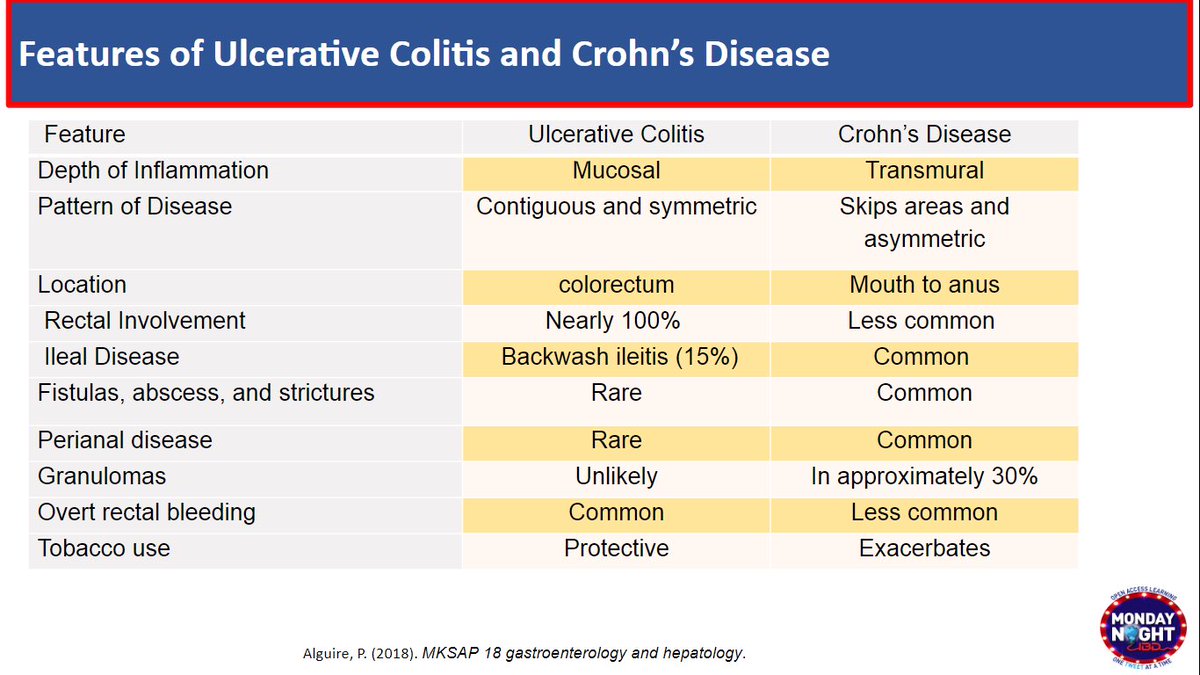
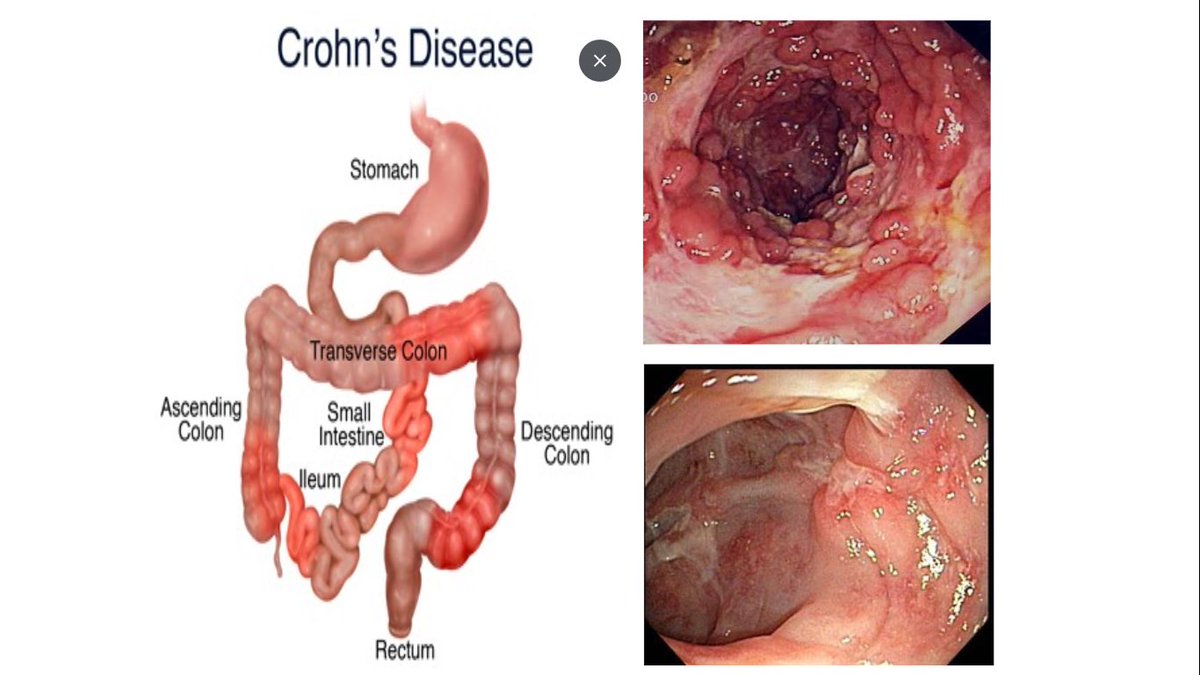
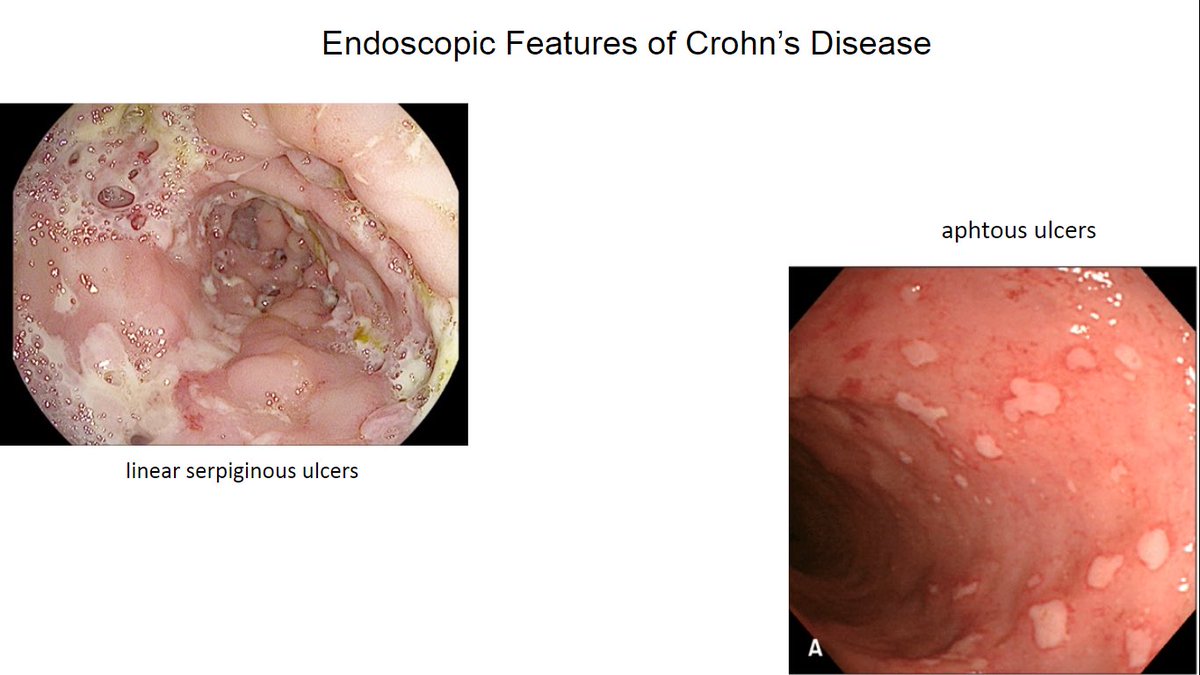
@MondayNightIBD @SobiaMujtabaMD @JasonHouMD @DCharabaty 1/ 65 y/o M new dx #Crohns ileitis after he presented w abdo pain,diarrhea, wt loss, anemia. CLN: deep linear ulcers in TI. He has an active lifestyle,stable CAD. Symptoms recur when prednisone<15 mg. What is the LEAST effective strategy to keep this pt in remission? #Back2Basics
@MondayNightIBD @SobiaMujtabaMD @JasonHouMD @DCharabaty 2/ #IBD is not only a disease of the young !
