1/
How common is loss of smell (anosmia) in #SARSCoV2 #COVID19, and how useful is it for ruling the diagnosis in or out? Let’s take a look at the data.
Here’s a quick #HowIReadThisPaper on two @AnnalsofEM papers addressing this question:
Chua et al
&
Peyroney et al
(Thread)
How common is loss of smell (anosmia) in #SARSCoV2 #COVID19, and how useful is it for ruling the diagnosis in or out? Let’s take a look at the data.
Here’s a quick #HowIReadThisPaper on two @AnnalsofEM papers addressing this question:
Chua et al
&
Peyroney et al
(Thread)
2/
First, a question:
Let’s assume you have a limited supply of swabs and need to prioritize which patients to test for COVID19.
In which skilled nursing facility (SNF) setting would you expect anosmia to be more useful in identifying patients who will test positive?
First, a question:
Let’s assume you have a limited supply of swabs and need to prioritize which patients to test for COVID19.
In which skilled nursing facility (SNF) setting would you expect anosmia to be more useful in identifying patients who will test positive?
3/
Chua et al annemergmed.com/article/S0196-…
Question: What are the test characteristics of acute olfactory loss (hyposmia or anosmia for <14d) for Dx of COVID19, using oropharyngeal PCR as the gold standard?
Design: single-center cross-sectional study via chart review (retrospective)
Chua et al annemergmed.com/article/S0196-…
Question: What are the test characteristics of acute olfactory loss (hyposmia or anosmia for <14d) for Dx of COVID19, using oropharyngeal PCR as the gold standard?
Design: single-center cross-sectional study via chart review (retrospective)
4/
Population: 717 patients presenting to a single ED in Singapore from 3/23/2020 - 4/4/2020
Procedures: All patients tested for COVID-19 via OP swab (those with respiratory symptoms or recent travel) were also asked about hyposmia & anosmia from 3/23/3030 onward.
Population: 717 patients presenting to a single ED in Singapore from 3/23/2020 - 4/4/2020
Procedures: All patients tested for COVID-19 via OP swab (those with respiratory symptoms or recent travel) were also asked about hyposmia & anosmia from 3/23/3030 onward.
5/
Results:
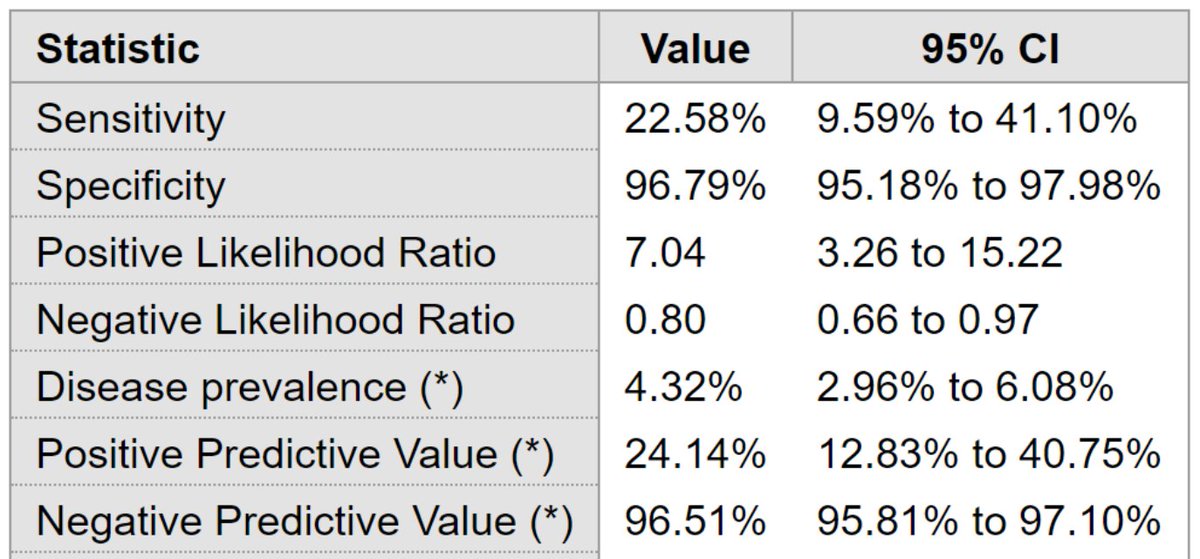
31/717 (4.3%) patients were positive for COVID19. Only 2 had isolated acute olfactory loss; all others had associated URI Sx.
