Hello, #MedTwitter, #MedStudentTwitter, #NeuroTwitter
It’s been a long time since my last clinical neuroanatomy #tweetorial, sorry about that!
Here's a new one:
MOTOR SUPPLY to the FACE and Approach to FACIAL WEAKNESS
cc @Tracey1milligan @CPSolvers @DxRxEdu @MedTweetorials
It’s been a long time since my last clinical neuroanatomy #tweetorial, sorry about that!
Here's a new one:
MOTOR SUPPLY to the FACE and Approach to FACIAL WEAKNESS
cc @Tracey1milligan @CPSolvers @DxRxEdu @MedTweetorials
I'm glad #EndNeurophobia campaign has grown but please check out the rest of my feed, which seeks to amplify voices I’m learning from on the path to becoming an antiracist ally
@CPSolvers #antiracism series
Subscribe:@ThePraxisPod @SocMedOnAir
Follow @InequityKills @LashNolen
@CPSolvers #antiracism series
Subscribe:@ThePraxisPod @SocMedOnAir
Follow @InequityKills @LashNolen
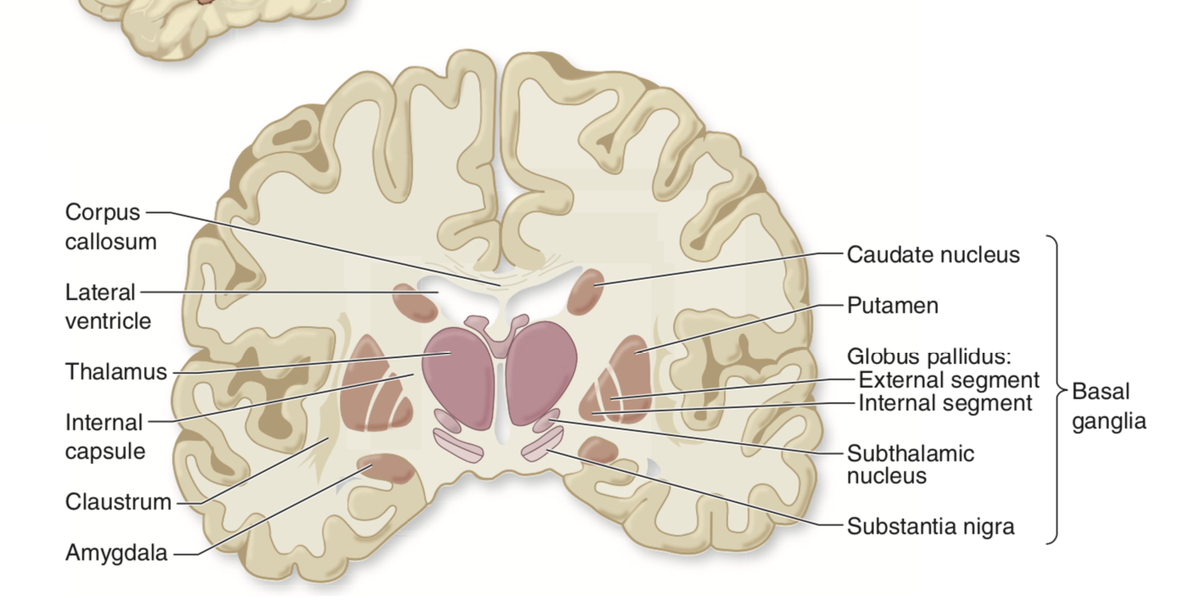
Just like the arms and legs the facial motor pathway has both UPPER motor neurons and LOWER motor neurons:
The UMNs begin in the lateral precentral gyrus, descend with the internal capsule, through the cereeral peduncle to arrive at the facial nucleus in the PONS.
The UMNs begin in the lateral precentral gyrus, descend with the internal capsule, through the cereeral peduncle to arrive at the facial nucleus in the PONS.