♦️ Typical dx age 20-39, w a second smaller peak >50
♦️ Recently ⬆️ prevalence in elderly> age 60, due to:
🔺Aging of adults w #IBD
🔺⬆️elderly onset IBD > age 60 #EOIBD:
🔹⬆️awareness & dx
🔹Environment/ microbiome changes
♦️ Typical dx age 20-39, w a second smaller peak >50
♦️ Recently ⬆️ prevalence in elderly> age 60, due to:
🔺Aging of adults w #IBD
🔺⬆️elderly onset IBD > age 60 #EOIBD:
🔹⬆️awareness & dx
🔹Environment/ microbiome changes
@MondayNightIBD @SobiaMujtabaMD @JasonHouMD @DCharabaty 3/ Clinical Features of #IBD in #elderly 🔎?
📌Milder disease course, Fewer #Crohns complications, but
⬆️rates of hospitalizations
⬆️rates of colectomy in EO UC
📌❓Due to disease severity vs poor #IBD control d/t underuse of effective Rx
📌Milder disease course, Fewer #Crohns complications, but
⬆️rates of hospitalizations
⬆️rates of colectomy in EO UC
📌❓Due to disease severity vs poor #IBD control d/t underuse of effective Rx
@MondayNightIBD @SobiaMujtabaMD @JasonHouMD @DCharabaty 4/ Real life data of #IBD Rx in elderly show :
⚠️Overuse of 5ASA even in #Crohns disease
⚠️Up to ⅓ pts kept on chronic corticosteroids
⚠️Limited use of thiopurines or biologic (<6%)
⚠️CS are NOT a maintenance strategy & SE ⬆️⬆️in elderly
link.springer.com/article/10.100…
⚠️Overuse of 5ASA even in #Crohns disease
⚠️Up to ⅓ pts kept on chronic corticosteroids
⚠️Limited use of thiopurines or biologic (<6%)
⚠️CS are NOT a maintenance strategy & SE ⬆️⬆️in elderly
link.springer.com/article/10.100…
@MondayNightIBD @SobiaMujtabaMD @JasonHouMD @DCharabaty 5/⬆️Disease burden in elderly; for eg:
⬇️cognitive & functional status → ⬇️anal sphincer tone,⬇️mobility →incontinence,distress, risk of fall from diarrhea
⬇️social support →limit access to scope, infusion..
@DCharabaty @joshsteinbergMD @yaransarkis
doi.org/10.1007/s11938…
⬇️cognitive & functional status → ⬇️anal sphincer tone,⬇️mobility →incontinence,distress, risk of fall from diarrhea
⬇️social support →limit access to scope, infusion..
@DCharabaty @joshsteinbergMD @yaransarkis
doi.org/10.1007/s11938…
@MondayNightIBD @SobiaMujtabaMD @JasonHouMD @DCharabaty @joshsteinbergMD @yaransarkis 6/ Potential barriers to Rx in #EOIBD :
Co-morbidities
⬆️risk of (opportunistic) infection, mainly if frail vs fit pt
❗️Poly💊
❗️Overall frailty
❗️Older pts excluded from biologics RCT👉🏽limited data on efficacy/safety in elderly
Co-morbidities
⬆️risk of (opportunistic) infection, mainly if frail vs fit pt
❗️Poly💊
❗️Overall frailty
❗️Older pts excluded from biologics RCT👉🏽limited data on efficacy/safety in elderly
@MondayNightIBD @SobiaMujtabaMD @JasonHouMD @DCharabaty @joshsteinbergMD @yaransarkis 7/ Rx options for #IBD in #elderly
#5ASA most prescribed
👉🏽Perceived as safe,but 🛎️
📍Many & large💊in pts w often difficulty swallowing
📍Difficulty using topical form
👉🏽non-adherence
📍⬆️risk of interstitial nephritis in elderly w comorbidities
📍Indicated only in mild UC
#5ASA most prescribed
👉🏽Perceived as safe,but 🛎️
📍Many & large💊in pts w often difficulty swallowing
📍Difficulty using topical form
👉🏽non-adherence
📍⬆️risk of interstitial nephritis in elderly w comorbidities
📍Indicated only in mild UC
@MondayNightIBD @SobiaMujtabaMD @JasonHouMD @DCharabaty @joshsteinbergMD @yaransarkis 8/ Rx options for #IBD in #elderly
#Thiopurines (AZA/MP)/ IMM
⬆️ Risk of lymphoma, specifically in men > age 50
⬆️ Risk of NMSC
📍Need frequent lab monitoring, that can be challenging in elderly
#Thiopurines (AZA/MP)/ IMM
⬆️ Risk of lymphoma, specifically in men > age 50
⬆️ Risk of NMSC
📍Need frequent lab monitoring, that can be challenging in elderly
@MondayNightIBD @SobiaMujtabaMD @JasonHouMD @DCharabaty @joshsteinbergMD @yaransarkis 9/ How about biologics for #IBD in #elderly ?
