1/
Should we use #Lopinavir-ritonavir (LPV/r) + #Ribavirin (RBV) +/- #Interferon beta-1b (IFN) to treat #SARSCoV2 #COVID19? Let’s take a look at the data.
Here’s: #HowIReadThisPaper on @TheLancet trial of triple therapy for COVID19
Hung et al: thelancet.com/journals/lance…
Should we use #Lopinavir-ritonavir (LPV/r) + #Ribavirin (RBV) +/- #Interferon beta-1b (IFN) to treat #SARSCoV2 #COVID19? Let’s take a look at the data.
Here’s: #HowIReadThisPaper on @TheLancet trial of triple therapy for COVID19
Hung et al: thelancet.com/journals/lance…

2/
First, let’s assess our baseline beliefs about triple therapy:
Before reading this study, when considering triple therapy as a treatment for patients with COVID19, I think the most important component is likely to be:
First, let’s assess our baseline beliefs about triple therapy:
Before reading this study, when considering triple therapy as a treatment for patients with COVID19, I think the most important component is likely to be:
3/
Background: A 2003 case series suggested ↓mortality (vs historical controls) in SARS patients treated with LPV/r + RBV :
ncbi.nlm.nih.gov/pmc/articles/P…
In 2015, LPV/r and IFN led to ↓viral load and improved clinical outcomes in animal models of MERS:
pubmed.ncbi.nlm.nih.gov/26198719/
Background: A 2003 case series suggested ↓mortality (vs historical controls) in SARS patients treated with LPV/r + RBV :
ncbi.nlm.nih.gov/pmc/articles/P…
In 2015, LPV/r and IFN led to ↓viral load and improved clinical outcomes in animal models of MERS:
pubmed.ncbi.nlm.nih.gov/26198719/
4/
Question: Does the triple combo of LPV/r + RBV +/- IFN reduce viral load and improve clinical outcomes in patients hospitalized with COVID19?
Date Published: 8 May 2020
Funding: Foundations + individuals; no drug manufacturer support