For hyposmia + anosmia combined:
Feeling frequentist?
Sensitivity: 22.6%
Specificity: 96.8%
Better off Bayesian?
PPV: 24.1%
NPV: 96.5%
Results:
31/717 (4.3%) patients were positive for COVID19. Only 2 had isolated acute olfactory loss; all others had associated URI Sx.
For hyposmia + anosmia combined:
Feeling frequentist?
Sensitivity: 22.6%
Specificity: 96.8%
Better off Bayesian?
PPV: 24.1%
NPV: 96.5%

6/
Author's conclusions: among patients presenting to the ED with respiratory symptoms, hyposmia and anosmia are highly specific (but not at all sensitive) for the diagnosis of COVID-19. PPV was low, but NPV was high.
How should we use these results?
A few thoughts:
Author's conclusions: among patients presenting to the ED with respiratory symptoms, hyposmia and anosmia are highly specific (but not at all sensitive) for the diagnosis of COVID-19. PPV was low, but NPV was high.
How should we use these results?
A few thoughts:
7/
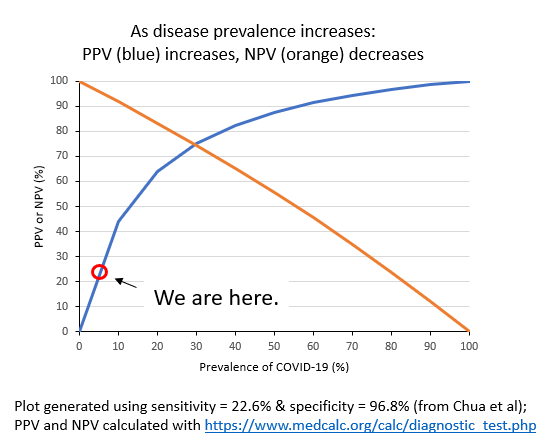
Plotting PPV and NPV against prevalence of COVID19 reveals that as prevalence ↑, PPV ↑, and NPV ↓.
In this study the prevalence of COVID19 was 4.3%, which corresponds to a PPV of 24.1%. This means that only 24.1% of patients with anosmia actually had COVID19.
Plotting PPV and NPV against prevalence of COVID19 reveals that as prevalence ↑, PPV ↑, and NPV ↓.
In this study the prevalence of COVID19 was 4.3%, which corresponds to a PPV of 24.1%. This means that only 24.1% of patients with anosmia actually had COVID19.
8/
You can see why this is bad. A PPV of <50% means that more than half of people with acute olfactory loss will test negative for COVID19!
But – what about the specificity of 96.8%, doesn’t that mean anosmia should be useful for ruling in COVID19?
You can see why this is bad. A PPV of <50% means that more than half of people with acute olfactory loss will test negative for COVID19!
But – what about the specificity of 96.8%, doesn’t that mean anosmia should be useful for ruling in COVID19?
9/
Yes, but at the cost of many false positives when the disease is rare.
Therefore, acute olfactory loss is not really useful when disease prevalence is low.
What about when disease prevalence is high? Let’s take a look at the second paper to find out.
Yes, but at the cost of many false positives when the disease is rare.
Therefore, acute olfactory loss is not really useful when disease prevalence is low.
What about when disease prevalence is high? Let’s take a look at the second paper to find out.
10/
Peyrony et al annemergmed.com/article/S0196-…
Question: What are the test characteristics of anosmia (among other things) for diagnosis of COVID19, using nasal PCR as the gold standard?
Design: single-center prospective cohort study
Peyrony et al annemergmed.com/article/S0196-…
Question: What are the test characteristics of anosmia (among other things) for diagnosis of COVID19, using nasal PCR as the gold standard?
