1/14 I’ve never sent a patient to a nursing home for low aerobic endurance, but I’ve sent MANY for low physical strength.
My 1st MedEd #tweetorial pairs w/ our appearance on the @thecurbsiders podcast exploring an under-recognized and critically important problem: SARCOPENIA.
My 1st MedEd #tweetorial pairs w/ our appearance on the @thecurbsiders podcast exploring an under-recognized and critically important problem: SARCOPENIA.
2/14 The term describes a decrease in muscle mass and muscle strength, drawing from the Greek roots sarx- (“flesh”), and -penia (“poverty”).
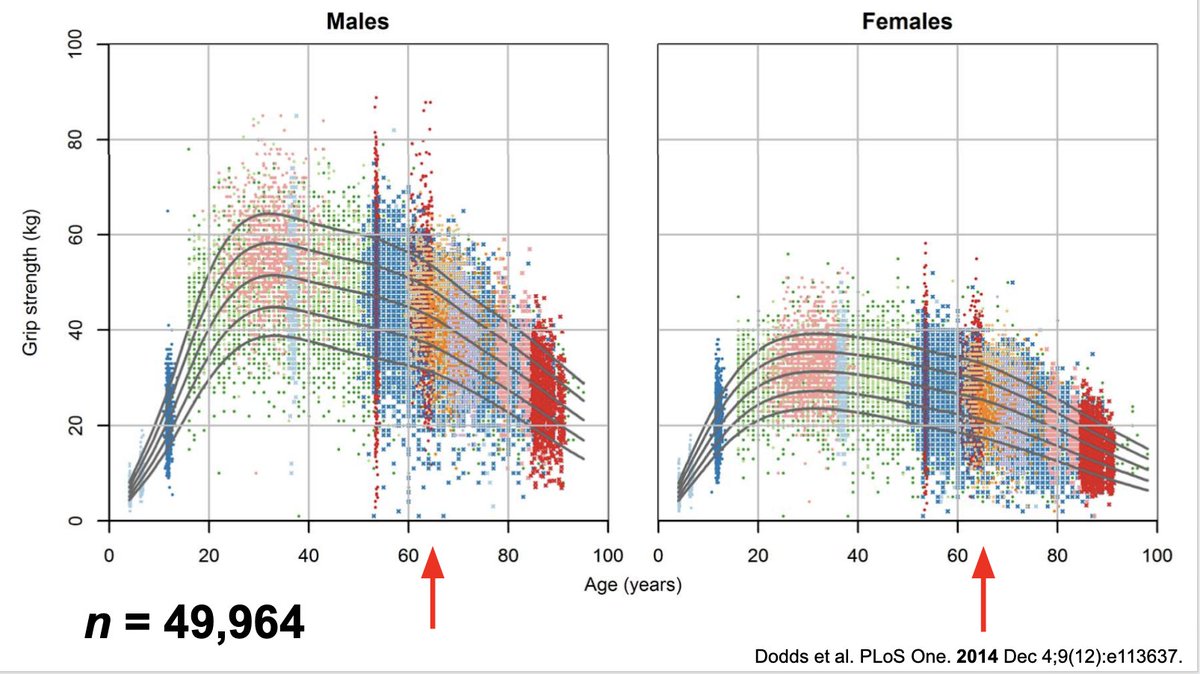
3/14 Physically inactive adults lose 3-8% muscle mass per decade from age 30; accelerates after age 50 → 40-50% muscle loss between age 20 and 80! Physical activity guidelines give strong recommendation for 2x/wk strength training, but this is only met by ¼ of the population! 
4/14 Sarcopenia is a strong independent predictor of hospitalization, re-admission, and all-cause, CV, and cancer mortality. One finding I always point out to students/residents: check out in-hospital mortality risk with LOW admission creatinine (reflective of low muscle mass)!

