
Neuroanatomy TOTD #11🧵
➡️intracanalicular facial nerve. IAC cross section➡️4 nerves; ant-sup➡️facial, ant-inf➡️cochlear (7-up/coke-down). Post nerves➡️sup&inf vestibular #medtwitter #meded #FOAMed #FOAMrad #neurorad #radiology #radres #neurology #neurosurgery #neuroanatomy
1/11
➡️intracanalicular facial nerve. IAC cross section➡️4 nerves; ant-sup➡️facial, ant-inf➡️cochlear (7-up/coke-down). Post nerves➡️sup&inf vestibular #medtwitter #meded #FOAMed #FOAMrad #neurorad #radiology #radres #neurology #neurosurgery #neuroanatomy
1/11

Facial motor nucleus is in the pontine tegmentum; axons loop dorsally around the abducens nucleus, then course anterolaterally, exiting the brainstem at the CPA.
2/11
2/11
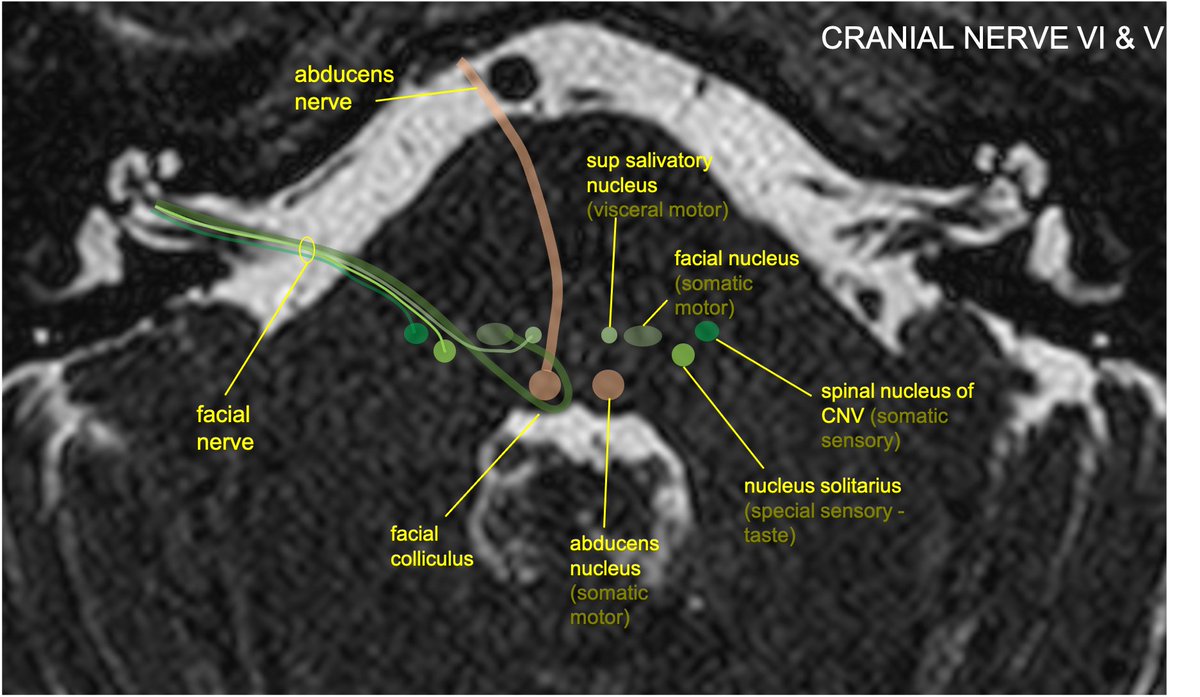
The nervus intermedius (NI) is composed of preganglionic parasympathetic fibers w/cell bodies in the sup salivatory nucleus, taste fibers w/cell bodies in the nucleus solitarius, and somatic sensory input from EAC/external ear, w/cell bodies in the spinal nucleus of CNV.
3/11
3/11
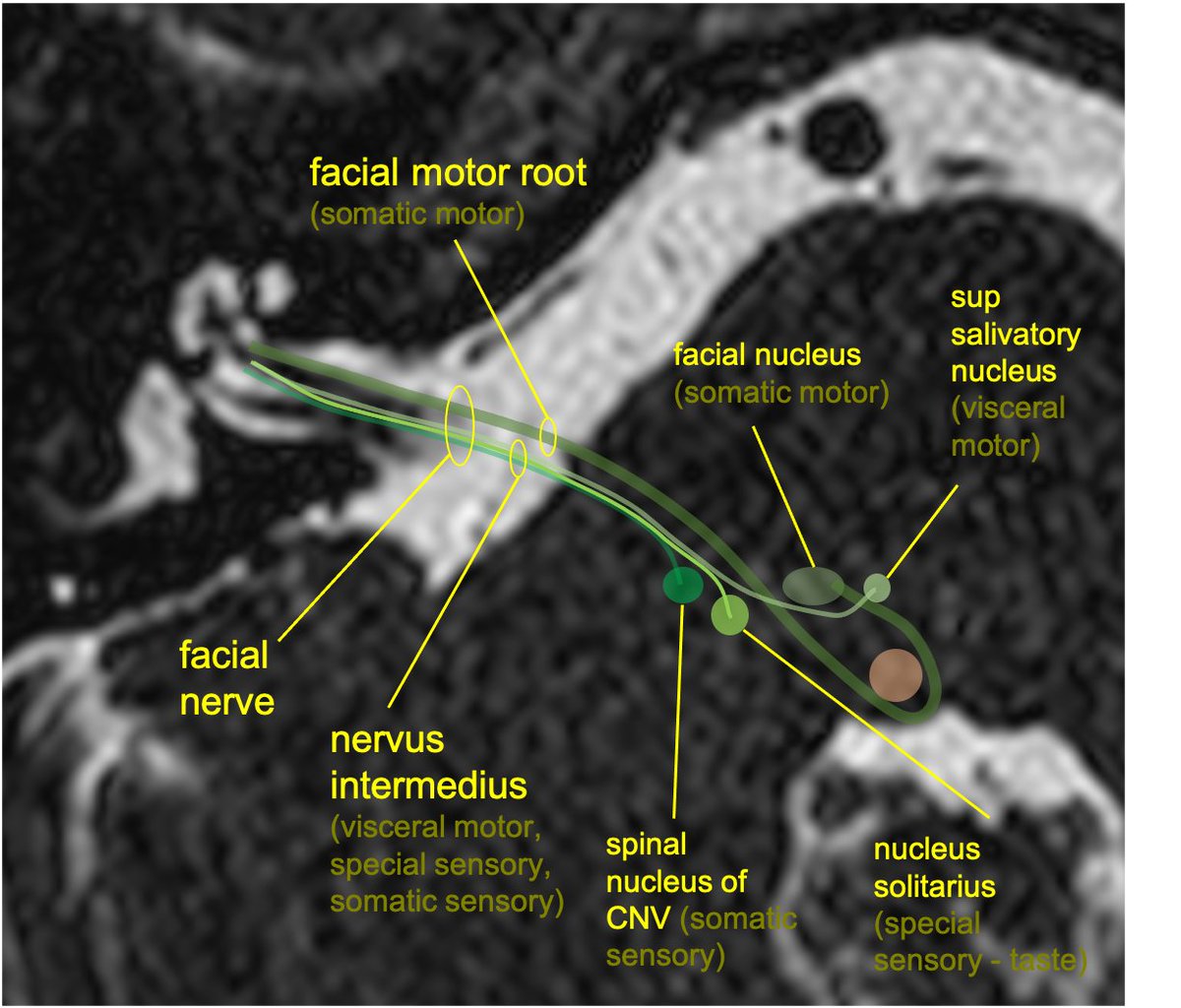
Although NI and the motor components of CN7 are anatomically separate, they are generally not distinguished on imaging of the IAC.
4/11
4/11

