I listened to (while doing some admin) @ISPD1 webinar on dispelling #myths in #peritoneal #dialysis by the inimitable @PD_perls- really interesting content and I’ve added some of my own myths that I’ve been presented with over the years that I’ve lead the service @HeartlandsUHB
Myth #1- Previous abdominal surgery and PD are not compatible..
This is the commonest reason why patients are not offered PD
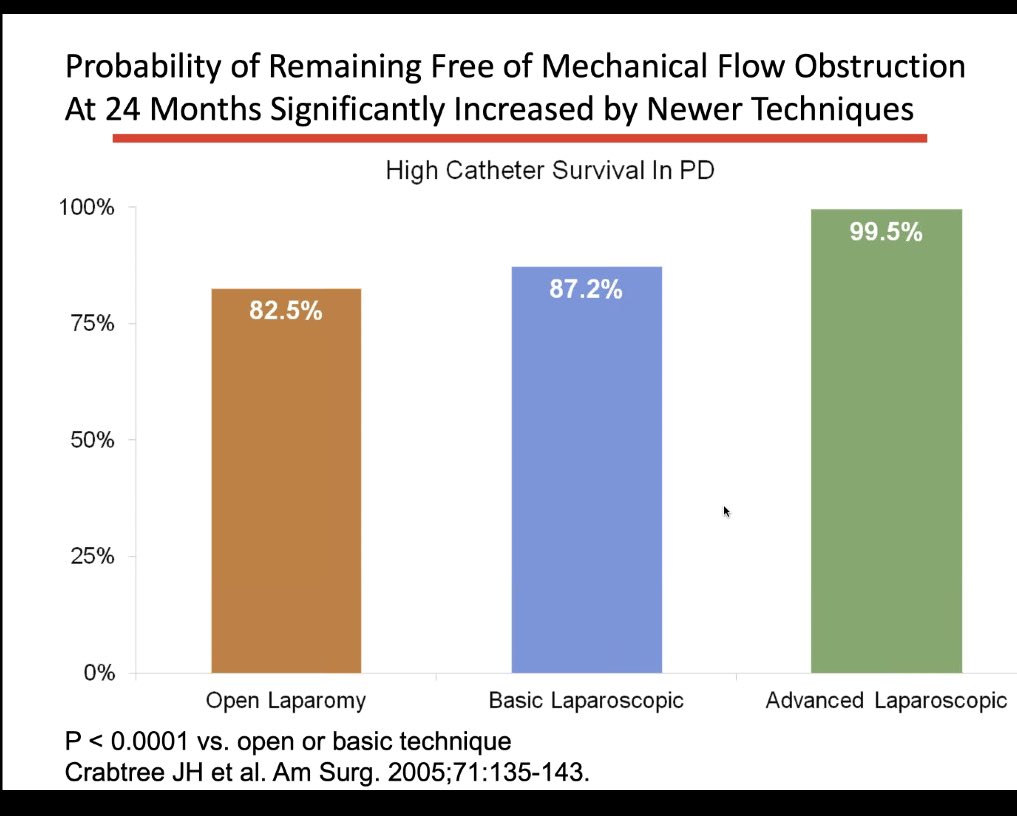
Advanced laparoscopic tube placement can do away with most issues as this slide shows:
This is the commonest reason why patients are not offered PD
Advanced laparoscopic tube placement can do away with most issues as this slide shows:




We have also done some percutaneous blind and fluoroscopy guided procedures in patients with simple scars such as a C-section; appendectomy and laparoscopic cholecystectomy and overall, not had any issues
