#FITSurvivalGuide: CV disease in Pregnancy #CardioObstetrics
#Tweetorial for new #CardiologyFIT by @MonSangh and @JennLewey @Penn
1⃣CV Physiology
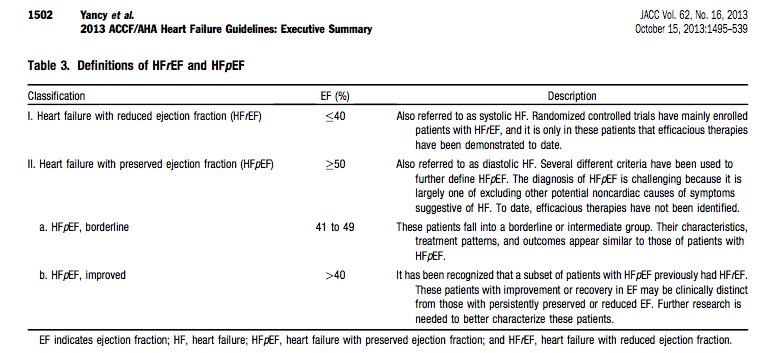
2⃣Peripartum CM
3⃣SCAD
4⃣Valve Dz
5⃣Aortopathy
6⃣Arrhythmias
7⃣HTN Disorders of 🤰
8⃣🤰& Future CV Risk
9⃣Drug Safety
#Tweetorial for new #CardiologyFIT by @MonSangh and @JennLewey @Penn
1⃣CV Physiology
2⃣Peripartum CM
3⃣SCAD
4⃣Valve Dz
5⃣Aortopathy
6⃣Arrhythmias
7⃣HTN Disorders of 🤰
8⃣🤰& Future CV Risk
9⃣Drug Safety
1⃣CV Physiology
**Major changes occur to meet metabolic & circulatory needs of 🚼.
🔸Hemodynamic: ⬇️SVR/BP ⬆️HR/CO ⬆️Plasma ↔️Filling pressure
🔸Structural: ⬆️Chamber/LV mass ⬆️Aortic Compliance