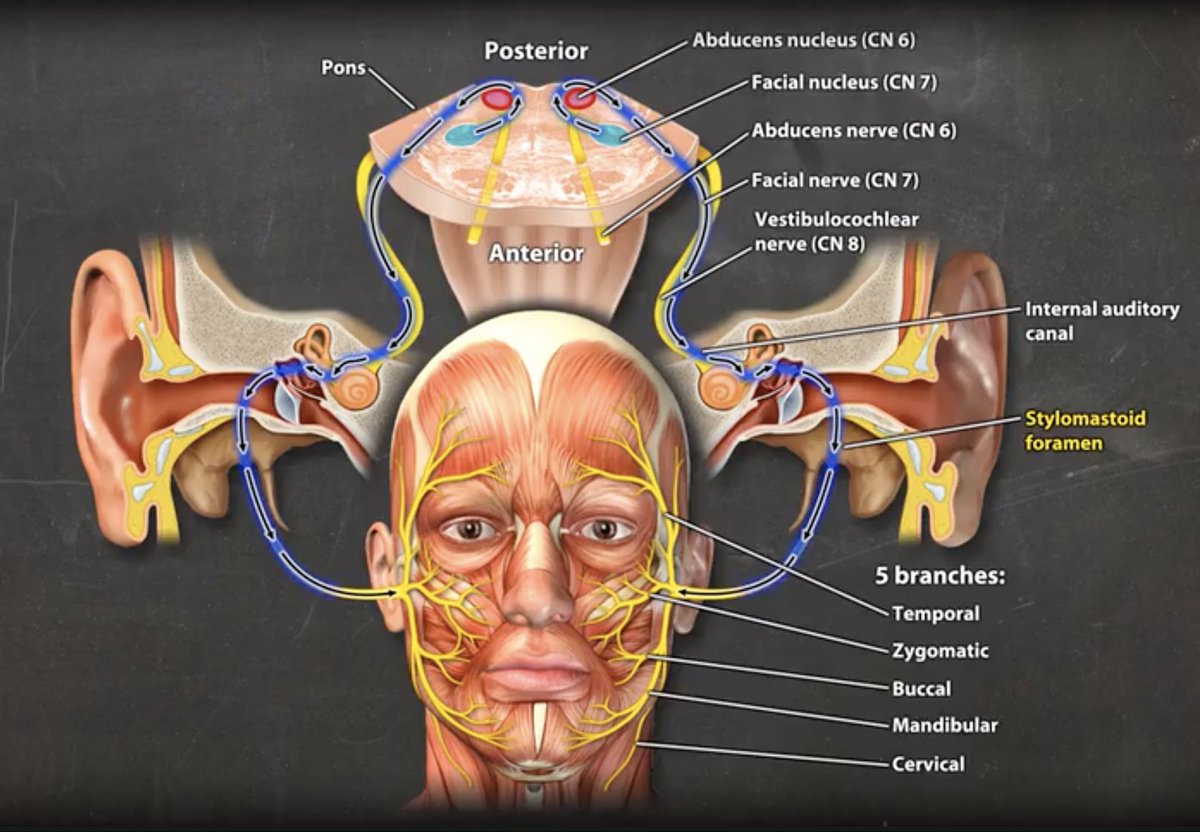
The LMNs begin in the facial nucleus, travel as the seventh cranial nerve fascicle through the pons (looping around the 6th nerve nucleus), and exit the pons as the 7th cranial nerve, which passes through the internal auditory canal en route to the face, where it -> 5 branches
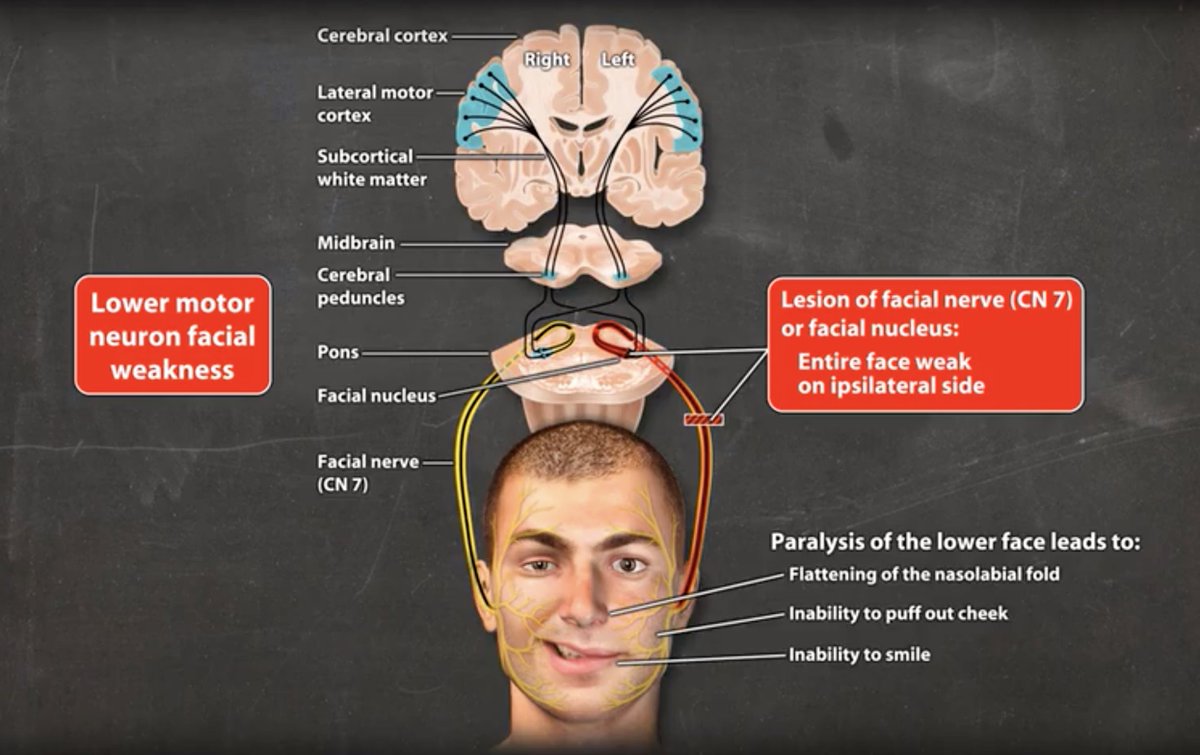
Facial weakness generally either involves the entire face on one side (or both sides) OR the lower face only
The WHOLE face = lesion of CN 7 or its nuc (LMN lesion)
The LOWER face ONLY = lesion of brain or brainstem above the level of the CN7 nuc (UMN lesion)
The WHOLE face = lesion of CN 7 or its nuc (LMN lesion)
The LOWER face ONLY = lesion of brain or brainstem above the level of the CN7 nuc (UMN lesion)