Question: Does the triple combo of LPV/r + RBV +/- IFN reduce viral load and improve clinical outcomes in patients hospitalized with COVID19?
Date Published: 8 May 2020
Funding: Foundations + individuals; no drug manufacturer support
5/
Study Design: Multicenter, randomized, open-label (unblinded) active-controlled (no placebo group) superiority trial
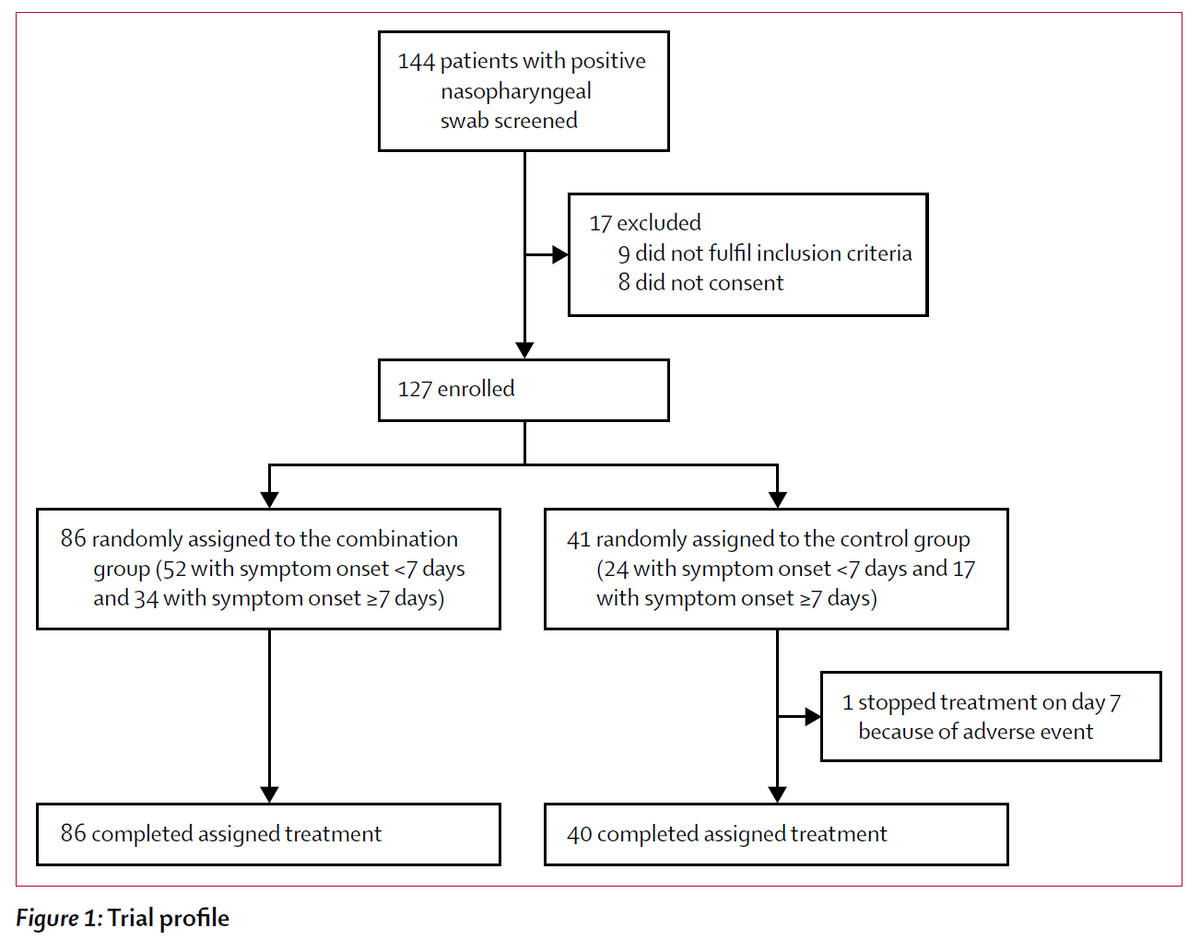
Population: 127 adults hospitalized with PCR-confirmed COVID19 at 6 hospitals in Hong Kong were included
Study Period: 2/10/2020 - 3/20/2020
Study Design: Multicenter, randomized, open-label (unblinded) active-controlled (no placebo group) superiority trial
Population: 127 adults hospitalized with PCR-confirmed COVID19 at 6 hospitals in Hong Kong were included
Study Period: 2/10/2020 - 3/20/2020
6/
Intervention: 14d of:
LPV/r (PO)
+
RBV (PO)
+/-
IFN (SubQ)
3 doses if 1-2d of Sx; 2 doses if 3-4d of Sx, 1 dose if 5-6d of Sx, 0 doses if >6d of Sx
+
Usual care
Control: LPV/r x14d + usual care
Usual care = any level of O2, dialysis, steroids, or ABx as indicated
Intervention: 14d of:
LPV/r (PO)
+
RBV (PO)
+/-
IFN (SubQ)
3 doses if 1-2d of Sx; 2 doses if 3-4d of Sx, 1 dose if 5-6d of Sx, 0 doses if >6d of Sx
+
Usual care
Control: LPV/r x14d + usual care
Usual care = any level of O2, dialysis, steroids, or ABx as indicated
7/
Study Procedures: Consecutively admitted patients were enrolled within 48h and randomized 2:1 (triple therapy : control) without stratification.
All patients requiring O2 received stress-dose steroids.
Daily swabs for PCR from multiple sites were collected until discharge.
Study Procedures: Consecutively admitted patients were enrolled within 48h and randomized 2:1 (triple therapy : control) without stratification.