❇️ #TNFi ❇️
🔰⬆️ risk of URI/pneumonia, opportunistic infxn
🔰Avoid use w IMM/CS
🚫diff in efficacy vs young on TNFi
⛔️ Absolute/relative CI: Uncontrolled CHF, neurologic disease, h/o lymphoma, CA..
doi.org/10.1016/j.cgh.…
❇️ #TNFi ❇️
🔰⬆️ risk of URI/pneumonia, opportunistic infxn
🔰Avoid use w IMM/CS
🚫diff in efficacy vs young on TNFi
⛔️ Absolute/relative CI: Uncontrolled CHF, neurologic disease, h/o lymphoma, CA..
doi.org/10.1016/j.cgh.…
@MondayNightIBD @SobiaMujtabaMD @JasonHouMD @DCharabaty @joshsteinbergMD @yaransarkis 10 / 🌀VDZ🌀 in #elderly
🔹Perceived as safer option because it’s gut-specific
⬆️ Risk of (non serious) infection elderly vs young on VDZ
🔹Similar efficacy vs adult on VDZ
🔹👍 #IBD w/o EIMs, or h/o lymphoma/ CA/Skin CA
doi.org/10.1177/205064…
🔹Perceived as safer option because it’s gut-specific
⬆️ Risk of (non serious) infection elderly vs young on VDZ
🔹Similar efficacy vs adult on VDZ
🔹👍 #IBD w/o EIMs, or h/o lymphoma/ CA/Skin CA
doi.org/10.1177/205064…
@MondayNightIBD @SobiaMujtabaMD @JasonHouMD @DCharabaty @joshsteinbergMD @yaransarkis 11/ ✴️ #UST ✴️ in #elderly
🔸Good safety data in RCT
🔸 Limited data in elderly
🔸⬆️ risk of CV SEs in pts w CVD risk factors
jamanetwork.com/journals/jamad…
🔸Good safety data in RCT
🔸 Limited data in elderly
🔸⬆️ risk of CV SEs in pts w CVD risk factors
jamanetwork.com/journals/jamad…
@MondayNightIBD @SobiaMujtabaMD @JasonHouMD @DCharabaty @joshsteinbergMD @yaransarkis 12/🔺TOFA/JAK-i🔻in #elderly
🚩Approved after failure of TNFi
🚩⬆️ Risk of HZ with ⬆️age
👉Vaccinate w/Shingrix
🚩⬆️ Potential risk of DVT/PE in pts with VTE risk factors on 10mg bid dosing
@ManasiAgrawalMD
ncbi.nlm.nih.gov/pmc/articles/P…
🚩Approved after failure of TNFi
🚩⬆️ Risk of HZ with ⬆️age
👉Vaccinate w/Shingrix
🚩⬆️ Potential risk of DVT/PE in pts with VTE risk factors on 10mg bid dosing
@ManasiAgrawalMD
ncbi.nlm.nih.gov/pmc/articles/P…
@MondayNightIBD @SobiaMujtabaMD @JasonHouMD @DCharabaty @joshsteinbergMD @yaransarkis @ManasiAgrawalMD 13/ To Recap #IBD in the #Elderly
🎯Elderly make up ⅓ of all #IBD pts
🎯Tailor Rx based on “Fit” vs “Frail”
🚫Chronic Corticosteroids
⬆️ Risk of lymphoma w IMM
⬆️ Risk of infxn w biologics related to age, frailty & MOA
🔑 Vaccinate for flu/pneumoc. in all & Shingles if TOFA
🎯Elderly make up ⅓ of all #IBD pts
🎯Tailor Rx based on “Fit” vs “Frail”
🚫Chronic Corticosteroids
⬆️ Risk of lymphoma w IMM
⬆️ Risk of infxn w biologics related to age, frailty & MOA
🔑 Vaccinate for flu/pneumoc. in all & Shingles if TOFA


@MondayNightIBD @SobiaMujtabaMD @JasonHouMD @DCharabaty @joshsteinbergMD @yaransarkis @ManasiAgrawalMD @DrMalSimons @FITWITMD @Waseem_AhmedMD @LaurenFeldMD @MayssanMuftah @JacquelineChuMD @MahamHayatMD @ptandonGI @MishahMD @DVinsard @RuthvikPadival @AlexaWeingarden @VivyTCmd @BilalMohammadMD @DrMohdZein @OmerShahabMD @HarisMD14 @mohammad @purnie_mae
• • •
Missing some Tweet in this thread? You can try to
force a refresh