This is a good paper pubmed.ncbi.nlm.nih.gov/19280807/ although fairly old that shows Scars on the abdomen and prior peritonitis do not predict the extent of adhesions and should not be used to judge eligibility for peritoneal dialysis
Advanced catheter placement has many advantages and gives clinicians the chance to perform adhensiolysis and an omentopexy if needed – and there is evidence that ACP leads to higher catheter survival pubmed.ncbi.nlm.nih.gov/16022013/


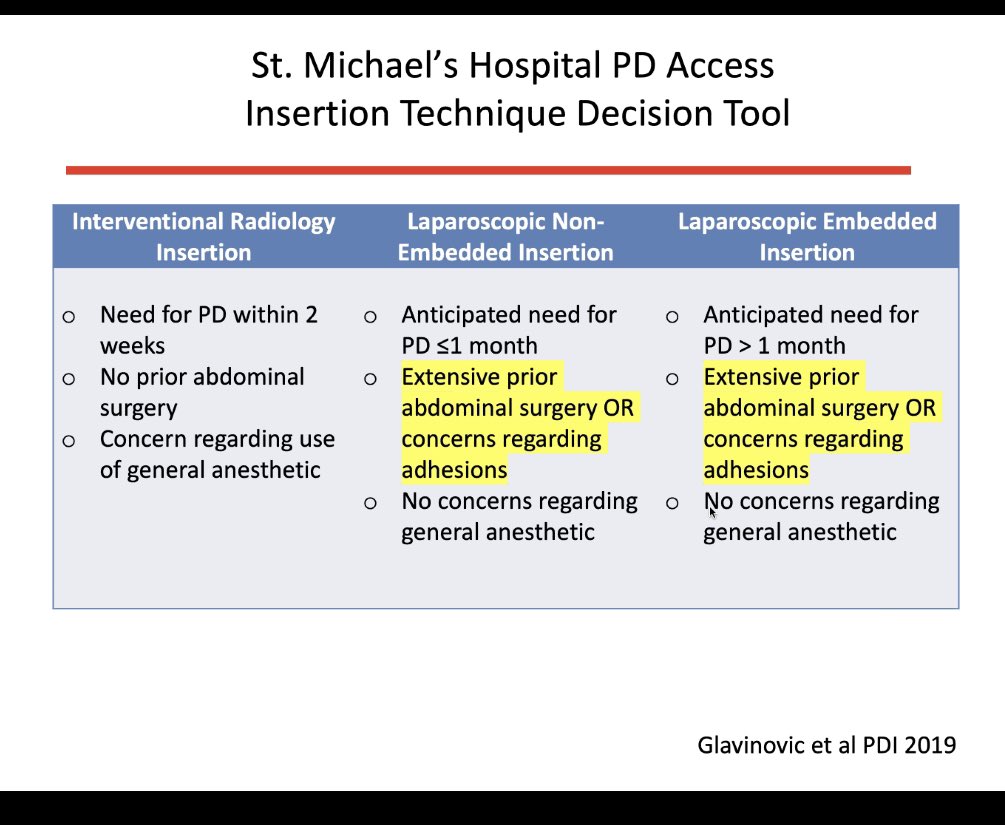
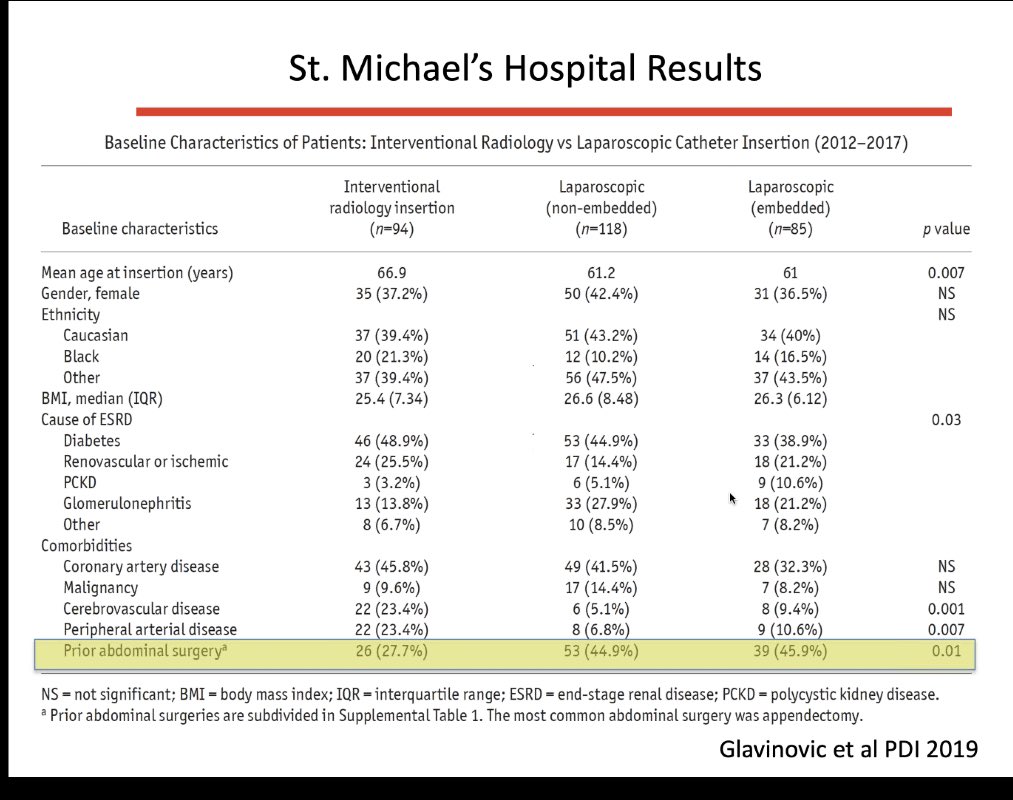
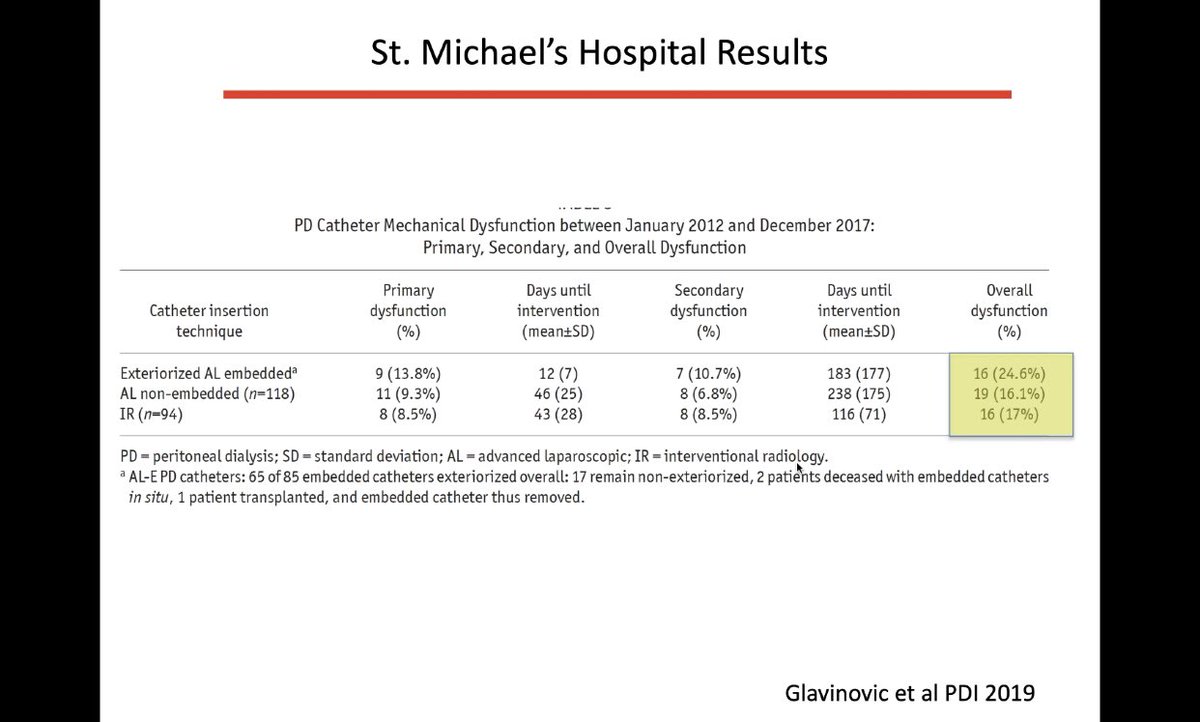
More recently a QIP showed improved outcomes following the implementation of a technique decision tool pdiconnect.com/content/early/…
Myth #2- stomas and PD are a match made in hell- I have no personal experience of this and TBH I haven’t been brave enough to attempt this nor have I ever found a patient that would IMO benefit from PD with a stoma in place over HD..but it is possible – after all its done in kids