All patients requiring O2 received stress-dose steroids.
Daily swabs for PCR from multiple sites were collected until discharge.
8/
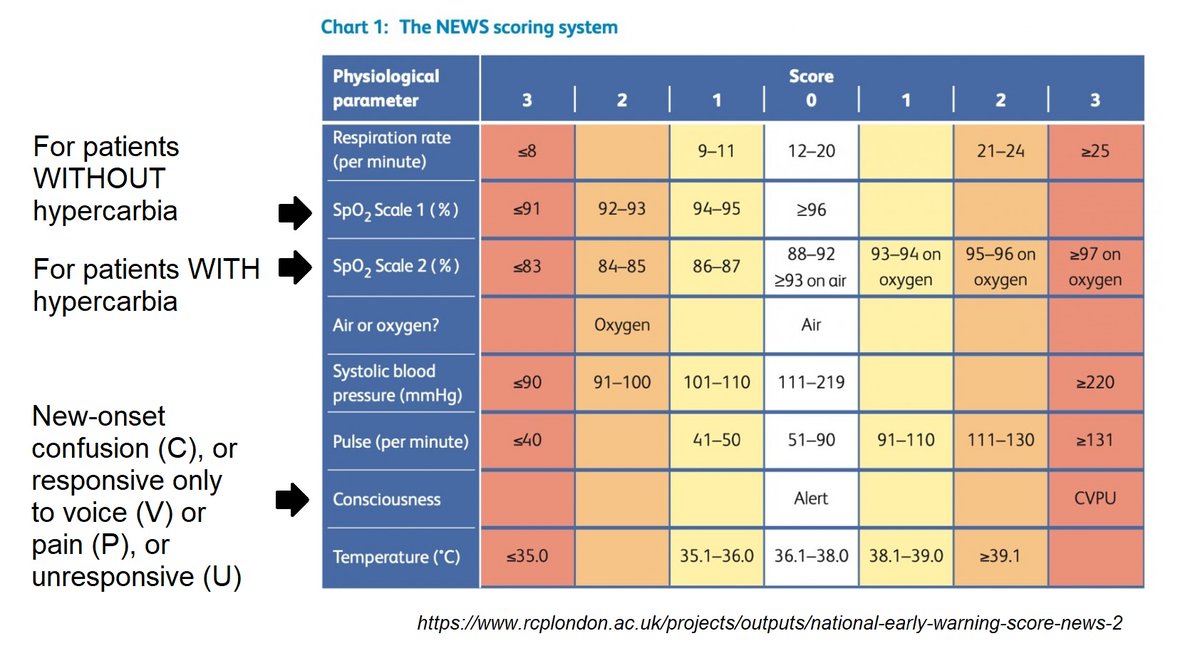
Inclusion Criteria: Age >18, hospitalization with RT-PCR confirmed, symptomatic SARSCoV2 + <14d of Sx onset, NEWS2 score =>1 (see pic)
Exclusion Criteria: QTc > 480 msec, Hx of VT, heart block, depression, or alcohol or substance use disorders; pregnant or breastfeeding women
Inclusion Criteria: Age >18, hospitalization with RT-PCR confirmed, symptomatic SARSCoV2 + <14d of Sx onset, NEWS2 score =>1 (see pic)
Exclusion Criteria: QTc > 480 msec, Hx of VT, heart block, depression, or alcohol or substance use disorders; pregnant or breastfeeding women
9/
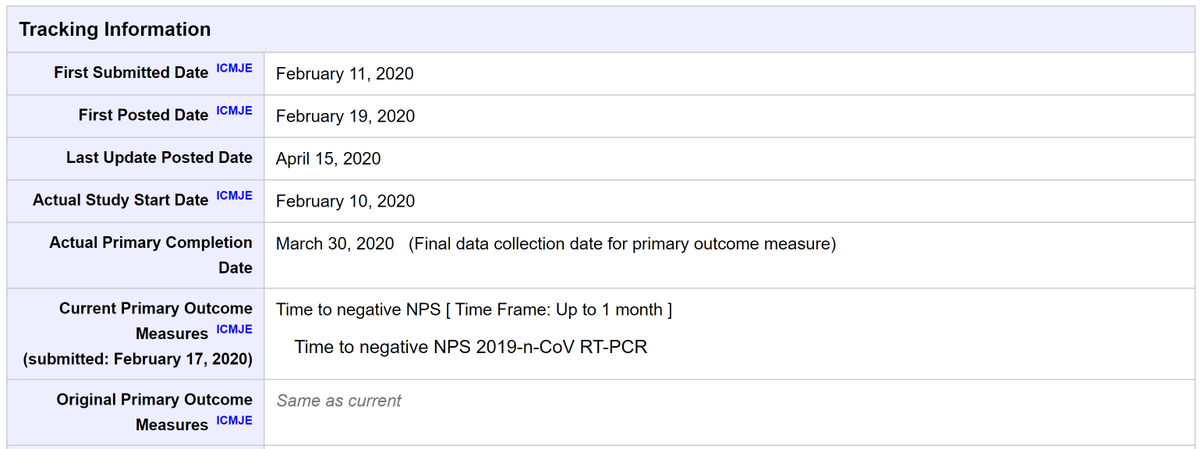
Protocol available? Yes: clinicaltrials.gov/ct2/show/recor…
Primary outcome: Time to negative nasopharyngeal swab PCR
Secondary outcomes: Resolution of Sx (defined as NEWS2=0 for >24h), LOS, 30-day mortality, detection of mutations, adverse events
Protocol available? Yes: clinicaltrials.gov/ct2/show/recor…
Primary outcome: Time to negative nasopharyngeal swab PCR
Secondary outcomes: Resolution of Sx (defined as NEWS2=0 for >24h), LOS, 30-day mortality, detection of mutations, adverse events
10/
Primary analysis: Time-to-event, intention-to-treat population
Sample size justification: 70 patients = 80% power (w/ 2-sided alpha 0.05) to detect a 26% absolute reduction in 21-day mortality or ARDS (allowing 17% dropout) assuming event rate of 29% in the control group
Primary analysis: Time-to-event, intention-to-treat population
Sample size justification: 70 patients = 80% power (w/ 2-sided alpha 0.05) to detect a 26% absolute reduction in 21-day mortality or ARDS (allowing 17% dropout) assuming event rate of 29% in the control group