🔸Cardiometabolic: ⬆️Insulin resistance ⬆️Lipid/Trig
**Major changes occur to meet metabolic & circulatory needs of 🚼.
🔸Hemodynamic: ⬇️SVR/BP ⬆️HR/CO ⬆️Plasma ↔️Filling pressure
🔸Structural: ⬆️Chamber/LV mass ⬆️Aortic Compliance
🔸Cardiometabolic: ⬆️Insulin resistance ⬆️Lipid/Trig


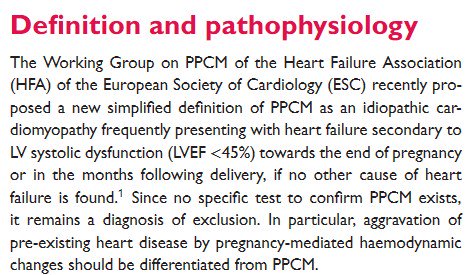
2⃣Peripartum Cardiomyopathy
🔸Epi: Blacks>>White
🔸Cause: Double-hit hypothesis
🔸Dx: Idiopathic, EF < 45%, ~ 1 m prior or 5 m after delivery
🔸Rx: HF tx; metoprolol/enalapril safe for lactation; ?bromocriptine, ?lactation
🔸LVEF recovery 👍 future risk
🔸Anticoagulation
🔸Epi: Blacks>>White
🔸Cause: Double-hit hypothesis
🔸Dx: Idiopathic, EF < 45%, ~ 1 m prior or 5 m after delivery
