I know others will have found these things before me but I've been home-schooling all day so only getting round to reading the roadmap now.
A few things stick out on first pass
(tl,dr: inequalities, testing, isolation support, social care, and inequalities).
A few things stick out on first pass
(tl,dr: inequalities, testing, isolation support, social care, and inequalities).
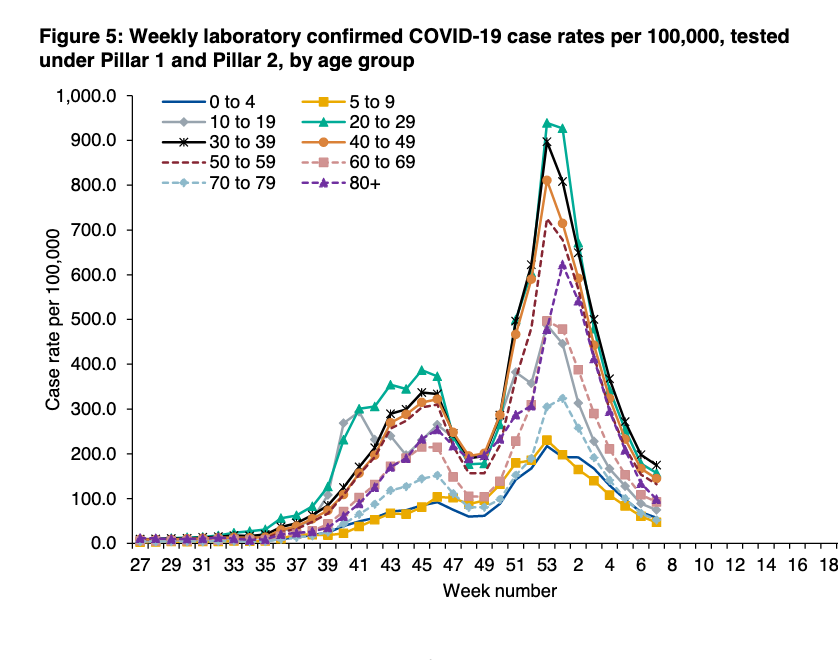
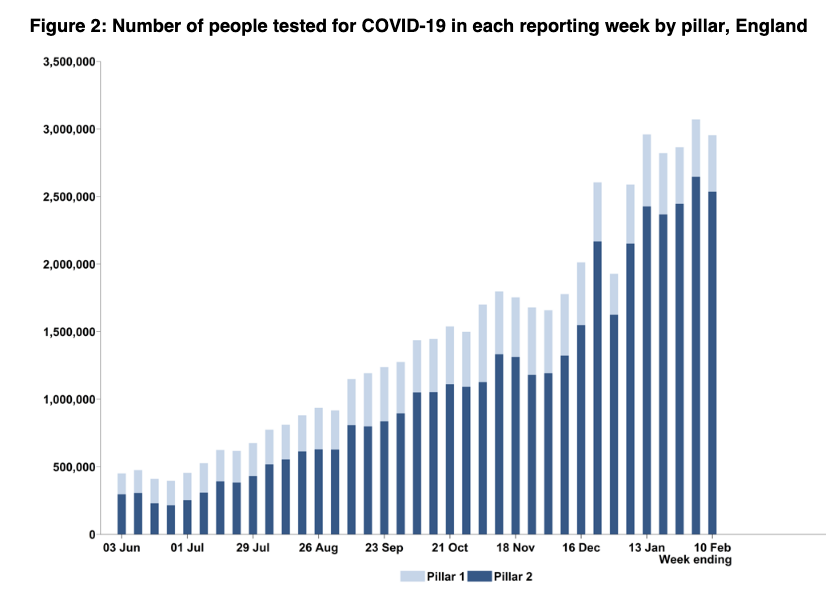
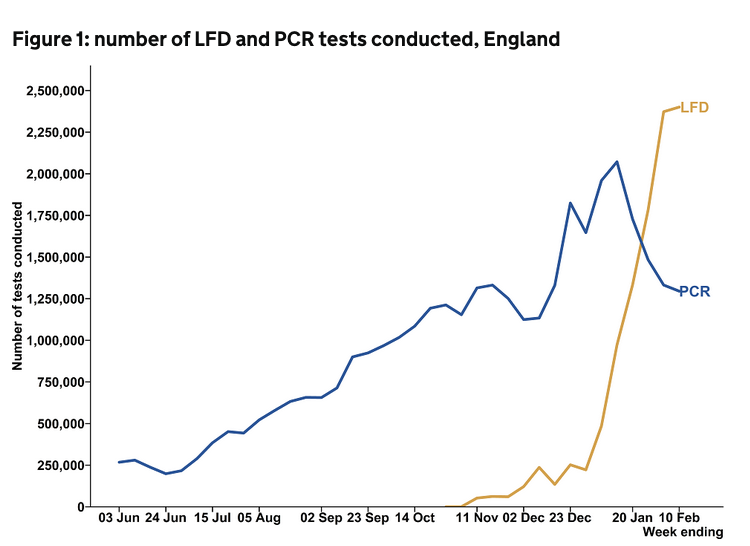
There's a section on 'Test, Trace and Isolate' (who says NHS Test and Trace has a branding problem).
As expected, big focus on testing plus a further £400m for local gov through the contain outbreak mgmt fund - details tbc but likely much is for local testing/variant mgmt.
As expected, big focus on testing plus a further £400m for local gov through the contain outbreak mgmt fund - details tbc but likely much is for local testing/variant mgmt.


As have said, there remains a big challenge of people not getting tested in the first place (fear of being unable to isolate, job insecurity, caring responsibilities etc). Surveys suggest just 1/3 get tested regularly if symptomatic.
The community collect model is not going to help more underlying structural societal issues. But the added £20m/month for local gov discretionary isolation support payment is v welcome and *will* help.
The next piece missing is work with employers to help those in insecure jobs.
The next piece missing is work with employers to help those in insecure jobs.

Bit more on testing, nothing on potential alternatives for people who find it difficult to safely isolate at home (multigenerational households etc), and this on regular testing as an alternative to isolation for contacts - lots of pilots but not ready yet.

There's plenty of what gov has done for care homes - but no more hints about any more substantive long term social care reform (also missing from the recently announced NHS reform plans)
https://twitter.com/hughalderwick/status/1359809210662473729?s=20
And there's a short section on 'disproportionately impacted groups' (note, the word 'inequalities' isn't mentioned in the report once).
COVID loves inequalities, both directly & indirectly disproportionately impacting those least able to cope.
COVID loves inequalities, both directly & indirectly disproportionately impacting those least able to cope.
Inequalities must be front and center of all gov policy - both to directly limit transmission, and as central to an inclusive long-term socioeconomic recovery.
A commitment around new approaches to viral spread won't be enough.
A commitment around new approaches to viral spread won't be enough.

Furthermore, resilience to future pandemics is far more than the establishment of the National Institute for Health Protection and improved outbreak mgmt.
It means a cross-gov approach to inequalities that ensures everyone is able to withstand future socioeconomic shocks.
It means a cross-gov approach to inequalities that ensures everyone is able to withstand future socioeconomic shocks.
Full report link:
assets.publishing.service.gov.uk/government/upl…
assets.publishing.service.gov.uk/government/upl…
• • •
Missing some Tweet in this thread? You can try to
force a refresh