11/
Duration of follow-up: up to 30 days after randomization
Loss to follow-up: 1/41 patient in the control group, 0/86 patients in the triple therapy group (of whom 52 received IFN; 34 did not)
Duration of follow-up: up to 30 days after randomization
Loss to follow-up: 1/41 patient in the control group, 0/86 patients in the triple therapy group (of whom 52 received IFN; 34 did not)
12/
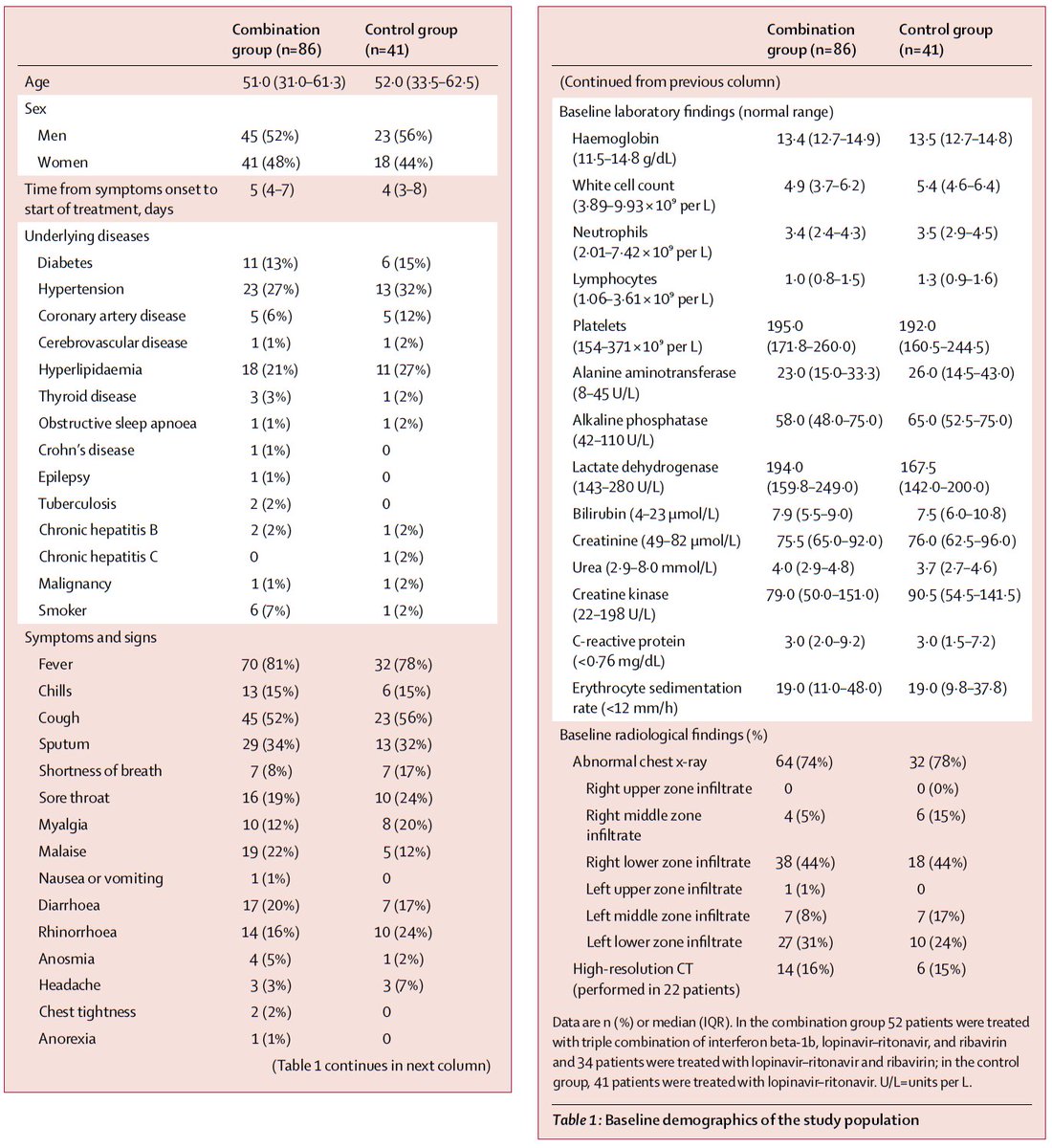
Results: Table 1:
Median age = 52, 54% male
Median time from Sx to admit: 5 [IQR 3-7] days, ~ to time from Sx to Tx in both groups.
In both groups: fever in ~80%, dry cough in ~50%, infiltrates on CXR in ~75%.
Imbalances: more HTN, CAD, and dyspnea in the control group
Results: Table 1:
Median age = 52, 54% male
Median time from Sx to admit: 5 [IQR 3-7] days, ~ to time from Sx to Tx in both groups.
In both groups: fever in ~80%, dry cough in ~50%, infiltrates on CXR in ~75%.
Imbalances: more HTN, CAD, and dyspnea in the control group
13/
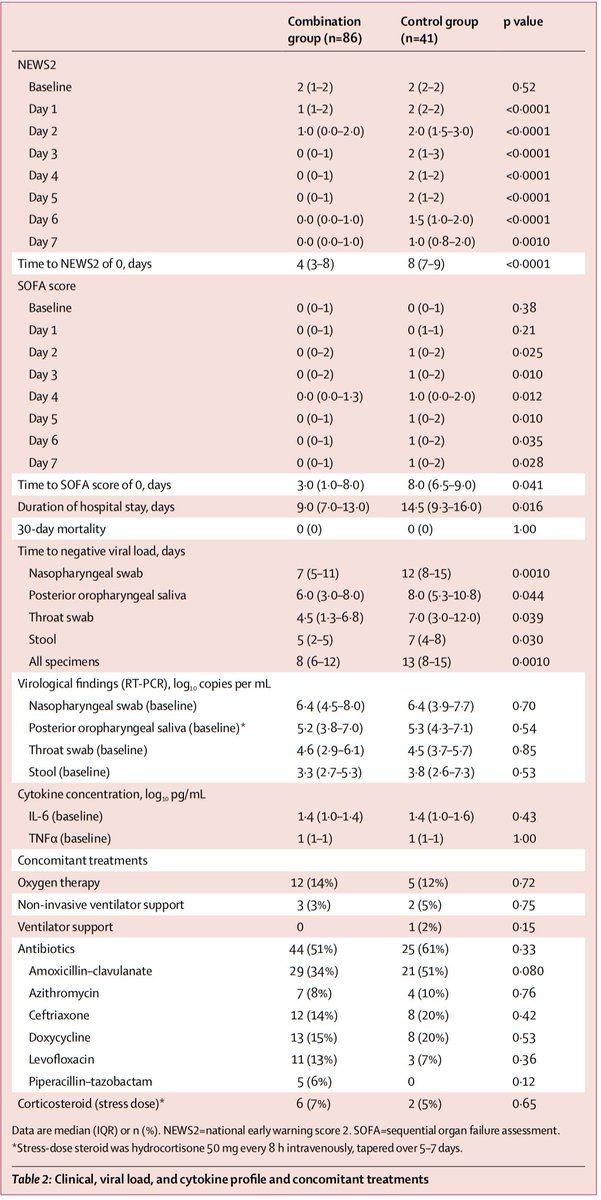
Table 2:
At baseline (triple therapy vs control):
NEWS2: 2 vs 2
SOFA: 0 vs 0
log NP viral load: 6.4 vs 6.4
Any O2 requirement: 14% vs 12% (mostly NC; <5% of pts required NIV, only 1 pt was intubated)
Primary outcome: time to negative NP swab: 7 vs 12 days (p=0.0010)
Table 2:
At baseline (triple therapy vs control):
NEWS2: 2 vs 2
SOFA: 0 vs 0
log NP viral load: 6.4 vs 6.4
Any O2 requirement: 14% vs 12% (mostly NC; <5% of pts required NIV, only 1 pt was intubated)
Primary outcome: time to negative NP swab: 7 vs 12 days (p=0.0010)
14/
Secondary outcomes (triple therapy vs control):
Time to NEWS2=0: 4 vs 8 days (p<0.0001)
LOS: 9 vs 14.5 days (p=0.016)
30-day mortality: 0 vs 0
No mutations in the nsp5 gene (which antivirals could select for) were detected.