🔸Rx: HF tx; metoprolol/enalapril safe for lactation; ?bromocriptine, ?lactation
🔸LVEF recovery 👍 future risk
🔸Anticoagulation



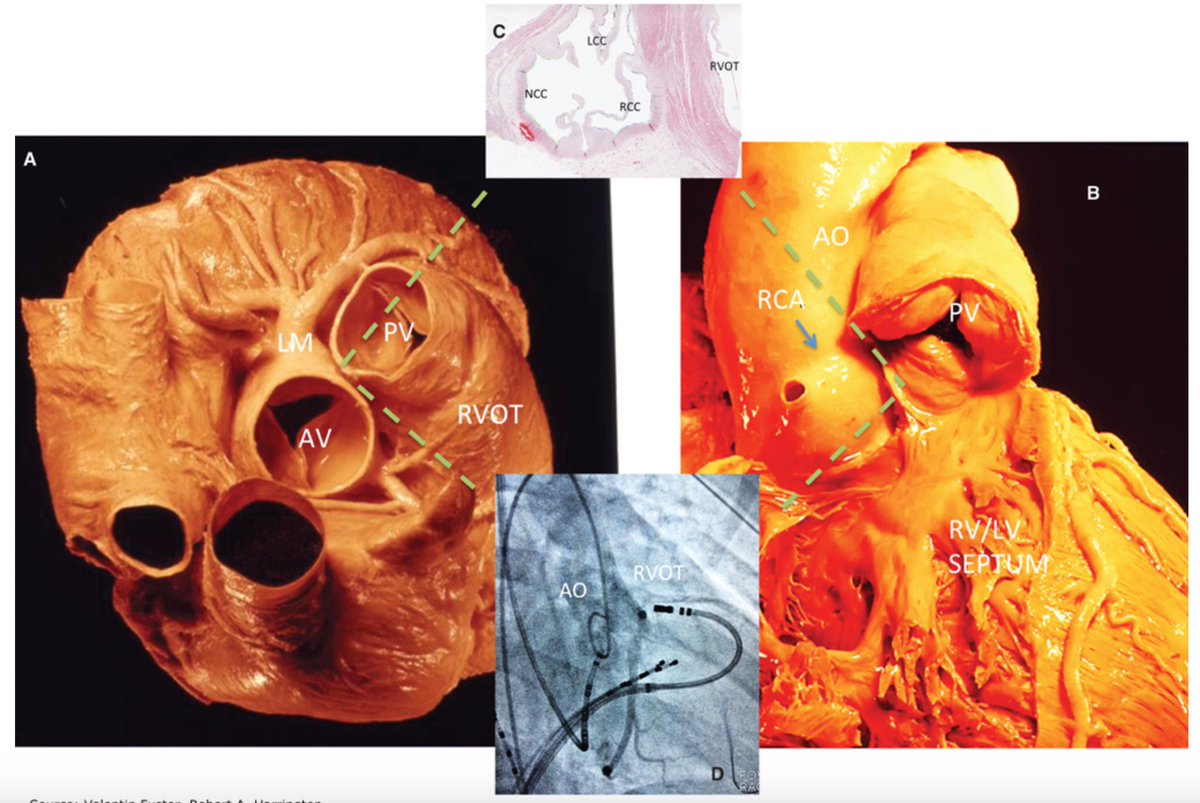
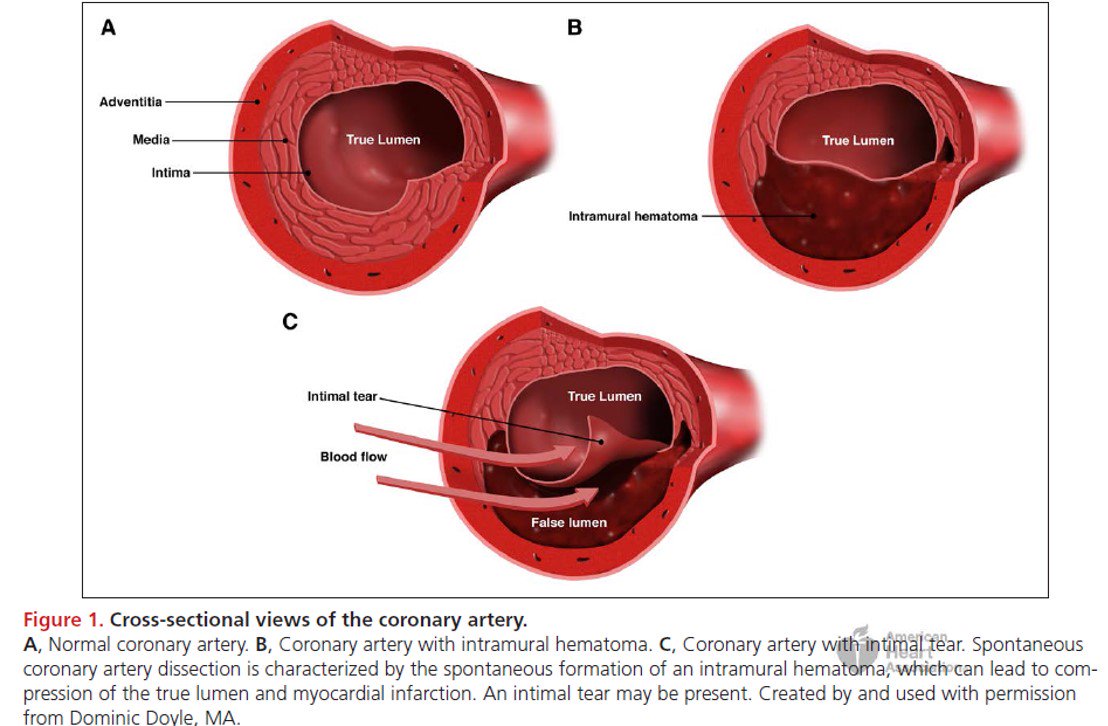
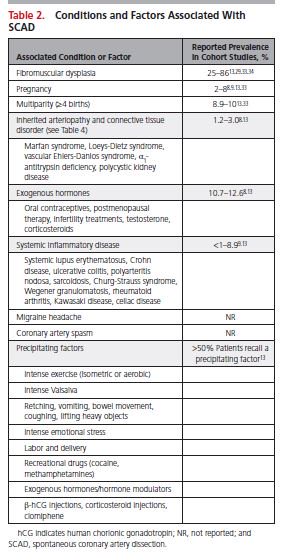
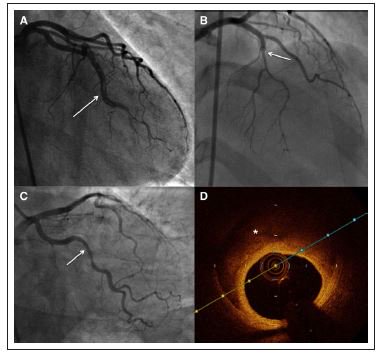
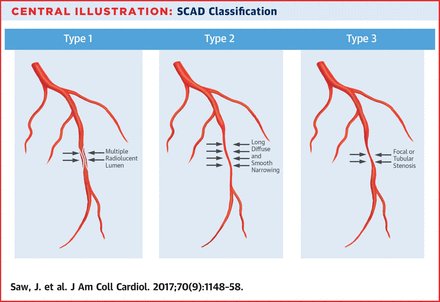
3⃣Spontaneous Coronary Artery Dissection (SCAD )
#SCAD -> AMI in 3rd tri & postpartum (most common cause)
🔸Get EKG & Tn in P & PP 👩🦰 with CP
🔸Dx made by cath
🔸Conservative tx (meds>>PCI)
🔸?prolonged IP obs
🔸Strong association with FMD
#SCAD -> AMI in 3rd tri & postpartum (most common cause)
🔸Get EKG & Tn in P & PP 👩🦰 with CP
🔸Dx made by cath
🔸Conservative tx (meds>>PCI)
🔸?prolonged IP obs