Some remember "Upper Spares Upper," for upper face being spared in UMN lesion but since Lower does NOT spare Lower, let’s understand the underlying anatomy in case we forget the mnemonic...
Just like the arm and leg, the LEFT cerebral hemisphere controls the RIGHT face, and the RIGHT cerebral hemisphere controls the left face.
BUT there is also a sort of BACKUP just for the upper face, that runs IPSIlateral
BUT there is also a sort of BACKUP just for the upper face, that runs IPSIlateral


So Left cerebral hemisphere sends input to the R CN7 nucleus for the whole face AND input to the L CN 7 nucleus just for the upper face
And Right cerebral hemisphere sends input to the LCN7 nucleus for the whole face AND input to the R CN 7 nucleus just for the upper face
And Right cerebral hemisphere sends input to the LCN7 nucleus for the whole face AND input to the R CN 7 nucleus just for the upper face


So if there’s a RIGHT upper motor neuron lesion (brain or upper brainstem), there would have been weakness of the whole left face contralaterally…BUT thanks to the left hemisphere ipsilateral input to the upper face (the BACKUP), the left upper face is spared!

So Upper spares upper and only the lower face is affected:
UMN lesion: failure to smile or puff cheek on contralateral side, with SPARED eye closure, eyebrow raise, and forehead wrinkle.
UMN lesion: failure to smile or puff cheek on contralateral side, with SPARED eye closure, eyebrow raise, and forehead wrinkle.

In contrast if there is a lesion of CN 7 (or its nucleus), the ENTIRE face will be weak!
The CN7 nucleus/nerve receive ipsilateral and contralateral input but if the nerve is lesioned, we’ve lost the primary pathway and the ‘backup’…
The CN7 nucleus/nerve receive ipsilateral and contralateral input but if the nerve is lesioned, we’ve lost the primary pathway and the ‘backup’…
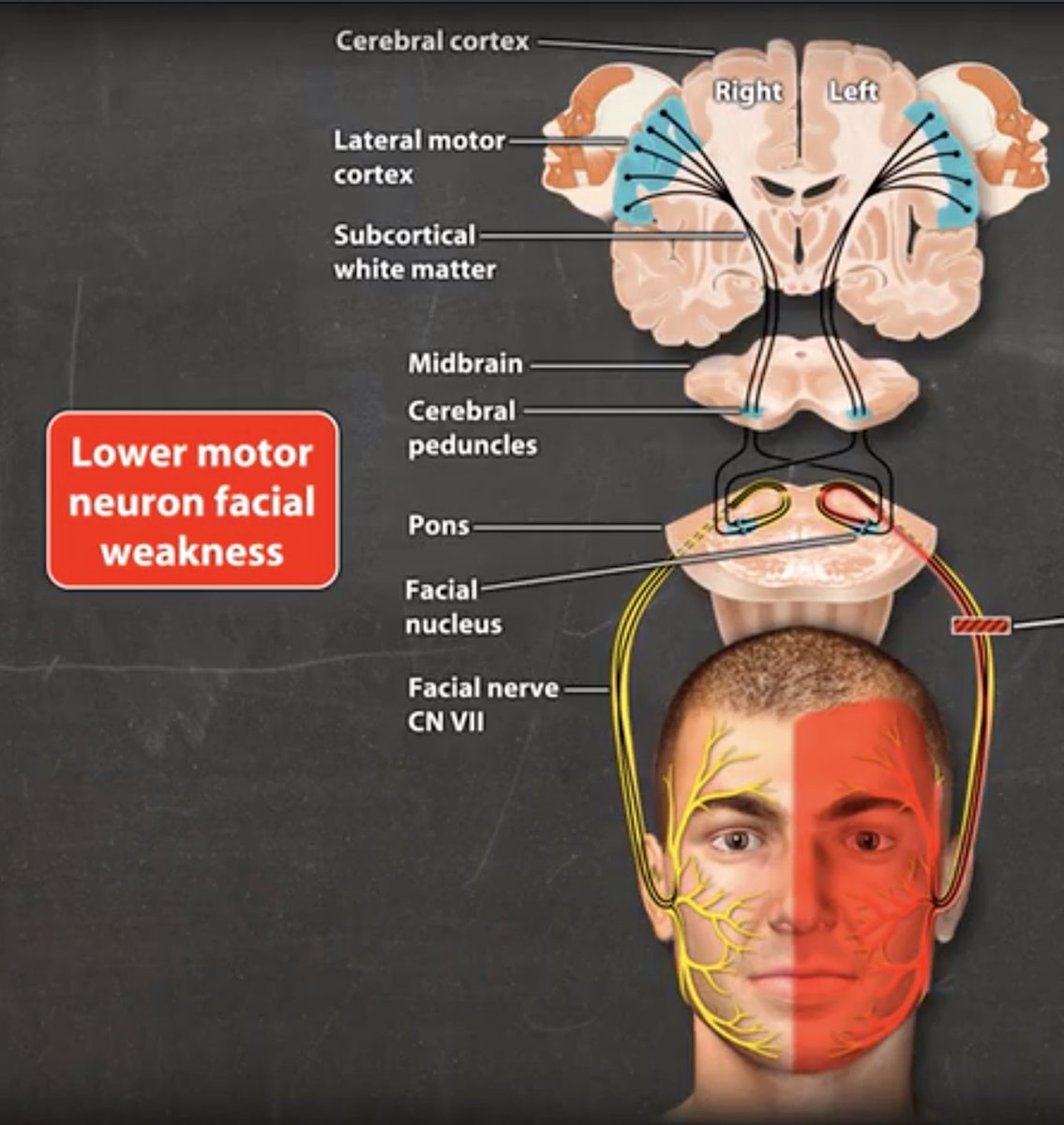
So remember: whole nerve = whole face
So in addition to inability to smile, the patient w a LMN (CN 7/nuc) lesion will have difficulty closing the eye, raising the eyebrow, wrinkling the forehead.
So in addition to inability to smile, the patient w a LMN (CN 7/nuc) lesion will have difficulty closing the eye, raising the eyebrow, wrinkling the forehead.