Secondary outcomes (triple therapy vs control):
Time to NEWS2=0: 4 vs 8 days (p<0.0001)
LOS: 9 vs 14.5 days (p=0.016)
30-day mortality: 0 vs 0
No mutations in the nsp5 gene (which antivirals could select for) were detected.
15/
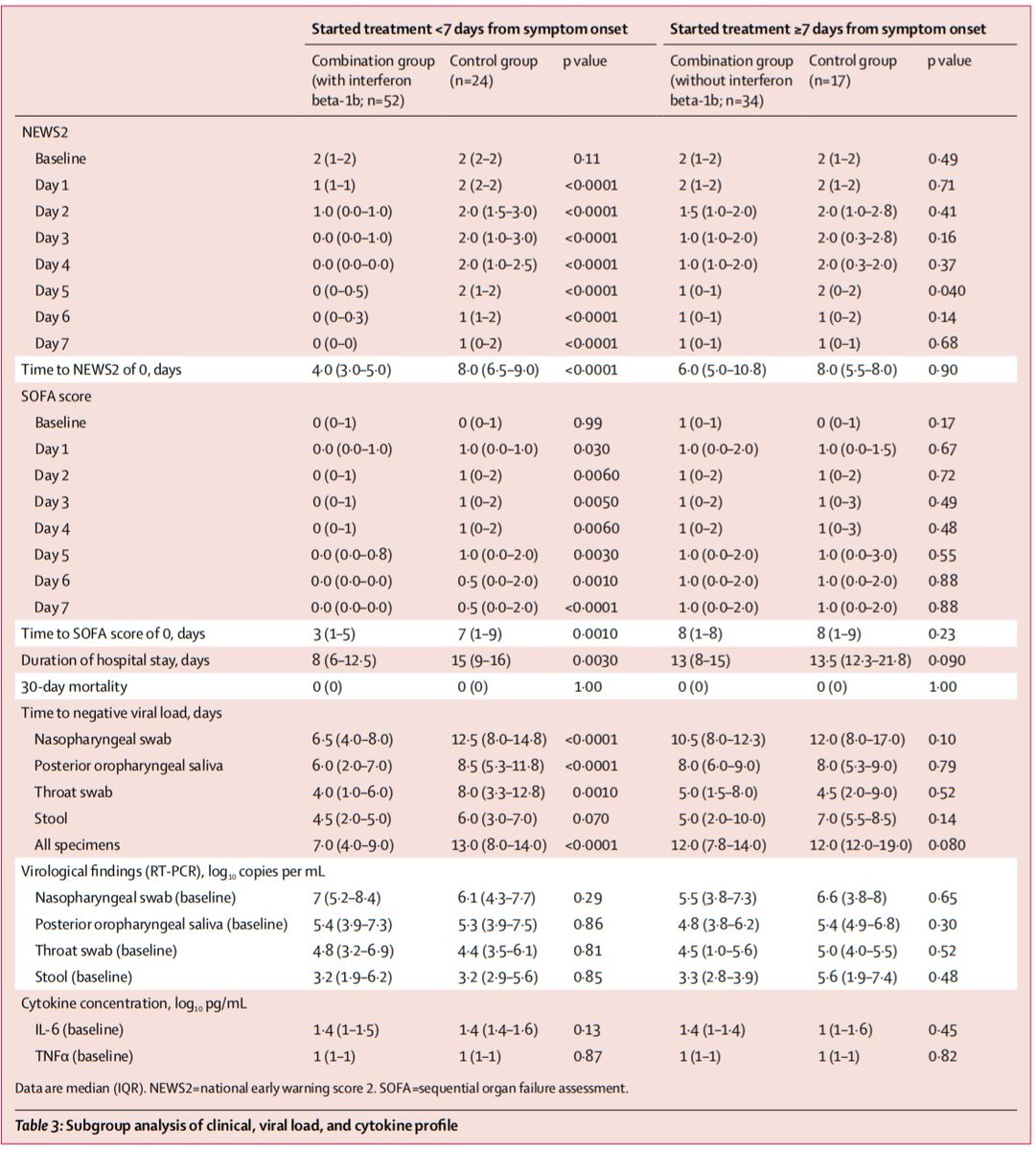
Table 3:
In the subgroup of 52 pts who actually received IFN (Tx <7d of Sx onset) vs 24 controls:
Time to negative NP swab: 6.5 vs 12.5 days (p<0.0001)
This difference did not reach statistical significance among pts who did not receive IFN (Tx started =>7d of Sx onset)
Table 3:
In the subgroup of 52 pts who actually received IFN (Tx <7d of Sx onset) vs 24 controls:
Time to negative NP swab: 6.5 vs 12.5 days (p<0.0001)
This difference did not reach statistical significance among pts who did not receive IFN (Tx started =>7d of Sx onset)
16/
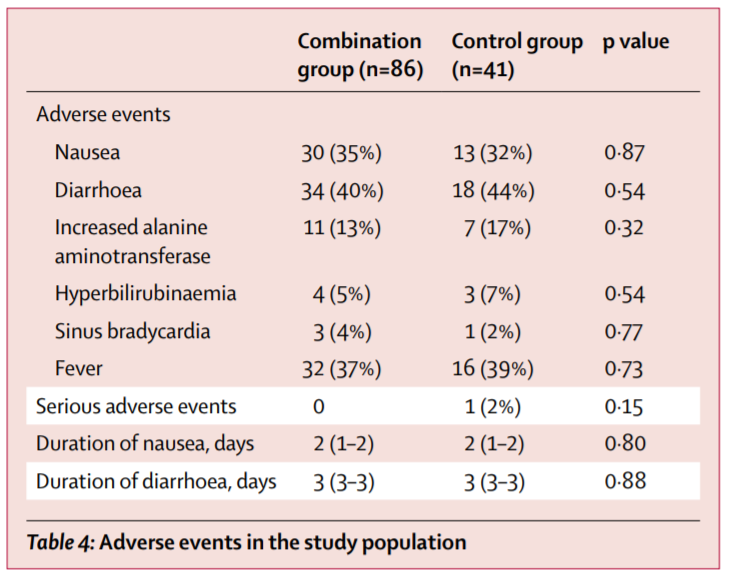
Table 4:
Adverse events occurred in ~50% of patients in both groups.