🔸Strong association with FMD
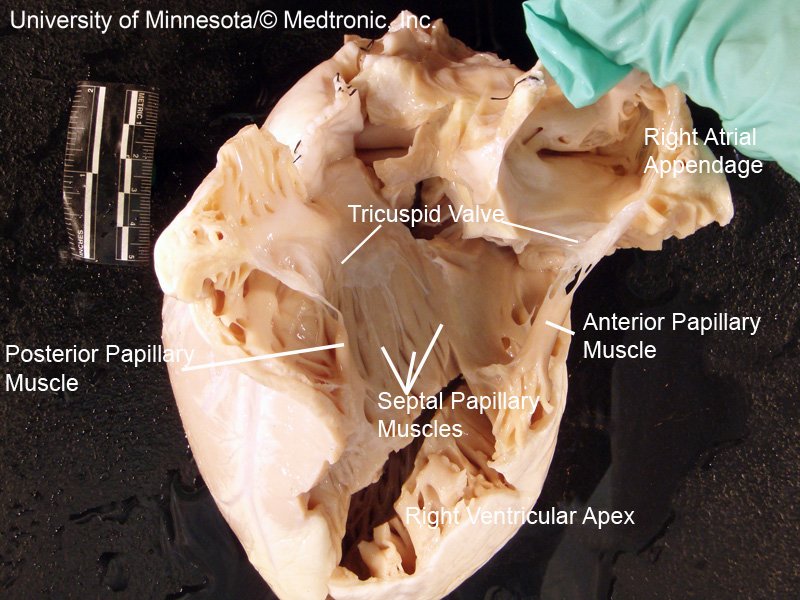
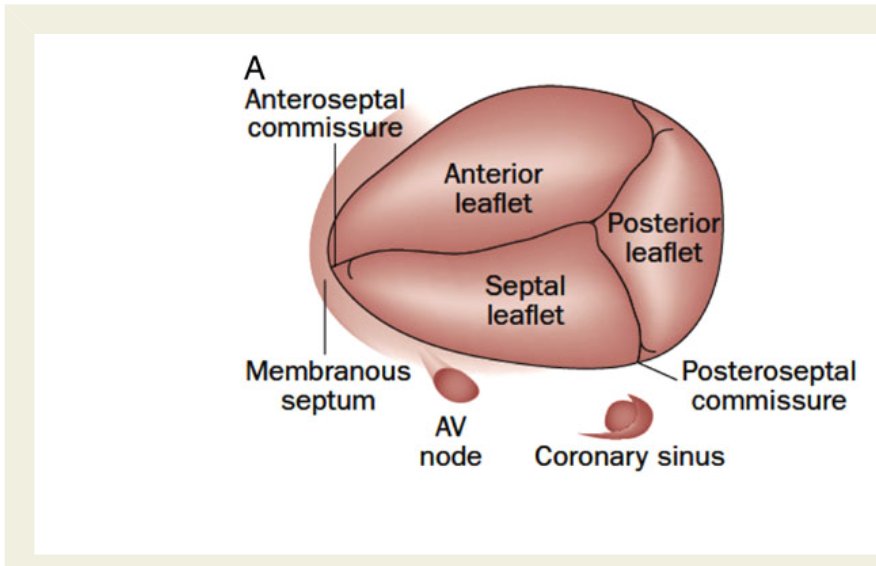
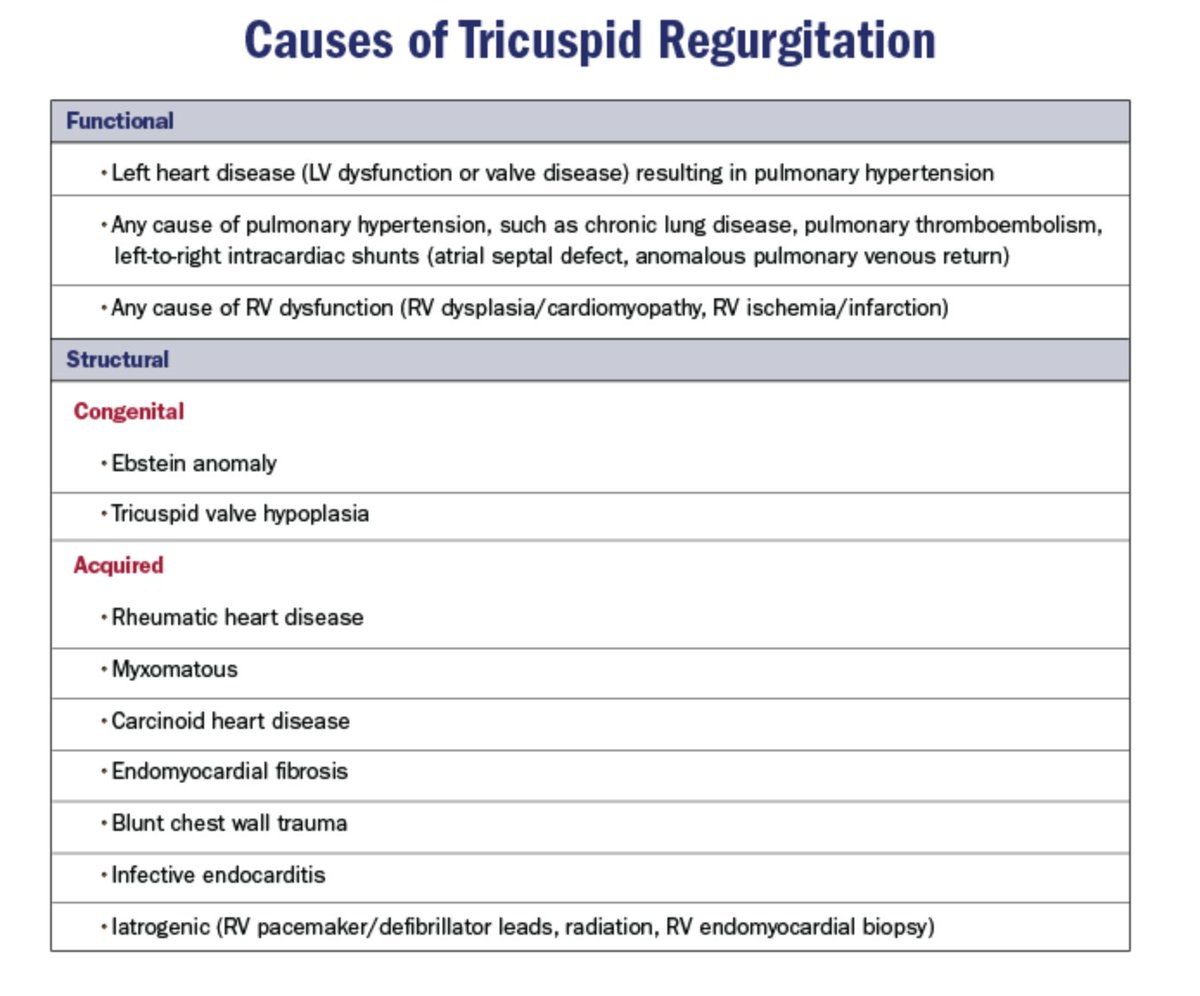
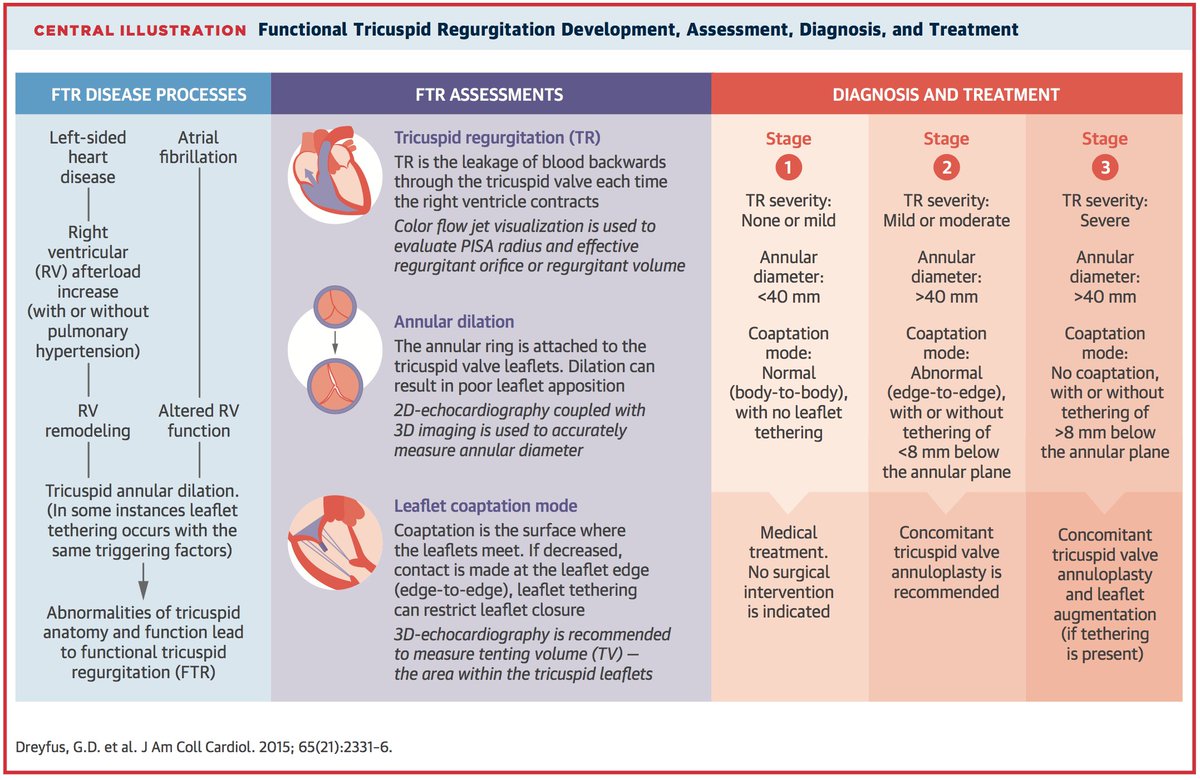
4⃣Valve Disease
🔸Regurg better tolerated than stenosis in 🤰
🔸Mitral Stenosis: CO ↑ MV gradient ↑ -> HF sx
▪️Tx: BB, Lasix, PMBV if refractory
🔸 Mech valves: (Controversy; ?Dose)
▪️2-3 Tri: Warfarin
▪️1 Tri: Warfarin vs Lovenox
🔸Regurg better tolerated than stenosis in 🤰
🔸Mitral Stenosis: CO ↑ MV gradient ↑ -> HF sx
▪️Tx: BB, Lasix, PMBV if refractory
🔸 Mech valves: (Controversy; ?Dose)
▪️2-3 Tri: Warfarin
▪️1 Tri: Warfarin vs Lovenox


5⃣Aortopathies
🔸High-risk for 🤰with aortic pathology, high mortality.