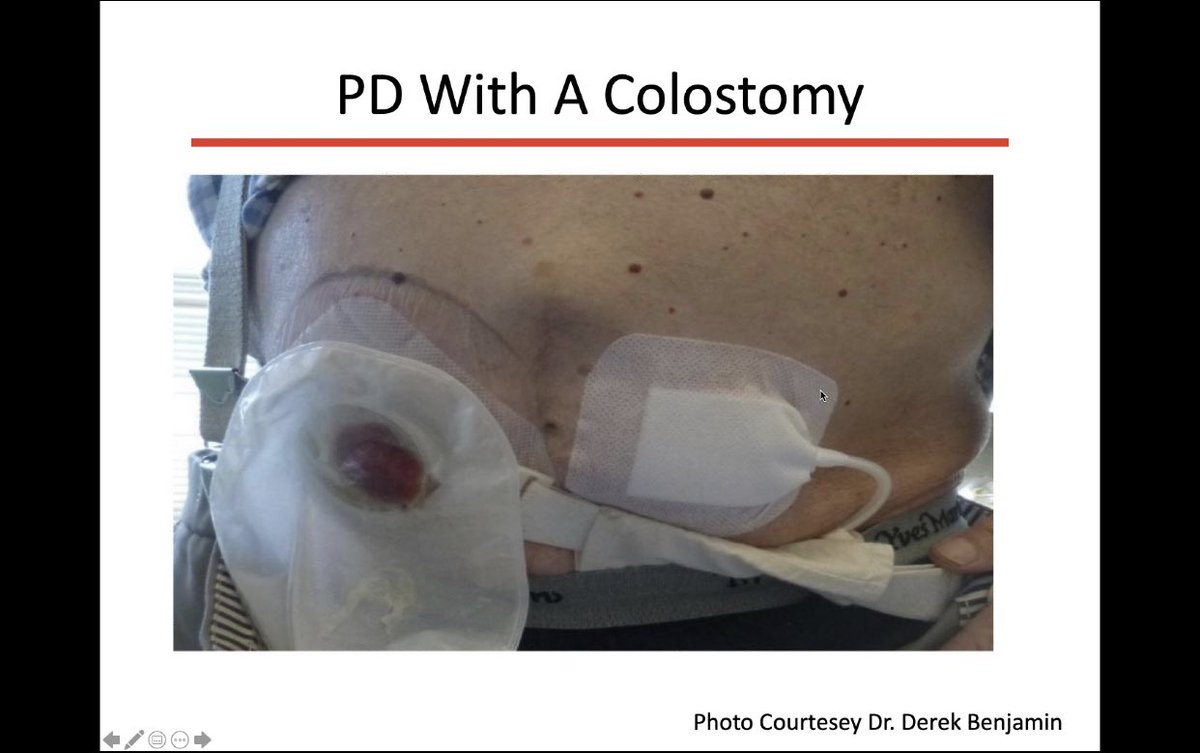
The trick apparently is – a distant exit site – again not difficult if you know how or if your access surgeon does this – I once looked after a patient from Canada who was on holiday with us who had an ostomy and had an exit
site near the sternum and I that was the first time I had seen one so clearly its not something we do much in the UK- this is a really old reference pubmed.ncbi.nlm.nih.gov/1586692/- and it showed that that PD in the presence of an ostomy was associated with reasonable outcomes
Myth #3- Obesity and PD = poor outcomes – in fact after abdominal surgery this is the second common reason for patients not being offered PD


A few misconceptions about this –