The most common were diarrhea (41%), fever (38%), and nausea (34%); with no differences between patients receiving triple therapy or LPV/r alone.
Table 4:
Adverse events occurred in ~50% of patients in both groups.
The most common were diarrhea (41%), fever (38%), and nausea (34%); with no differences between patients receiving triple therapy or LPV/r alone.
17/
Author’s conclusions: Added to usual care, triple therapy with LPV/r + RBV +/- IFN was associated with a 5 day reduction in time to negative NP swab, compared with LPV/r alone. This effect was driven by patients receiving IFN (those with Tx <7d of Sx onset).
Author’s conclusions: Added to usual care, triple therapy with LPV/r + RBV +/- IFN was associated with a 5 day reduction in time to negative NP swab, compared with LPV/r alone. This effect was driven by patients receiving IFN (those with Tx <7d of Sx onset).
18/
My appraisal: This was a positive study.
Does this mean we should use triple therapy to treat patients hospitalized with COVID19, or could chance or bias explain these findings?
Let’s take a deeper look.
My appraisal: This was a positive study.
Does this mean we should use triple therapy to treat patients hospitalized with COVID19, or could chance or bias explain these findings?
Let’s take a deeper look.
19/
It should be noted that the primary outcome in this study (time to negative NP swab) is a surrogate outcome.
What we are really interested in is whether triple therapy reduces morbidity and mortality from COVID19.
Does this study provide any clues?
It should be noted that the primary outcome in this study (time to negative NP swab) is a surrogate outcome.
What we are really interested in is whether triple therapy reduces morbidity and mortality from COVID19.
Does this study provide any clues?
20/
This study was powered to find a relatively large ↓ in death or ARDS at 21 days, which was not the primary outcome. This is highly unusual.
Fortunately, the protocol shows the primary outcome was not changed. If it were, that could raise the likelihood of a type I error.
This study was powered to find a relatively large ↓ in death or ARDS at 21 days, which was not the primary outcome. This is highly unusual.
Fortunately, the protocol shows the primary outcome was not changed. If it were, that could raise the likelihood of a type I error.
21/
Also, the study population was not very sick (only <15% on O2; no deaths). This means a very large sample size would have been needed to show any mortality difference, if one exists, because deaths were rare.
Also, the study population was not very sick (only <15% on O2; no deaths). This means a very large sample size would have been needed to show any mortality difference, if one exists, because deaths were rare.
22/
Why was this the case? The authors note that a public health ordinance in Hong Kong required ALL patients with RT-PCR confirmed SARSCoV2 to be hospitalized.
This limits the generalizability of these results to settings where hospitalized patients are much sicker.
Why was this the case? The authors note that a public health ordinance in Hong Kong required ALL patients with RT-PCR confirmed SARSCoV2 to be hospitalized.
This limits the generalizability of these results to settings where hospitalized patients are much sicker.
23/
It did appear that triple therapy was associated with faster resolution of vital sign abnormalities (as reflected by NEWS2=0), but info on resolution of actual symptoms was not provided.
Did triple therapy prevent worsening? We don’t know, but it is a testable hypothesis.
It did appear that triple therapy was associated with faster resolution of vital sign abnormalities (as reflected by NEWS2=0), but info on resolution of actual symptoms was not provided.
Did triple therapy prevent worsening? We don’t know, but it is a testable hypothesis.
24/
Also, a negative NP swab x2 was a criterion for discharge, so the ↓LOS could be reflective of reduced time to a negative swab rather than an impact on disease severity.
So, from this study, we can’t say if triple therapy reduces morbidity & mortality.
Also, a negative NP swab x2 was a criterion for discharge, so the ↓LOS could be reflective of reduced time to a negative swab rather than an impact on disease severity.
So, from this study, we can’t say if triple therapy reduces morbidity & mortality.
25/
However, though PCR positivity is not a surrogate for shedding of infectious virus, a negative PCR does reduce the post-test probability of viral shedding, and therefore, contagiousness.
This suggests these findings, if true, could have implications for ↓transmission.
However, though PCR positivity is not a surrogate for shedding of infectious virus, a negative PCR does reduce the post-test probability of viral shedding, and therefore, contagiousness.