🔸Vascular Ehlers-Danlos pregnancy 🙅♀️
🔸Monitor with echo, MRI (q 4-12 weeks)
🔸Strict BP control (BB -> monitor fetal growth)
🔸Delivery: Continue BB, CS if (Ao >45mm, Acute/Chronic Dissection
🔸High-risk for 🤰with aortic pathology, high mortality.
🔸Vascular Ehlers-Danlos pregnancy 🙅♀️
🔸Monitor with echo, MRI (q 4-12 weeks)
🔸Strict BP control (BB -> monitor fetal growth)
🔸Delivery: Continue BB, CS if (Ao >45mm, Acute/Chronic Dissection


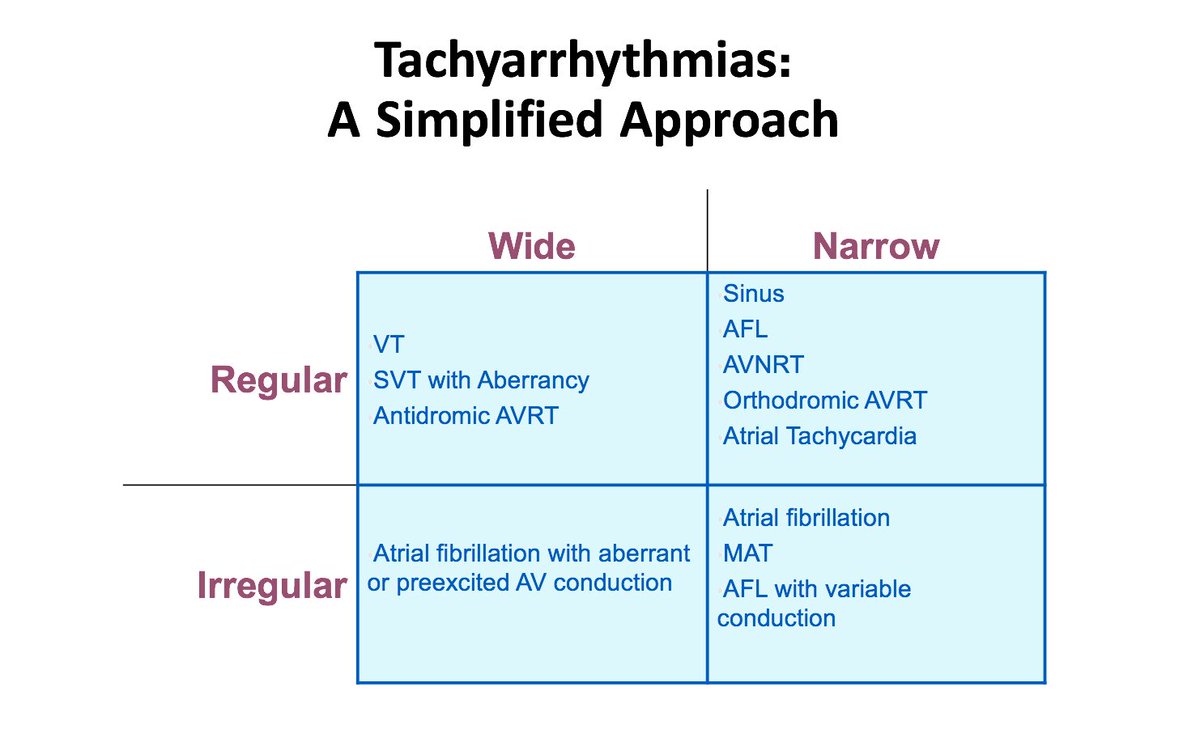
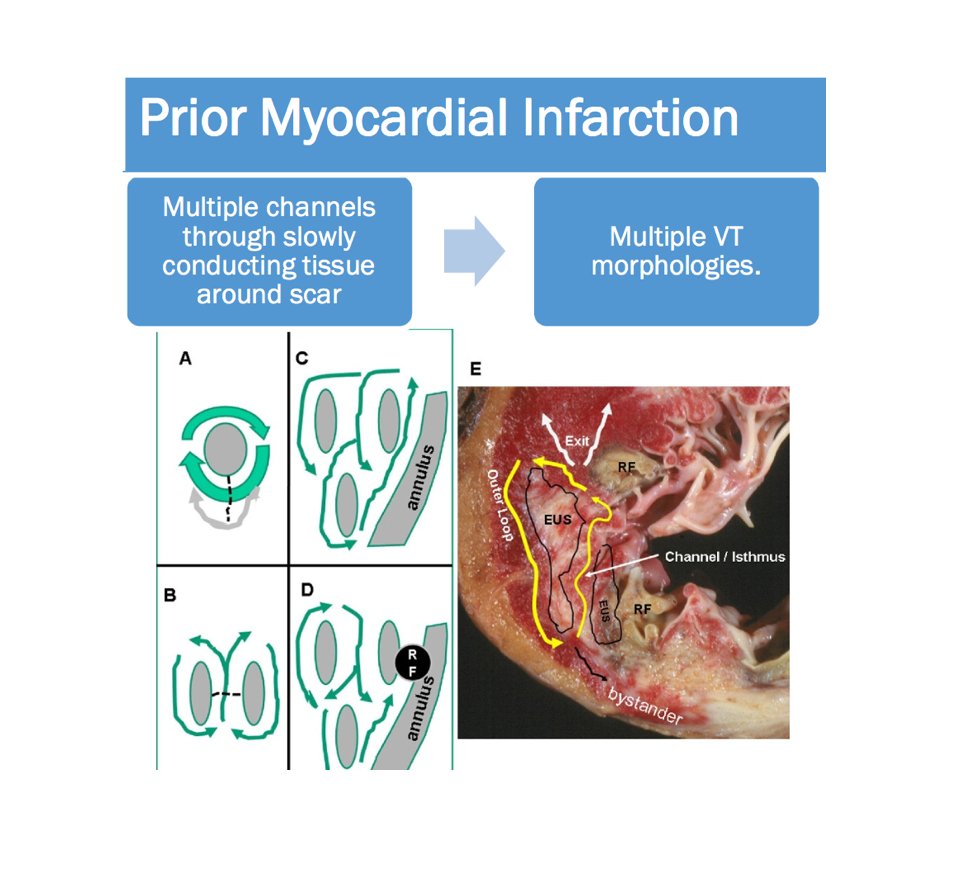
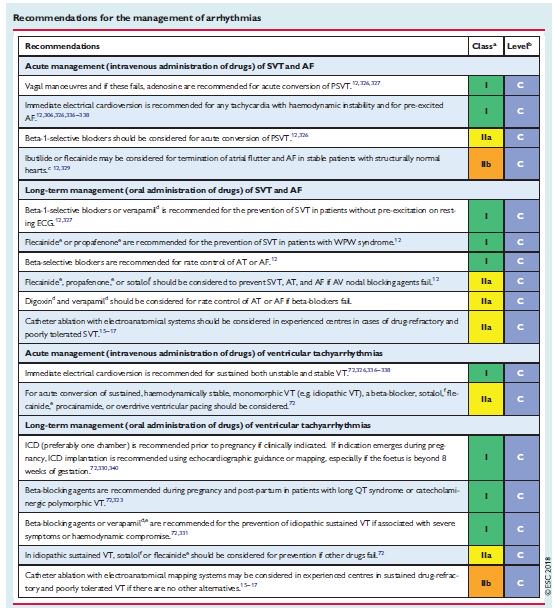
6⃣Arrhythmias in Pregnancy
🔸2/2 hemodynamic, hormonal, & autonomic changes
🔸Ectopy > AF and PSVT > VT/VF
🔸Tx (Similar):adenosine, bb, then antiarrhythmics