5/14 True prevalence is difficult to pinpoint due to lack of consensus on diagnostic criteria/cutoffs; estimates range 5-15% in community up to 60% in long-term care. In 2000, estimated costs directly attributable to sarcopenia in the US: $18.5 BILLION! ncbi.nlm.nih.gov/pubmed/14687319
6/14 Sarcopenia can occur w/ low/normal or high bodyfat (sarcopenic obesity), making dx tough (vs. cachexia = obvious, severe loss of lean AND fat mass 2/2 inflammation). Sarcopenia can also be acute (up to 20-40% muscle loss in the first 10 d of critical illness!) or chronic.

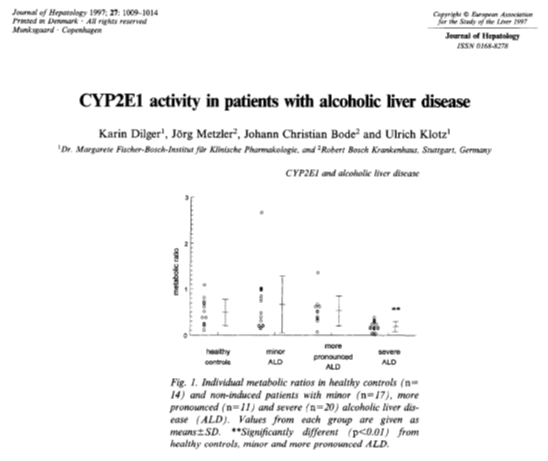
7/14 Complex, variable pathophysiology between individuals; results when muscle protein breakdown > synthesis. Common drivers: inactivity, poor nutrition, drugs (eg. steroids, chemo), chronic inflammation (eg. met. syndrome, HF, COPD, CKD/ESRD, cirrhosis, cancer, autoimmune dz).

8/14 Aging, inactivity, acute illness and chronic disease → ANABOLIC RESISTANCE, characterized by a blunted response to anabolic stimuli (muscle contraction + dietary protein). Individuals become more refractory the more cachectic they become → early intervention is key!

9/14 Good news: this can be overcome with higher dose of stimulus! Individuals may have blunted/no anabolic response to a meal w/ 0.2 g/kg protein → incr. to 0.4-0.6 g/kg/meal and response is maximized! Same has been shown with exercise volume.

10/14 Int’l groups have proposed diagnostic pathways for sarcopenia. In practice I skip quantitation of muscle mass due to low risk of “overtreating” false positives w/ exercise/nutrition. If anabolic drugs become widely used in the future, may require more rigorous dx approach.

11/14 Quick strength/performance screens: 5x chair sit-to-stand >15 s, Timed Up/Go >20 s, Gait speed <0.8 m/s. If positive → maximize anabolic stimuli, minimize catabolic stimuli to the extent possible, but EVERYONE should receive exercise counseling esp. RESISTANCE exercise!
12/14 Exercise: 2018 Physical Activity Guidelines recommend whole-body strength training of moderate or greater intensity at least 2x/wk. May need higher doses for clinical populations - APTA Choosing Wisely Guidelines recognize importance of individualized exercise dosing!