1)The shape of the patient and pattern of obesity is more important than the BMI itself – an apple and a pear can both have the same BMI – so don’t look at weight per se – look at the patient instead ..
1)The shape of the patient and pattern of obesity is more important than the BMI itself – an apple and a pear can both have the same BMI – so don’t look at weight per se – look at the patient instead ..

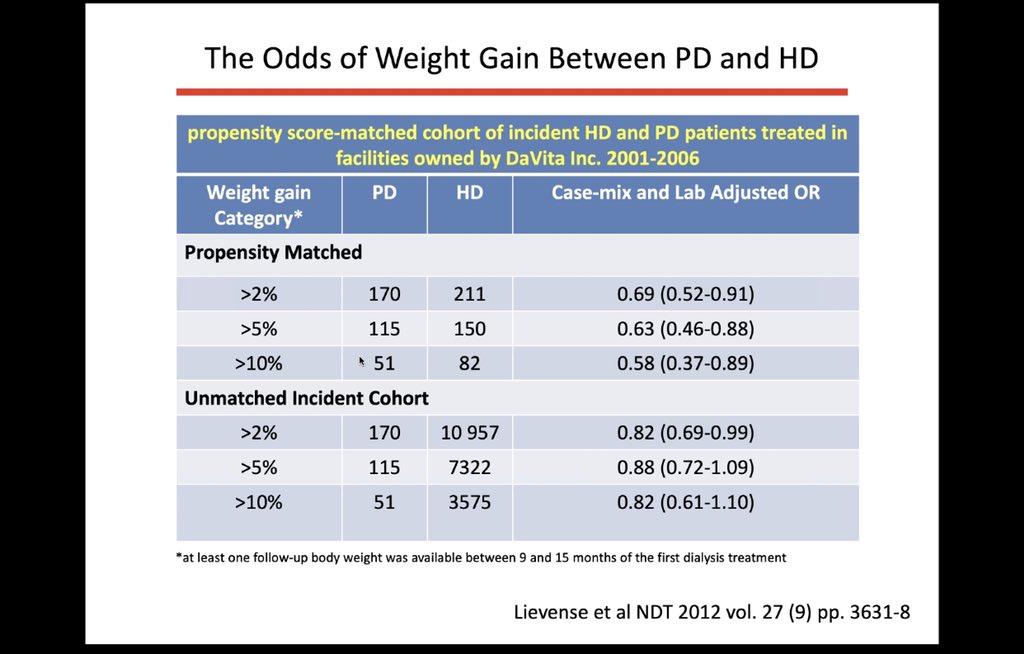
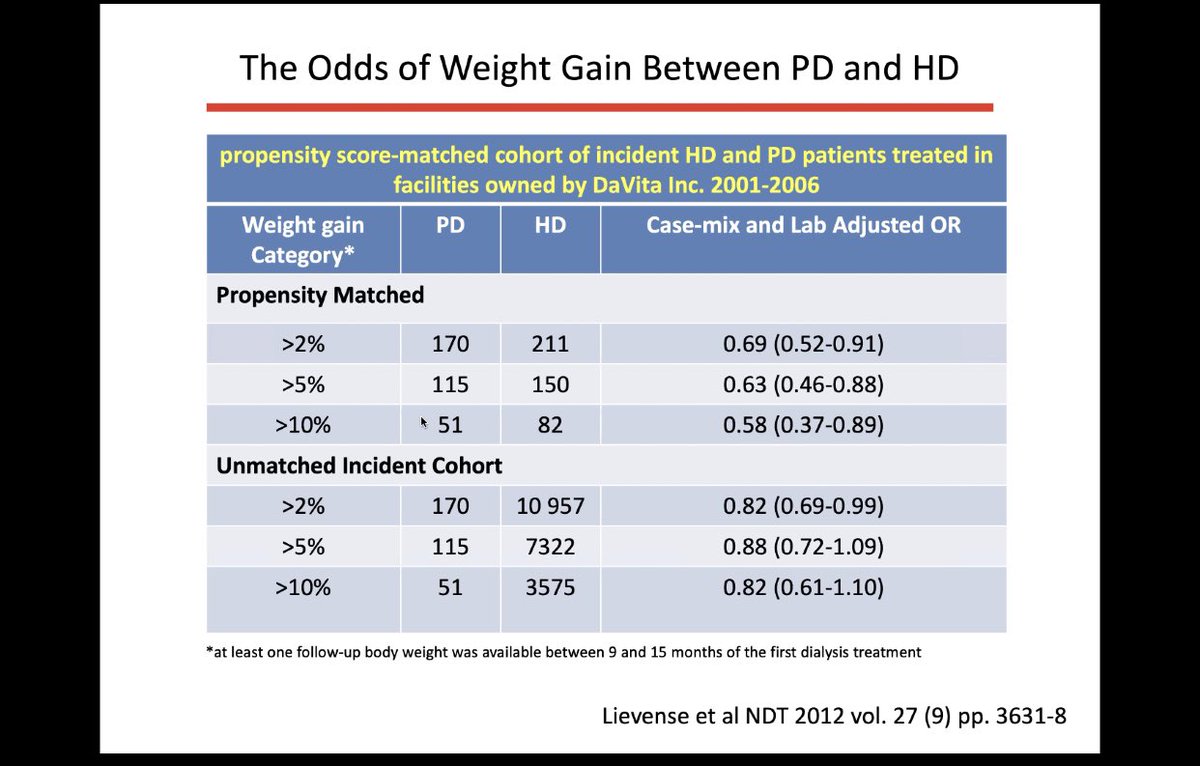
2)PD in overweight patients makes them gain more weight – patients gain more weight on HD than they do on PD actually ⬇️

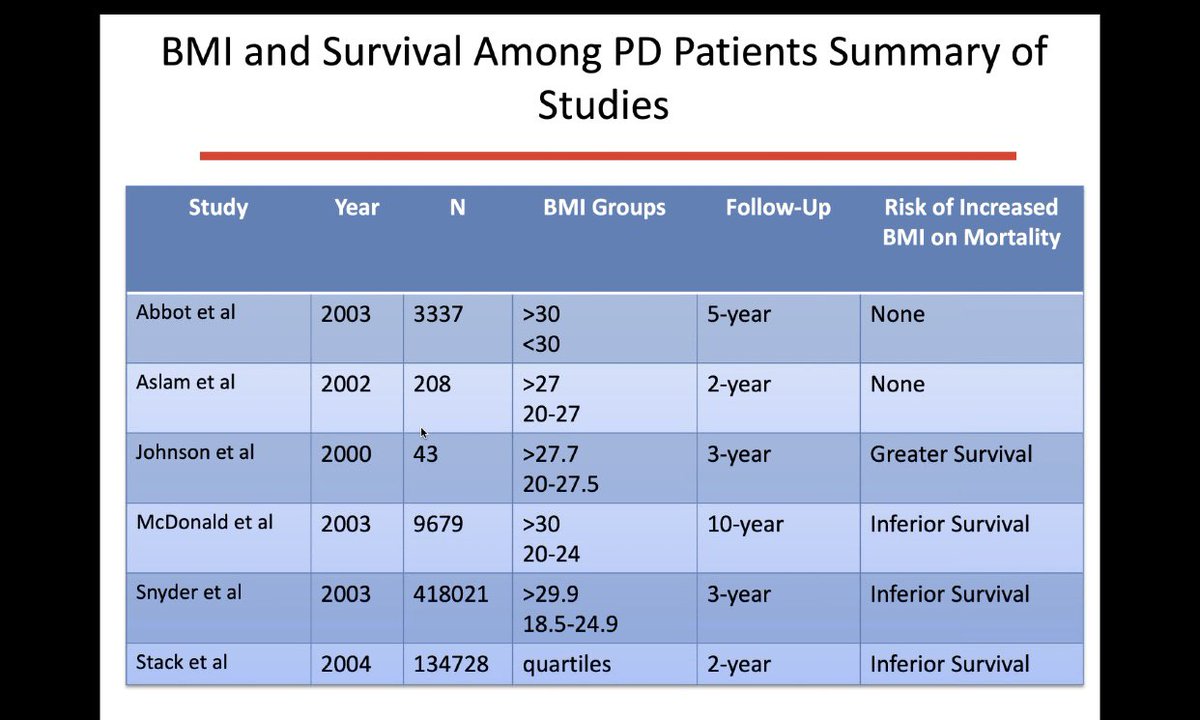
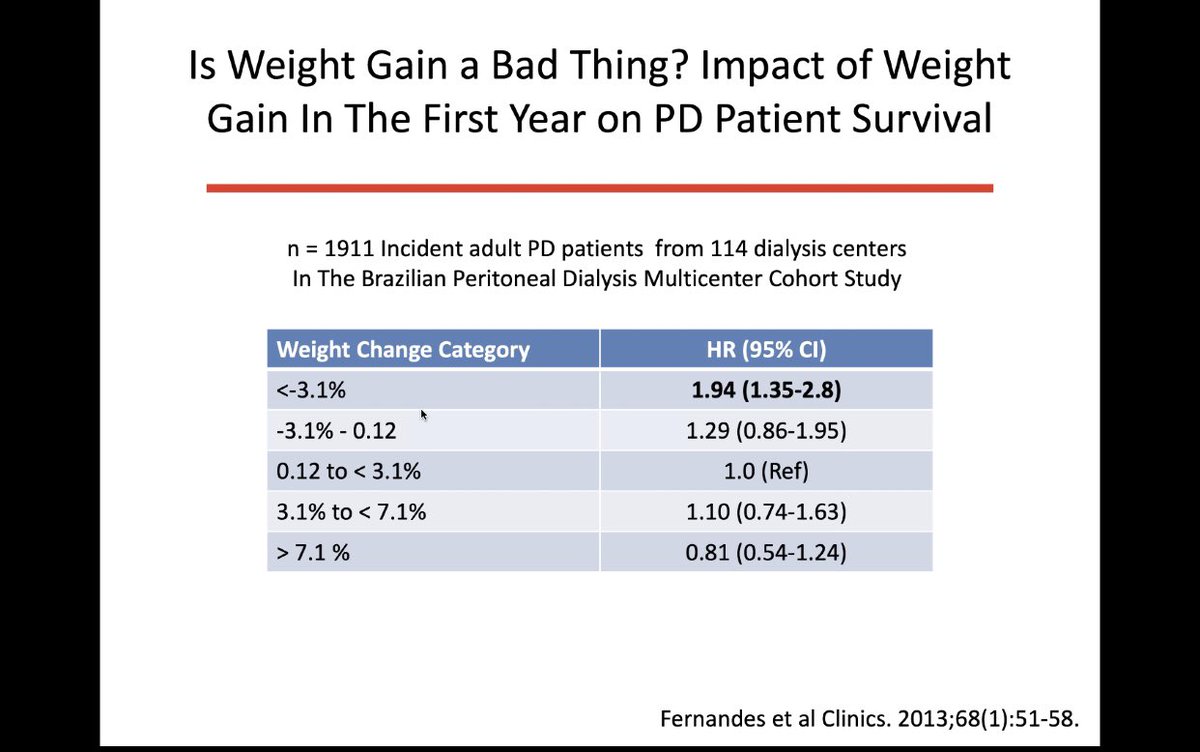
3) BMI on dialysis is linked to survival so putting on weight is not all bad if you are a dialysis patient...


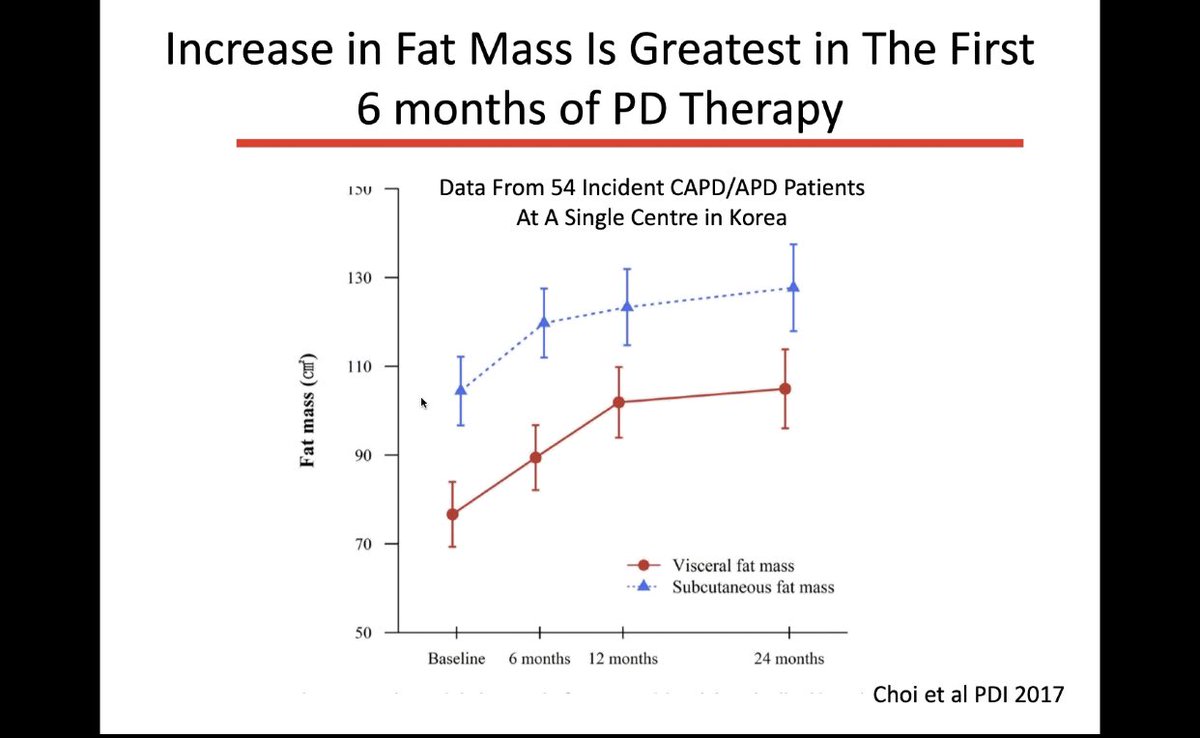
4) one can usually predict who will gain weight following initiation of PD – and it isn’t always the diabetic patients – and there is a reason why PD patients gain weight –