🔸Defer ablation 2nd tri if possible
🔸DCCV safe during entire pregnancy (monitor fetus)
ahajournals.org/doi/10.1161/CI…
🔸2/2 hemodynamic, hormonal, & autonomic changes
🔸Ectopy > AF and PSVT > VT/VF
🔸Tx (Similar):adenosine, bb, then antiarrhythmics
🔸Defer ablation 2nd tri if possible
🔸DCCV safe during entire pregnancy (monitor fetus)
ahajournals.org/doi/10.1161/CI…
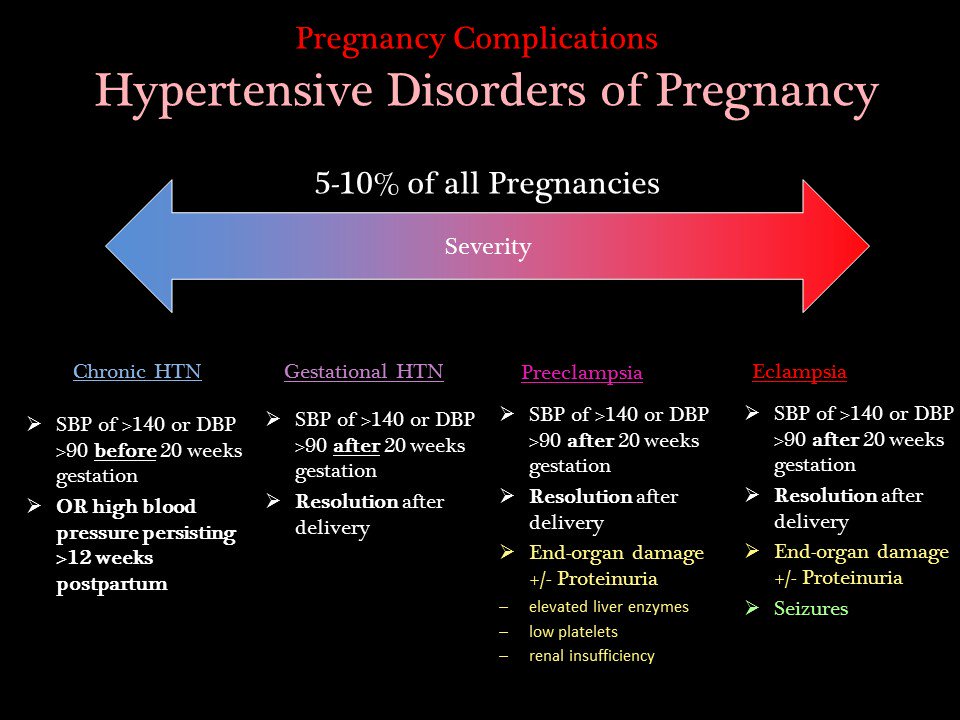
7⃣HTN Disorders of 🤰
🔸5-10% of pregnancies
🔸Diagnosis (see below)
🔸Tx: methyldopa, nifedipine, and/or labetalol during pregnancy
*C-htn: ?If SBP >160 (CHAPS study)
*Preeclampsia: Deliver
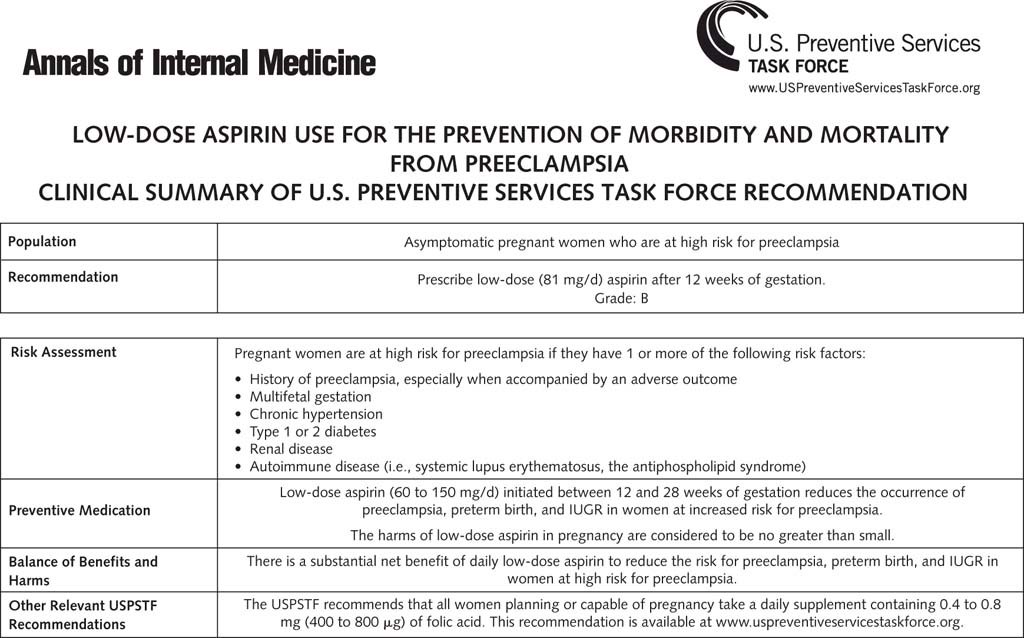
🔸ASA 1st Tri for preeclampsia prevention
sciencedirect.com/science/articl…
🔸5-10% of pregnancies
🔸Diagnosis (see below)