Think of UMN lesion like cancelled flight–airport (CN7 nuc) is still open so flights from other locations can make it in (the ipsilateral backup for upper face).
CN7 lesion=airport closure–doesn’t matter if other airports are open, this airport closed, so no flights in or out!
CN7 lesion=airport closure–doesn’t matter if other airports are open, this airport closed, so no flights in or out!
So WHOLE face = CN 7. We call this peripheral pattern facial weakness. And usually it is peripheral meaning a problem with CN7
DDx = Bell’s palsy, Lyme, Guillain-Barre, Sarcoid, HIV (time of seroconversion), compression from vestibular schwannoma (7 / 8 travel together in IAC).
DDx = Bell’s palsy, Lyme, Guillain-Barre, Sarcoid, HIV (time of seroconversion), compression from vestibular schwannoma (7 / 8 travel together in IAC).

If CN 7 nucleus/fascicle affected in the pons, a CENTRAL lesion can cause PERIPHERAL pattern weakness (whole face), often accompanied by ipsilateral CN 6 (abduction palsy) bc of proximity of CN6/7 nuclei and fascicles + contralateral hemiparesis (bc of the not-yet-crossed CST)

If you see just the lower face weak with spared upper face, think UMN: brain or upper brainstem
This could be any process that can occur in the CNS: stroke, tumor, infection, demyelinating lesion...
This could be any process that can occur in the CNS: stroke, tumor, infection, demyelinating lesion...

In sum:
LOWER face ONLY = CONTRALATERAL UMN Lesion (brain or brainstem above facial nucleus; ipsilateral backup 'saved' the upper face)
WHOLE face= IPSILATERAL CN 7 (or its nucleus; if nucleus often accompanied by CN 6 +/- contralateral hemiparesis)
LOWER face ONLY = CONTRALATERAL UMN Lesion (brain or brainstem above facial nucleus; ipsilateral backup 'saved' the upper face)
WHOLE face= IPSILATERAL CN 7 (or its nucleus; if nucleus often accompanied by CN 6 +/- contralateral hemiparesis)

Want to see all this ANIMATED!?
Log in to your school library's subscription to AccessMedicine and go to ch 13 in my book or this link: accessmedicine.mhmedical.com/MultimediaPlay…
Taking requests for next tweetorial!
#EndNeurophobia 🧠❤️
Log in to your school library's subscription to AccessMedicine and go to ch 13 in my book or this link: accessmedicine.mhmedical.com/MultimediaPlay…
Taking requests for next tweetorial!
#EndNeurophobia 🧠❤️
and @AvrahamCooperMD #curiousclinician can you tell us why we developed a 'backup' for the upper face...? is it because protecting the eye is evolutionary more important than smiling...? I've never found the answer to why we have this ipsilateral 'backup' pathway...
• • •
Missing some Tweet in this thread? You can try to
force a refresh