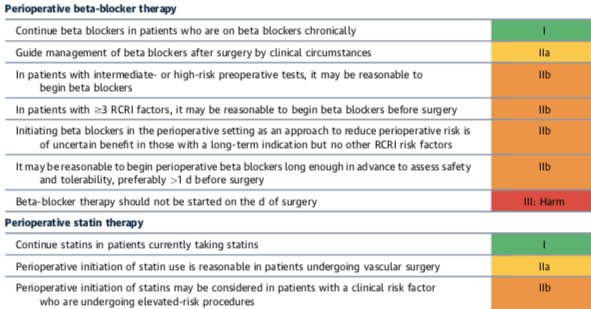
11/ Perioperative beta-blockers (debatable topic)
☑️Continue home dose of BB.
❌Don’t start on the day of surgery.
Statins
☑️Continue if already on.
☑️Consider starting prior to vascular surgery
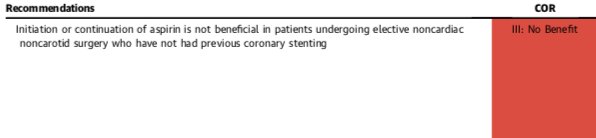
ASA-If prior PCI, continue ASA. Otherwise, no benefit over the placebo.
☑️Continue home dose of BB.
❌Don’t start on the day of surgery.
Statins
☑️Continue if already on.
☑️Consider starting prior to vascular surgery
ASA-If prior PCI, continue ASA. Otherwise, no benefit over the placebo.
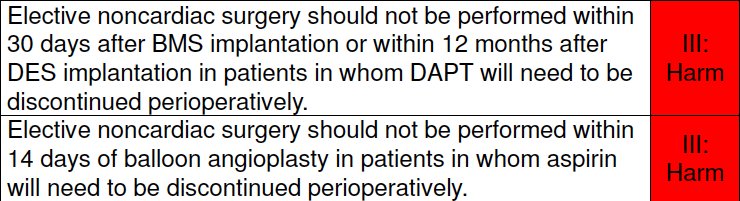
12/ Recent PCI and DAPT perioperatively
⚠️Stent thrombosis risk very high in 1st 4-6 weeks.
☑️Delay surgery for atleast 30 days (recent BMS) or 6 months (preferably 1 year; for DES)
Refer to the algorithm below.
⚠️Stent thrombosis risk very high in 1st 4-6 weeks.
☑️Delay surgery for atleast 30 days (recent BMS) or 6 months (preferably 1 year; for DES)
Refer to the algorithm below.


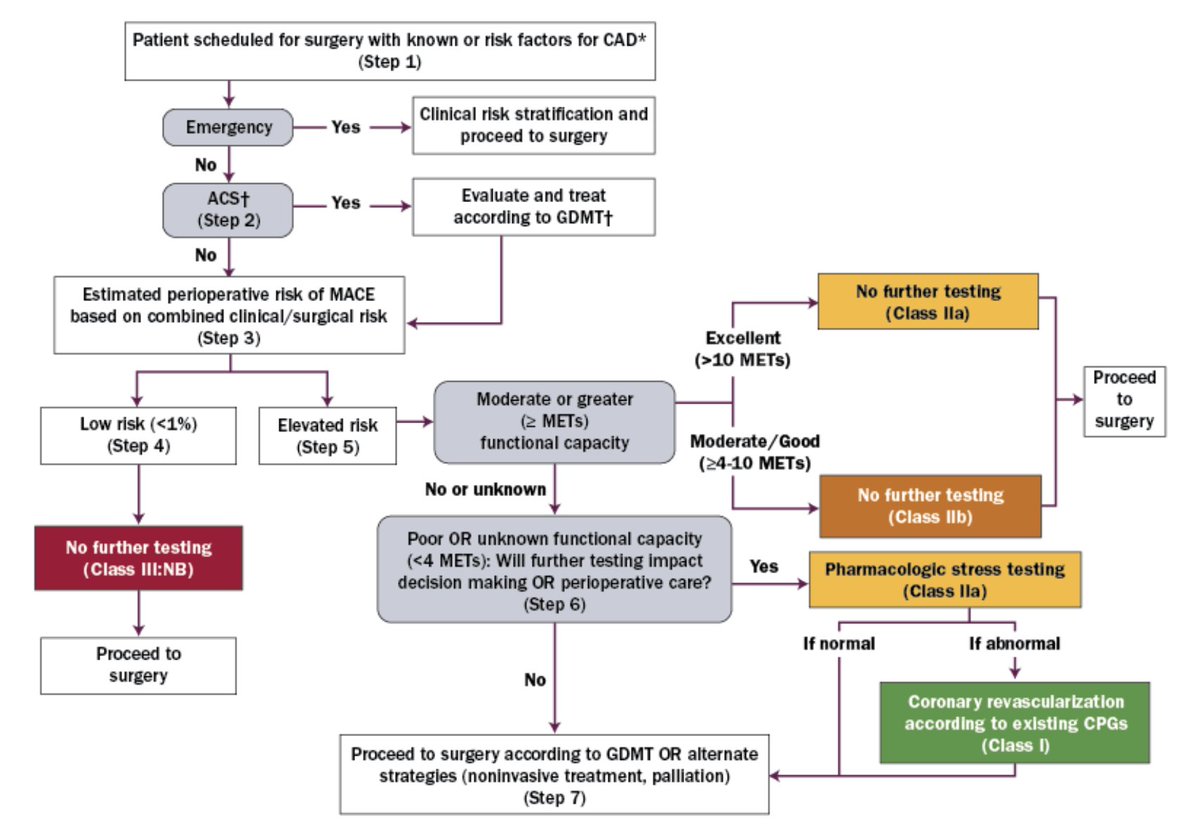
13/ Step wise approach for evaluating a patient preoperatively
14/ Summary
☑️Risk stratify, not “clear”
☑️Use “team” approach
☑️Use risk prediction 🛠️
☑️ Obtain good history and PE
☑️Use additional testing cautiously; can delay the surgery
☑️Manage meds, anti-platelets and pts with recent PCI carefully
☑️Remember the “DONTs”
☑️Risk stratify, not “clear”
☑️Use “team” approach
☑️Use risk prediction 🛠️
☑️ Obtain good history and PE
☑️Use additional testing cautiously; can delay the surgery
☑️Manage meds, anti-platelets and pts with recent PCI carefully
☑️Remember the “DONTs”