Facial nerve is separated into 4 intratemporal segments (intracanalicular, labyrinthine, tympanic, mastoid). Cisternal is from the CPA to the internal auditory meatus. Intracanalicular within the IAC. Labarynthine is from the fundus of the IAC to the geniculate ganglion.
5/11
5/11

The greater superficial petrosal nerve (GSPN) arises from geniculate ganglion w/preganglionic parasymp fibers (and some taste/sensation) along floor of middle cranial fossa, through pterygoid canal, to pterygopalatine fossa➡️lacrimal gland(TOTD #1) (
6/11
https://twitter.com/aaronrutman/status/1306712450616754177)
6/11

The tympanic segment starts at the sharp turn of the geniculate ganglion and runs horizontally/posterolaterally along the medial margin of the middle ear. (There are no branches of the tympanic segment).
7/11
7/11
At the post middle ear, the mastoid segment begins➡️turns inferiorly through the facial canal in the mastoid, giving off 3 branches: nerve of stapedius, chorda tympani, and sensory auricular branch.
8/11
8/11

The chorda tympani includes taste fibers to the ant 2/3 of the tongue, as well as preganglionic parasympathetic fibers which extend to the submandibular ganglion. The ch tymp traverses the middle ear and eventually joins with the lingual nerve (CNV) on its way to the tongue
9/11
9/11

CN7 exits bony facial canal through stylomastoid foramen➡️gives off 3 motor branches: post auricular, digastric, stylohyoid. Traverses parotid gland, divides into 5 branches: temporal, zygomatic, buccal, marginal mandibular, cervical (mnemonic: To Zanzibar By Motor Car).
10/11
10/11

Relevant path: Bell’s palsy (may be HSV reactiv in geniculate ganglion); variable effects on CN7: facial palsy, hyperacusis (stapedius), pain at jaw/ear (sensory auricular), loss of taste (ch tymp), changes in tear (GSPN) and saliva production (ch tymp)
#radiopaedia case
11/11
#radiopaedia case
11/11

• • •
Missing some Tweet in this thread? You can try to
force a refresh

