Design: single-center prospective cohort study
11/
Population: 391 patients presenting to a single ED in France from 3/9/2020 - 4/4/2020
Procedures: Testing (via nasal swab) was clinically driven; dyspneic, older, and sicker patients were more likely to be tested. Patients were only asked about anosmia from 3/24/3030 onward.
Population: 391 patients presenting to a single ED in France from 3/9/2020 - 4/4/2020
Procedures: Testing (via nasal swab) was clinically driven; dyspneic, older, and sicker patients were more likely to be tested. Patients were only asked about anosmia from 3/24/3030 onward.
12/
Results:
225/391 (58%) patients were positive for COVID19; 31 patients testing positive reported anosmia, compared with 3 who tested negative.
For anosmia:
Sensitivity: 14%
Specificity: 98%
PPV: 91%
NPV: 46%
Results:
225/391 (58%) patients were positive for COVID19; 31 patients testing positive reported anosmia, compared with 3 who tested negative.
For anosmia:
Sensitivity: 14%
Specificity: 98%
PPV: 91%
NPV: 46%


13/
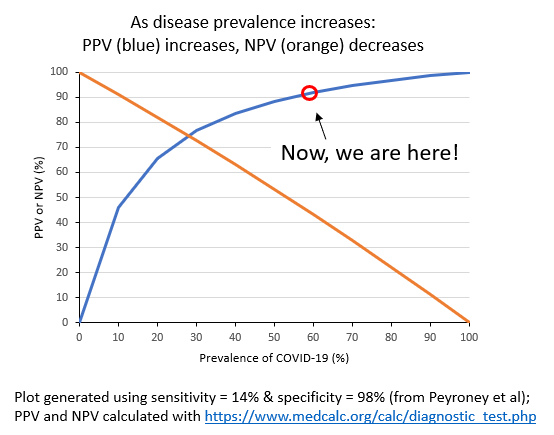
The sensitivity & specificity are similar to the estimates by Chua et al, but we see that at a much higher prevalence of COVID19 of ~60%, the PPV of anosmia goes up to 91%!
The sensitivity & specificity are similar to the estimates by Chua et al, but we see that at a much higher prevalence of COVID19 of ~60%, the PPV of anosmia goes up to 91%!
14/
How could chance & bias affect these results?
We know that asymptomatic COVID19 infections and false neg PCRs are common.
In both studies, testing was based on Sx, so the denominators are missing asymptomatic pts, but this should not affect specificity & PPV of anosmia:
How could chance & bias affect these results?
We know that asymptomatic COVID19 infections and false neg PCRs are common.
In both studies, testing was based on Sx, so the denominators are missing asymptomatic pts, but this should not affect specificity & PPV of anosmia:

15/
Also, false neg PCRs could misclassify patients positive for COVID19 as negative, and in Peyrony et al, patients were only asked about anosmia for half the study period.
These could both affect specificity & PPV, but in which direction?
The net effect is hard to know.
Also, false neg PCRs could misclassify patients positive for COVID19 as negative, and in Peyrony et al, patients were only asked about anosmia for half the study period.
These could both affect specificity & PPV, but in which direction?
The net effect is hard to know.

16/
Revisiting the original question:
Assuming you have a limited supply of swabs and need to prioritize who to test for COVID19:
In which skilled nursing facility (SNF) setting would you expect anosmia to be more useful in identifying patients who will test positive?
Revisiting the original question:
Assuming you have a limited supply of swabs and need to prioritize who to test for COVID19:
In which skilled nursing facility (SNF) setting would you expect anosmia to be more useful in identifying patients who will test positive?
17/
Bottom line: At low prevalence of COVID19, the PPV of acute olfactory loss (anosmia) is also low: more false positives than true positives are likely below a prevalence of 10-15%.
As prevalence ↑, the PPV of anosmia also ↑: at a prevalence of ~60%, the PPV is >90%.
(End)
Bottom line: At low prevalence of COVID19, the PPV of acute olfactory loss (anosmia) is also low: more false positives than true positives are likely below a prevalence of 10-15%.
As prevalence ↑, the PPV of anosmia also ↑: at a prevalence of ~60%, the PPV is >90%.
(End)