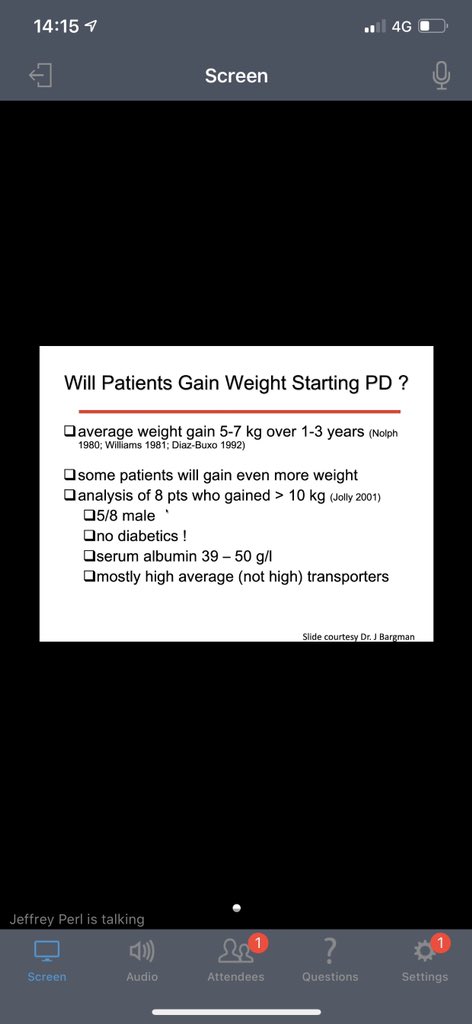

– and it is an increase in fat mass that is the greatest in the first 6 months of treatment scielo.br/scielo.php?scr… showed that obesity & a positive body weight variation during the first year of peritoneal dialysis therapy did not increase mortality in incident dialysis patients
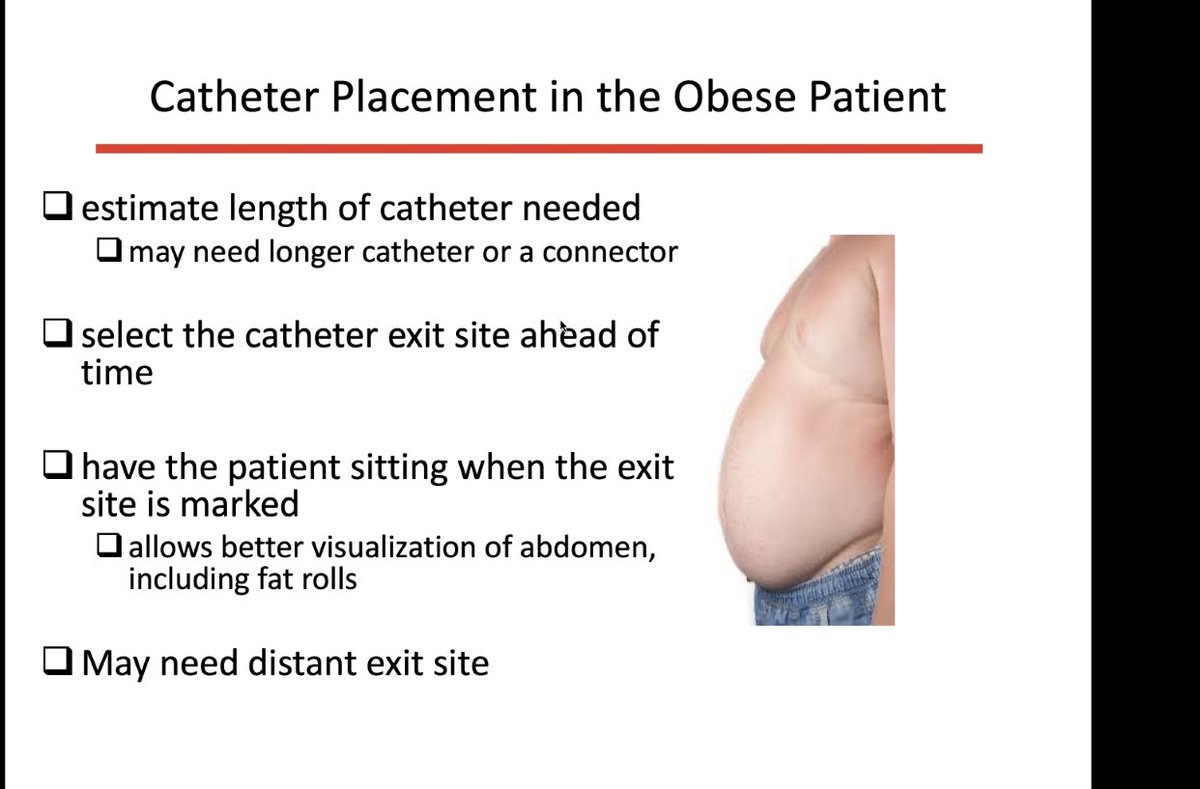
5) high BMI leads to an increased incidence of peritonitis – possibly with coagulase negative staph organisms – this is a risk but can be mitigated and shouldn’t be a reason not to offer PD – ACP helps




– get the PD nurse to mark the exit site whilst patient is standing and help the surgeon to chose best site when catheter exits …





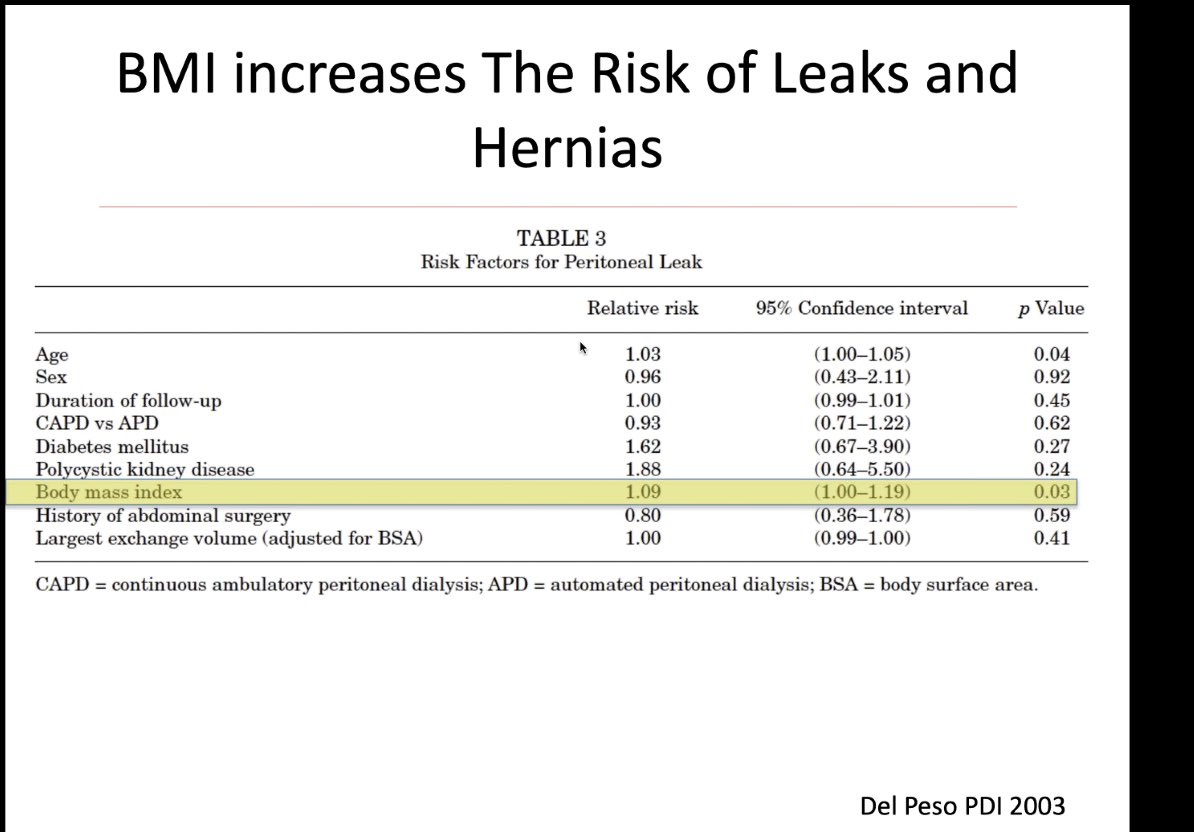
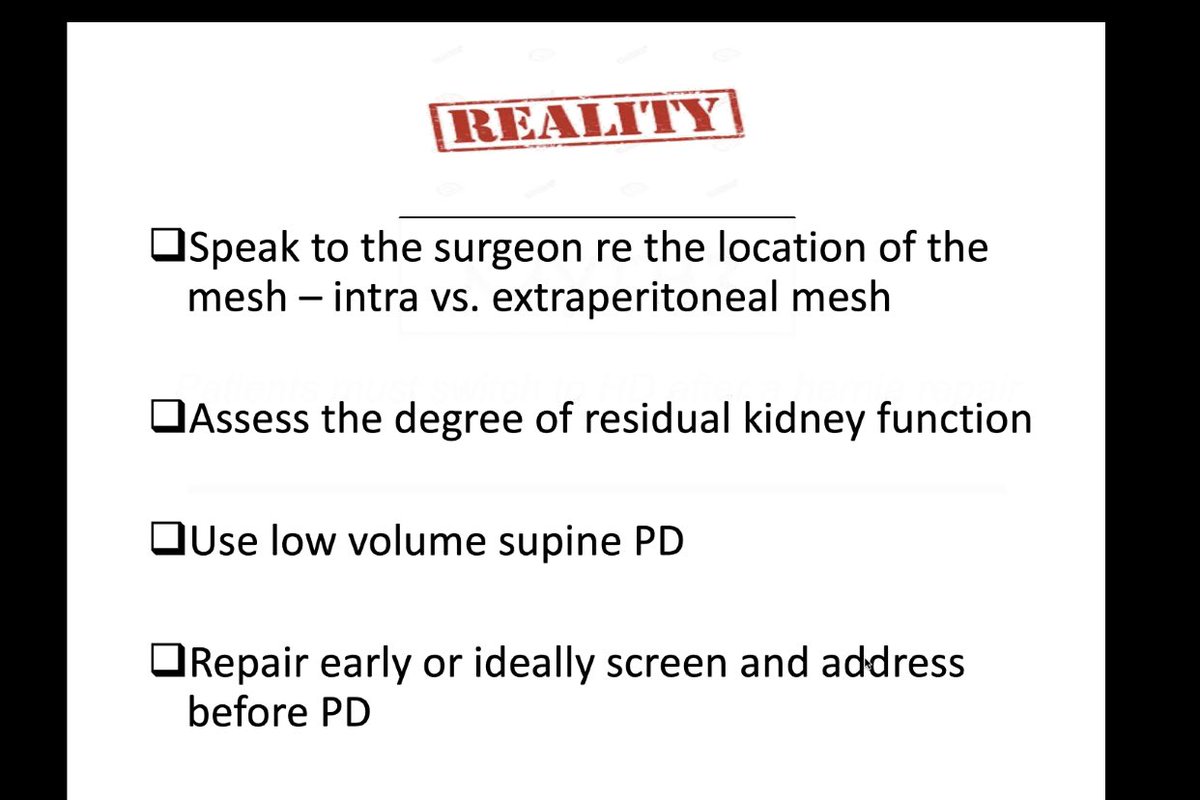