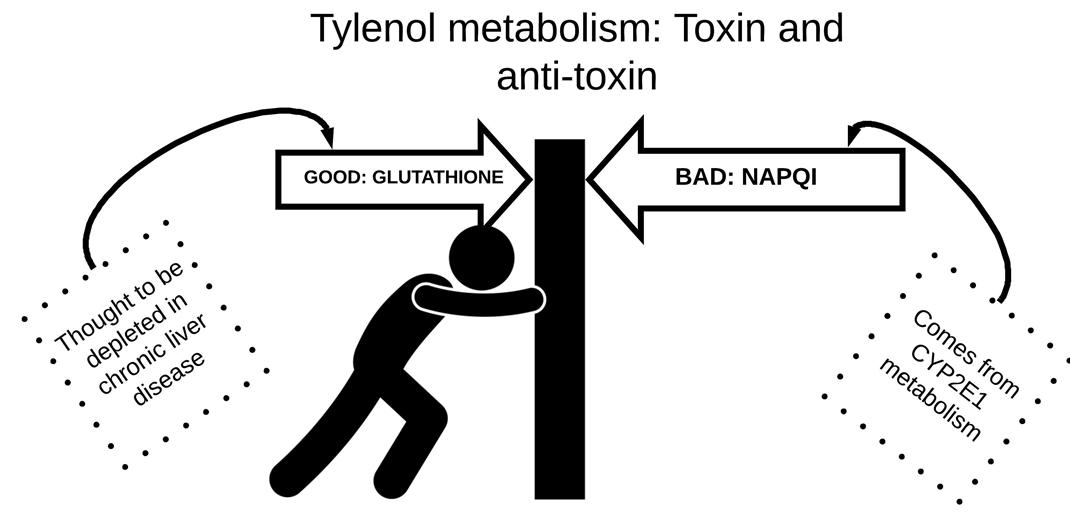
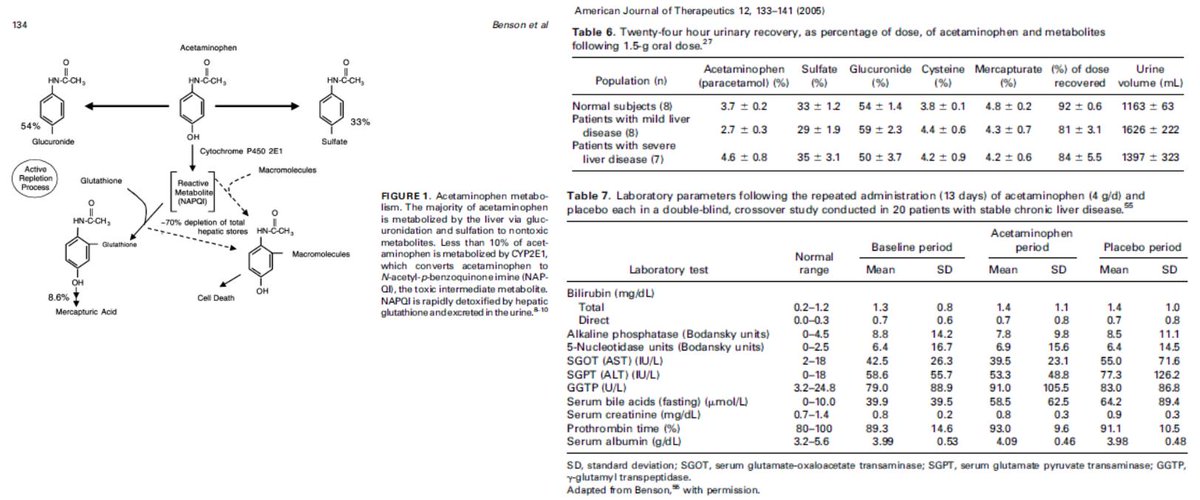
13/14 Dietary protein: evidence suggests 1.2-1.6 g/kg/d improves outcomes vs. RDA @ 0.8 g/kg/d. No evidence of harm in healthy individuals or w/ liver disease; in CKD consider risks/benefits of restriction - if restricted, exercise even more essential! ncbi.nlm.nih.gov/pubmed/26960445
14/14 Summary:
-Sarcopenia = loss of muscle mass and function
-Independent risk factor for hospitalization & mortality
-Widely prevalent yet under-recognized, especially w/ obesity
-Treatable w/ strength training & dietary protein, but DOSE matters due to anabolic resistance!
-Sarcopenia = loss of muscle mass and function
-Independent risk factor for hospitalization & mortality
-Widely prevalent yet under-recognized, especially w/ obesity
-Treatable w/ strength training & dietary protein, but DOSE matters due to anabolic resistance!