🔸Tx: methyldopa, nifedipine, and/or labetalol during pregnancy
*C-htn: ?If SBP >160 (CHAPS study)
*Preeclampsia: Deliver
🔸ASA 1st Tri for preeclampsia prevention
sciencedirect.com/science/articl…
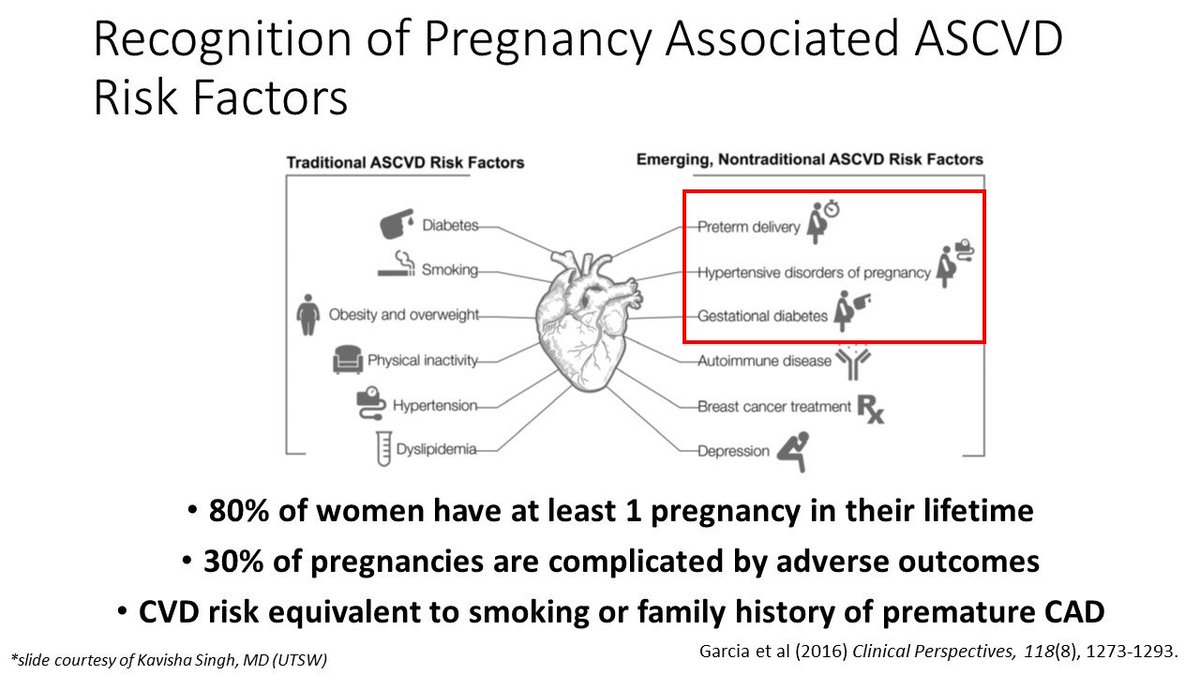
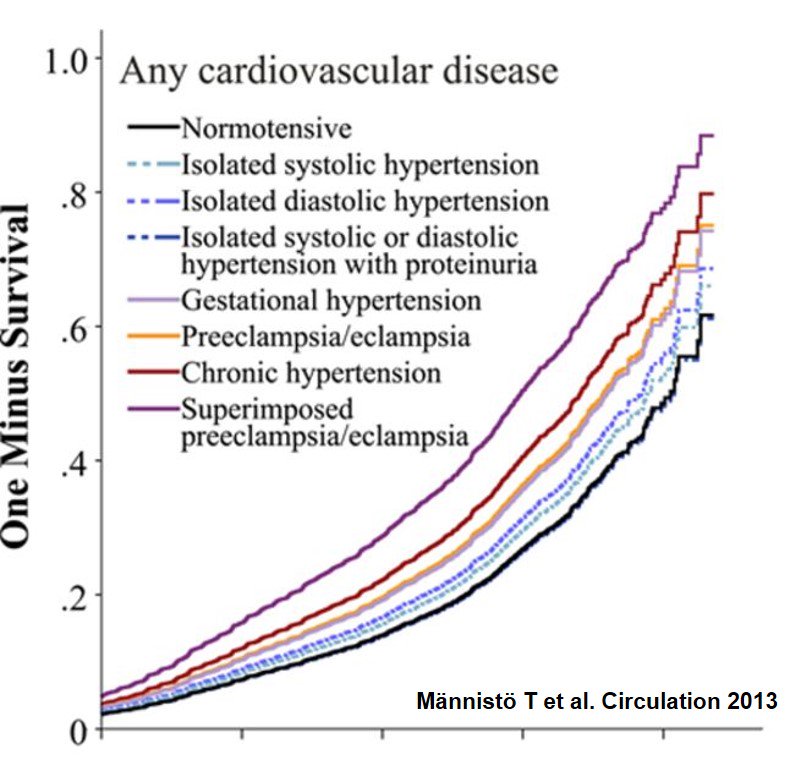
8⃣🤰& Future CV Risk
Pregnancy is "nature's stress test"
🔸Complications associated w/ ⬆️ risk of CVD (?predicts vs. causes)
- G-DM
- PE/G-HTN
- Preterm
- Small baby
🔸Recurrent/multiple complications ⬆️risk
🔸Important to take pregnancy hx!
Pregnancy is "nature's stress test"
🔸Complications associated w/ ⬆️ risk of CVD (?predicts vs. causes)
- G-DM
- PE/G-HTN
- Preterm
- Small baby
🔸Recurrent/multiple complications ⬆️risk
🔸Important to take pregnancy hx!