This suggests these findings, if true, could have implications for ↓transmission.
26/
The subgroup analysis in table 3 raises the possibility that receipt of IFN was the driver of this benefit.
Also, figure 2 reveals that viral loads from multiple sites began declining sooner in the triple therapy group, suggesting the greatest benefit of IFN may be early on.
The subgroup analysis in table 3 raises the possibility that receipt of IFN was the driver of this benefit.
Also, figure 2 reveals that viral loads from multiple sites began declining sooner in the triple therapy group, suggesting the greatest benefit of IFN may be early on.

27/
Another caveat is that the duration of PCR positivity in the control group was much shorter than in other studies.
In this case series, viral shedding was detected up to 4-6 weeks after symptom onset:
academic.oup.com/cid/advance-ar…
Another caveat is that the duration of PCR positivity in the control group was much shorter than in other studies.
In this case series, viral shedding was detected up to 4-6 weeks after symptom onset:
academic.oup.com/cid/advance-ar…
28/
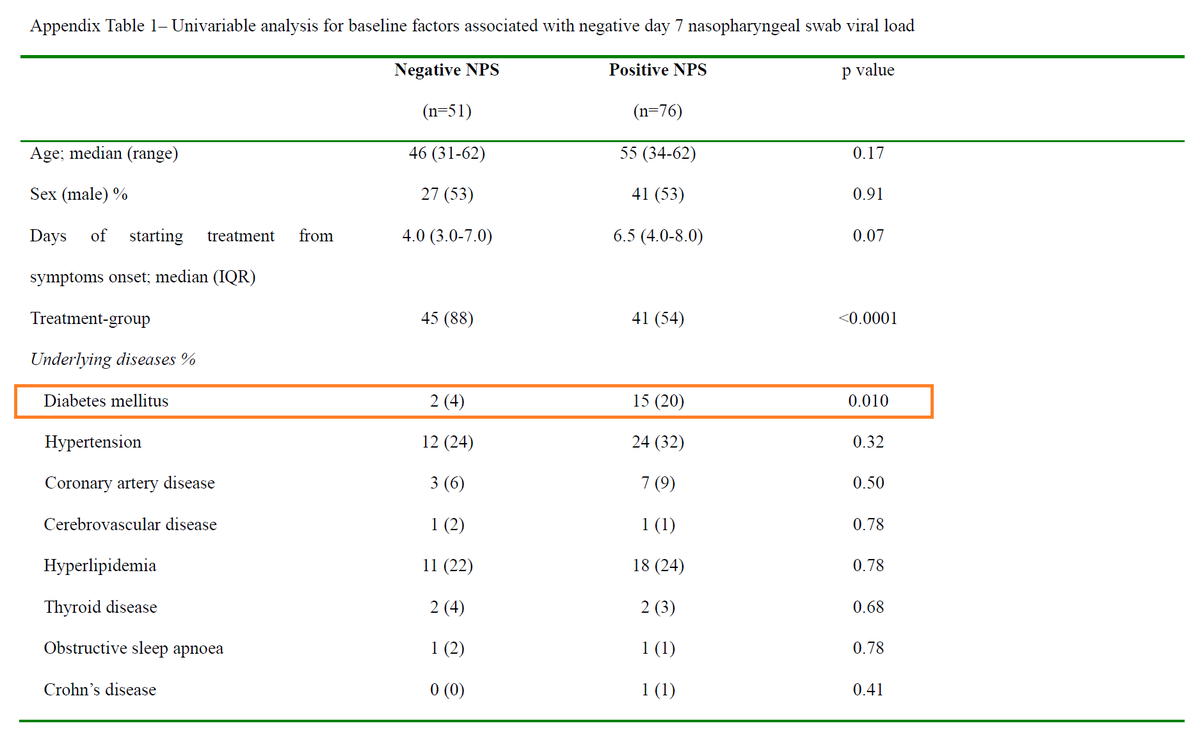
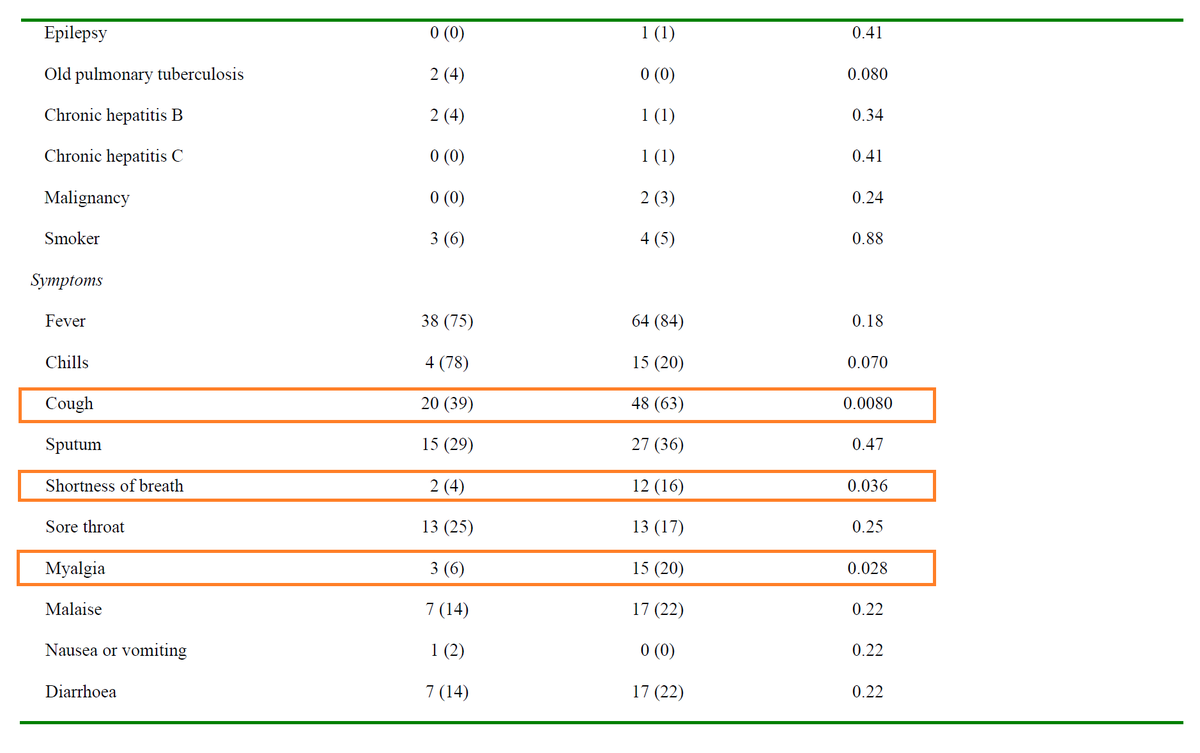
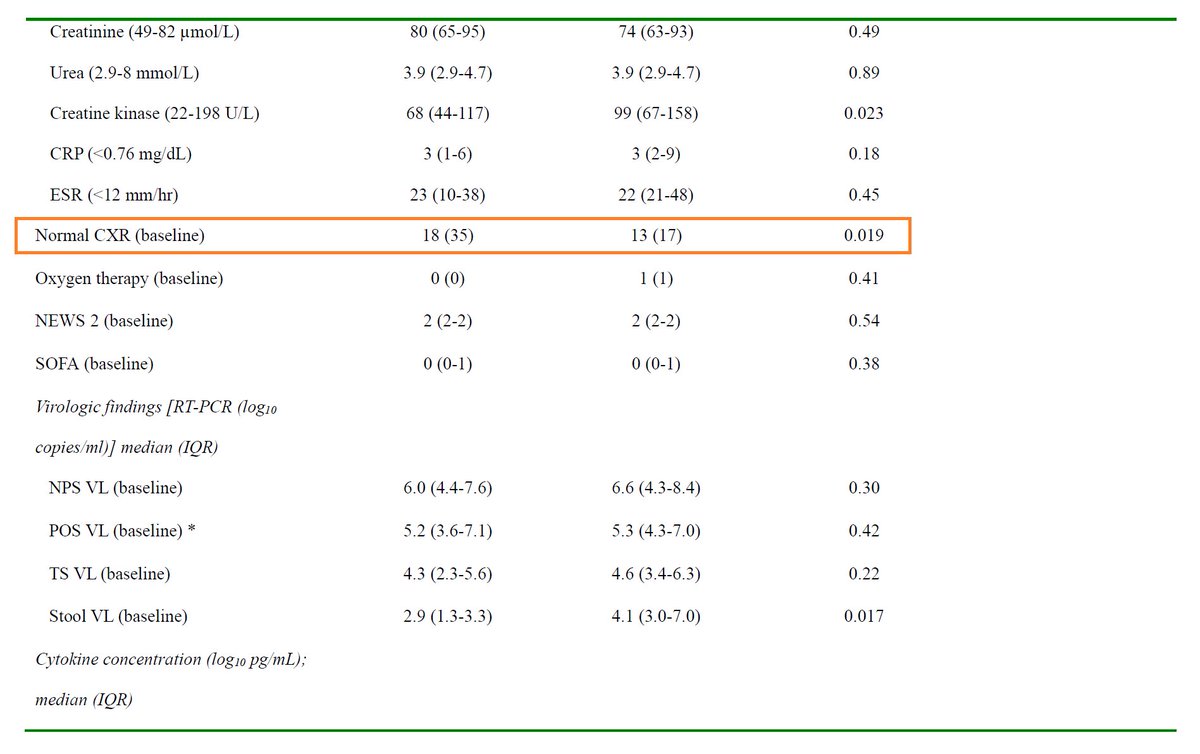
Finally, duration of viral shedding may be related to illness severity.
Data in the appendix indicate that that DM2, cough, SOB, and myaligas were all associated with having a positive NP swab on day 7, and having a normal CXR was associated with negative swab on day 7.
Finally, duration of viral shedding may be related to illness severity.
Data in the appendix indicate that that DM2, cough, SOB, and myaligas were all associated with having a positive NP swab on day 7, and having a normal CXR was associated with negative swab on day 7.
29/
To close, let’s revisit the original question:
After reading & appraising this study, when considering triple therapy as a treatment for patients with COVID19, I think the most important component is likely to be:
To close, let’s revisit the original question:
After reading & appraising this study, when considering triple therapy as a treatment for patients with COVID19, I think the most important component is likely to be:
30/
Bottom line: Among patients hospitalized with mild disease from COVID19, triple therapy was associated with reduced time to a negative NP swab; this was driven by IFN and/or Tx <7d of Sx onset. Further study is needed using clinical endpoints in sicker patients.
(End)
Bottom line: Among patients hospitalized with mild disease from COVID19, triple therapy was associated with reduced time to a negative NP swab; this was driven by IFN and/or Tx <7d of Sx onset. Further study is needed using clinical endpoints in sicker patients.
(End)