6) High BMI and non-infectious complications of PD - Advanced age, polycystic kidney disease, and high body mass index are independent risk factors for their development. Automated PD with low daytime fill volume should be

Automated PD with low daytime fill volume should be considered in all patients at risk for hernias and/or leaks citeseerx.ist.psu.edu/viewdoc/downlo…
And there are various strategies to minimize the risks of leaks and hernias



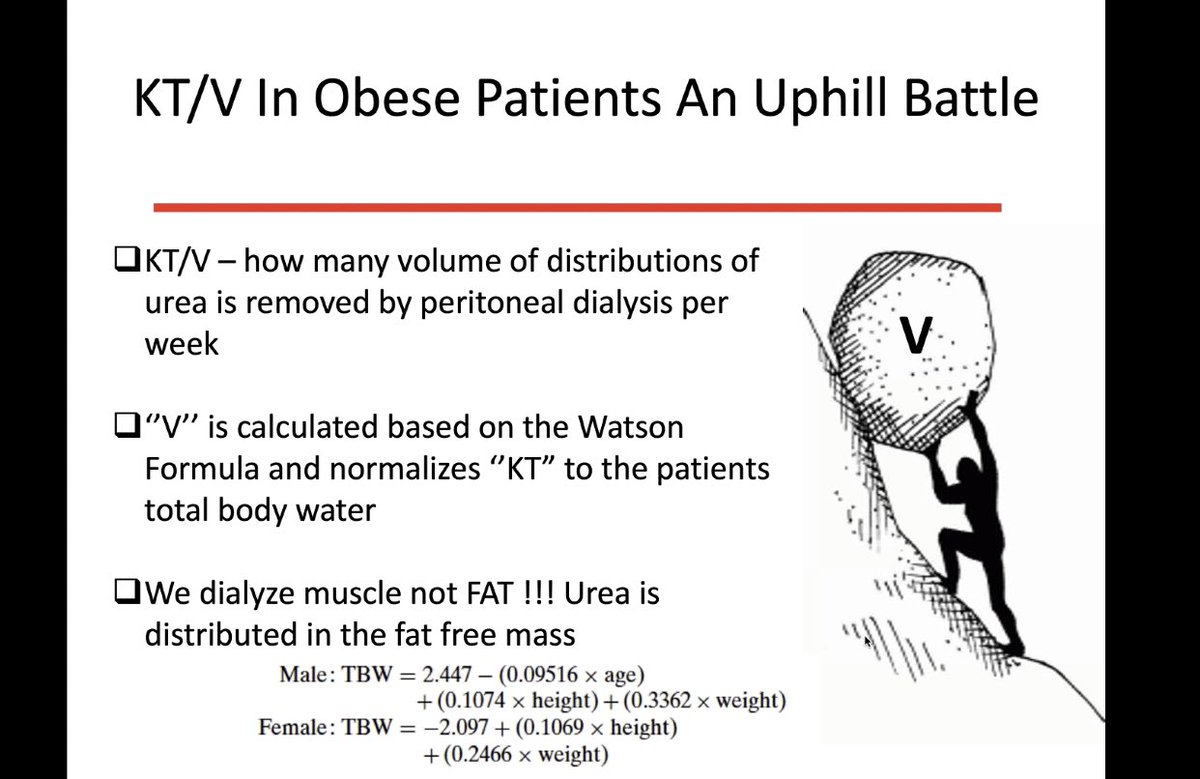
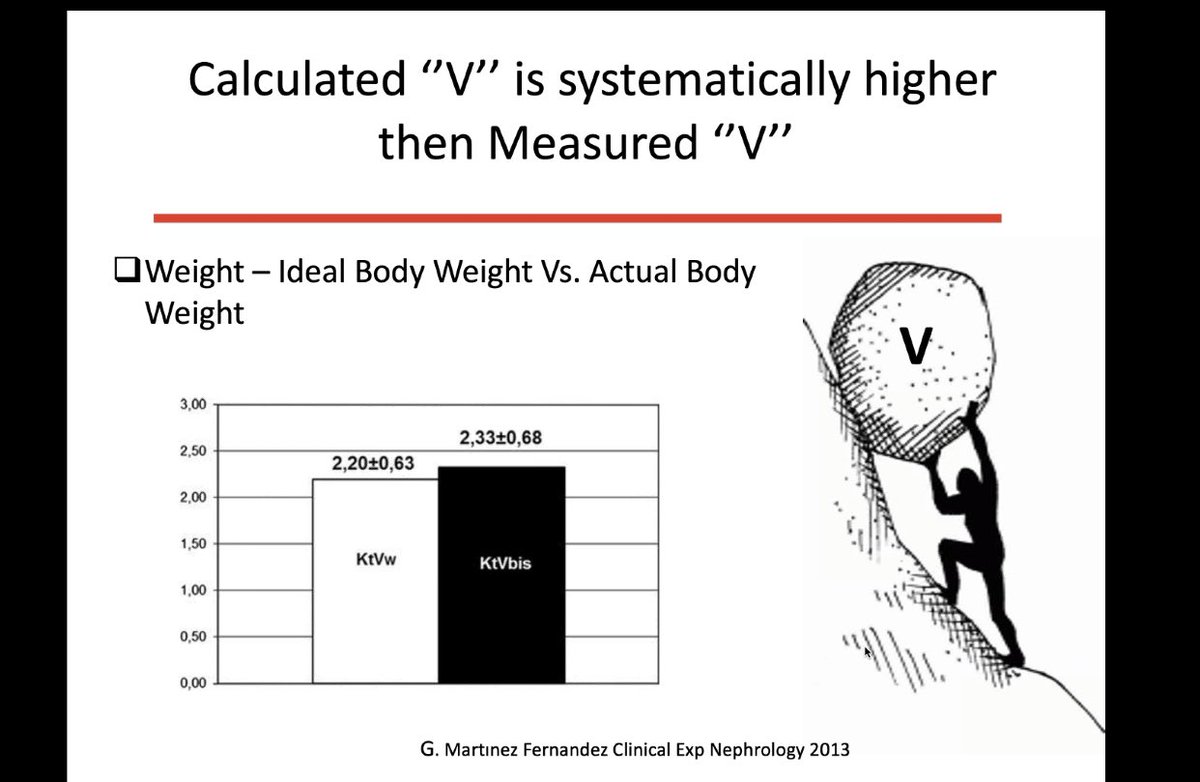
7) what about adequacy in those with a High BMI?- @ISPD1 guidelines have advocated a move away from measuring adequacy in numbers and KT/V in obesity is a minefield but again there are various ways to ensure larger patients receive adequate PD



Myth #4 Move to HD after a hernia repair or abdominal surgery is a must
Depends – personally I always try and continue with PD post-surgery where it’s safe to do so ..