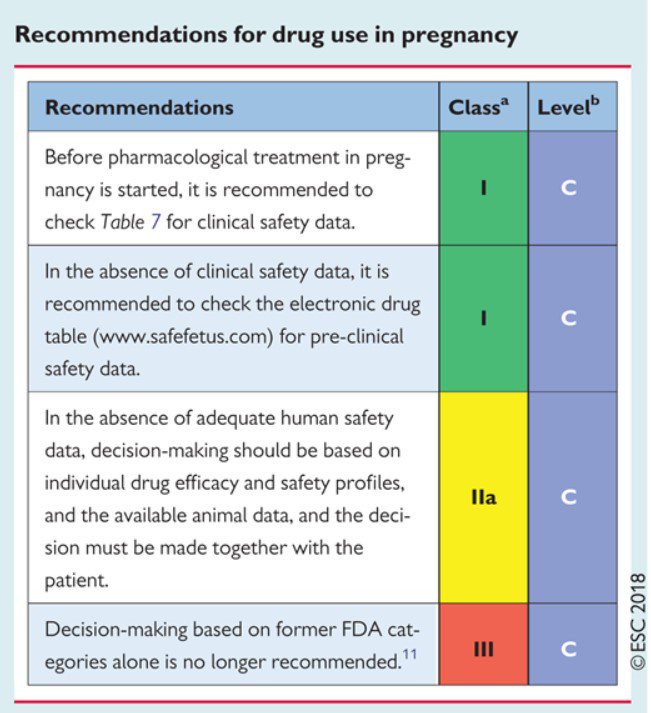
9⃣Drug Safety in Pregnancy
🔸Meds to avoid: ACEI, ARB, statin, amio
🔸Coumadin ok w/ mech valves (see above)
🔸A, B, C, D risk categories no longer preferred
🔸Consider Risks/Benefits
Websites:
medsmilk.com
safefetus.com
academic.oup.com/eurheartj/adva… (Table 7)
🔸Meds to avoid: ACEI, ARB, statin, amio
🔸Coumadin ok w/ mech valves (see above)
🔸A, B, C, D risk categories no longer preferred
🔸Consider Risks/Benefits
Websites:
medsmilk.com
safefetus.com
academic.oup.com/eurheartj/adva… (Table 7)
🔸That's a wrap! This is just the basics.
🔸Encourage comments/discussion.
🔸Follow hashtag #CardioObstretrics for updates
🔸Encourage comments/discussion.
🔸Follow hashtag #CardioObstretrics for updates