📍Huge blow—UK had halted plans to open rapid-turnaround #COVID19 tests across England amid concerns about the accuracy. Huge blow to UK’s £100bn “Operation Moonshot” mass-testing plan, to increase daily tests from 430k to 10mil. Poor 🇬🇧 case surging too.
theguardian.com/world/2020/dec…
theguardian.com/world/2020/dec…

2) Experts in testing and understand immunology like @michaelmina_lab think the test is good in capturing **INFECTIOUS** virus, which is key.
https://twitter.com/michaelmina_lab/status/1341638540095074308
3) it indeed caught the critical high viral cases
https://twitter.com/michaelmina_lab/status/1341639144271998976
4) The UK Birmingham study had serious methods problems.
https://twitter.com/michaelmina_lab/status/1341652199735226369
5) there are MORE ACCURATE RAPID ANTIGEN tests like the Abbott PanBio test available in continental Europe. It’s cheap and relatively very accurate. See thread 🧵 below 👇
https://twitter.com/drericding/status/1329024406396555269
6) comparing nasal PanBio rapid antigen test vs Nasal PCR #COVID19 test:
➡️VERY good.
📌Sensitivity 98.1% (99.0% for samples with higher viral load PCR Ct<=33)
📌Specificity 99.8% (ie 0.2% false positive)
(Sensitivity is 91-94% vs deep nasopharyngeal PCR).
➡️VERY good.
📌Sensitivity 98.1% (99.0% for samples with higher viral load PCR Ct<=33)
📌Specificity 99.8% (ie 0.2% false positive)
(Sensitivity is 91-94% vs deep nasopharyngeal PCR).

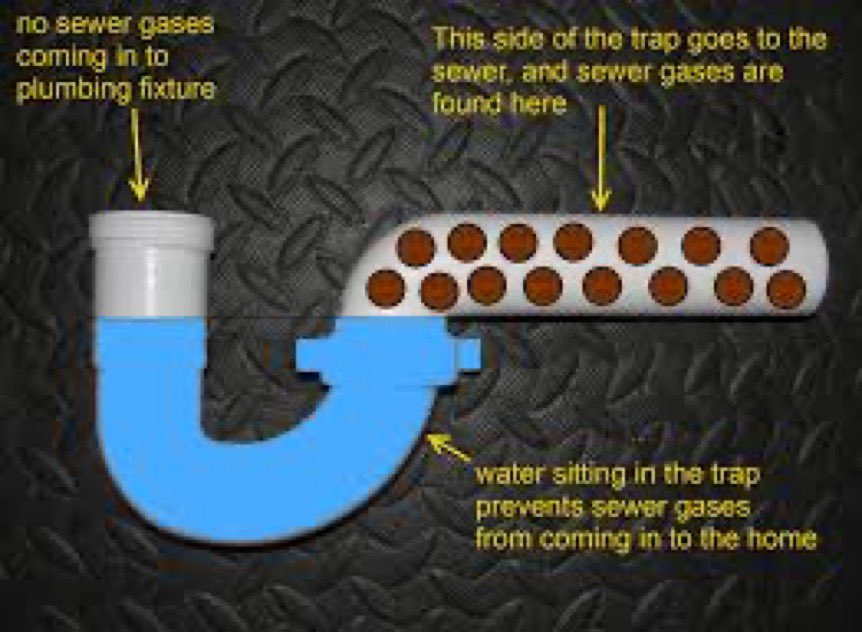
7) Thus, @michaelmina_lab thinks the lateral flow rapid antigen test is still indeed good for population screening.
Here is how they work.
Here is how they work.
8) For this reason, just yesterday, UK regulators also just gave the go-ahead for lateral flow devices (LFDs), which give results in 30 minutes, to be used at home by members of the public, with a few minor caveats.
dailymail.co.uk/news/article-9…
dailymail.co.uk/news/article-9…
9) Notably, you can only use them to confirm you need to isolate - NOT to make decisions on whether to mix with family and friends. It should not be a passport to go party since it just focuses on active infectious status.

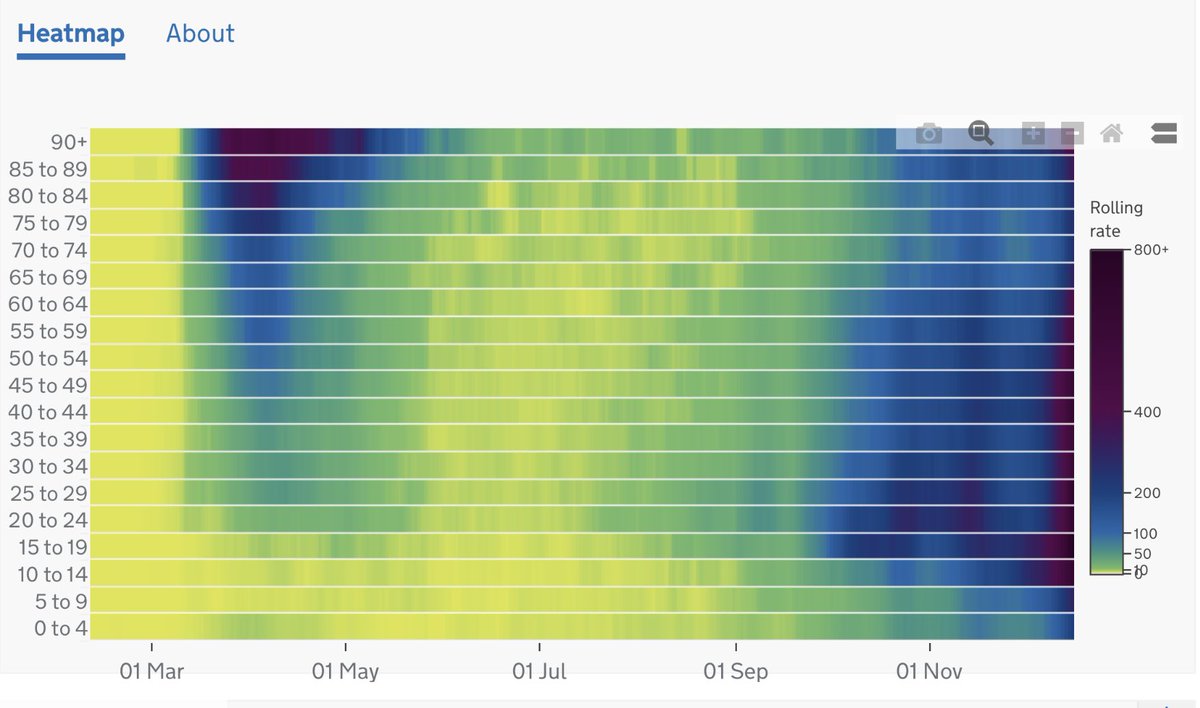
10) We really need rapid tests. Look how fast the epidemic is spreading in the UK recently. And especially among young people. But honestly all age groups.
• • •
Missing some Tweet in this thread? You can try to
force a refresh