Depends – personally I always try and continue with PD post-surgery where it’s safe to do so ..
much more convenient for the patient and most will have some RRF to enable the deviation from dialysis for 24 hours but where one cant then low volume dwells and a dry day are the way forward – if a patient is o APD and the umbilical hernia small then repair not always indicated
; in the webinar @PD_Perls mentioned some surgeries he would never advocate PD after – I don’t agree with the entire list as I do think local surgical experience is what should drive the decision to continue with PD or not post op..
Myth #5 Return to PD after catheter removal for peritonitis is not recommended
Depends on the organism – with fungal probably not – with Tb – no one knows – with another organism – it should not be discouraged
Depends on the organism – with fungal probably not – with Tb – no one knows – with another organism – it should not be discouraged








Over the years I have heard various other myths as to why patients should not have PD
• Glucose is not good for the PD membrane
• What is the point – will end up on HD anyway
• They have kids
• They have a dog /cat/snake etc...
• Glucose is not good for the PD membrane
• What is the point – will end up on HD anyway
• They have kids
• They have a dog /cat/snake etc...
• They will surgery planned
• They have an LRD in the pipeline
• They may get ESP...
• They have an LRD in the pipeline
• They may get ESP...
Whist I firmly believe in PD as a first line RRT modality in most patients – I think patient choice should not be ignored – as a renal community though we owe it to our patients to dispel the common myths that exist and not allow folklore to dictate what we do...