@MondayNightIBD @DCharabaty 1/ Thiopurines are associated with an increased risk of NMSC (non-melanoma skin cancer)
Which of the following is true about this risk relative to non-exposed IBD pts, duration of thiopurine use , and after thiopurine cessation 🛑#Back2Basics #MondayNightIBD
Which of the following is true about this risk relative to non-exposed IBD pts, duration of thiopurine use , and after thiopurine cessation 🛑#Back2Basics #MondayNightIBD
@MondayNightIBD @DCharabaty 32 y/o M with UC here for f/u. In remission x7 yrs on AZA 75mg/d. He is here to discuss his concerns about his risk of lymphoma associated w/ AZA. (HSTCL= hepatosplenic T cell; EBV-L= EBV assoc lymphoma) Which statement is true?
#Back2Basics #MondayNightIBD
#Back2Basics #MondayNightIBD
@MondayNightIBD @DCharabaty 2/ ‼️Cancer risk in IBD‼️can be→
🔺Disease related (eg CRC, anal CA)
🔺Therapy related ( Skin, Lymphoma, Cervical, Anal)
🔺Disease related (eg CRC, anal CA)
🔺Therapy related ( Skin, Lymphoma, Cervical, Anal)
@MondayNightIBD @DCharabaty 3/ IBD-related CRC:
🧬Typically in areas of🔥 (endo or histo)
🧬Mean age < sporadic CRC (4th-5th decade vs 6th)
🧬Historic incidence: 18% >30 yrs of colitis
🧬Recent↓risk w/improved medical Rx & CRC surveillance
🧬accounts for ⅙ deaths in IBD
🧬Typically in areas of🔥 (endo or histo)
🧬Mean age < sporadic CRC (4th-5th decade vs 6th)
🧬Historic incidence: 18% >30 yrs of colitis
🧬Recent↓risk w/improved medical Rx & CRC surveillance
🧬accounts for ⅙ deaths in IBD

@MondayNightIBD @DCharabaty 4/CRC🔍in #IBD
⭐️ If UC>rectosigmoid or CD>⅓ colon
⭐️ Start at 8yrs of dis.
⭐️ q1-3 yrs, risk stratify
💎#B2BPearl:🤔risk factors: severity of 🔥,FH CRC, stricture in UC,foreshortened colon,age at dx, h/o dysplasia
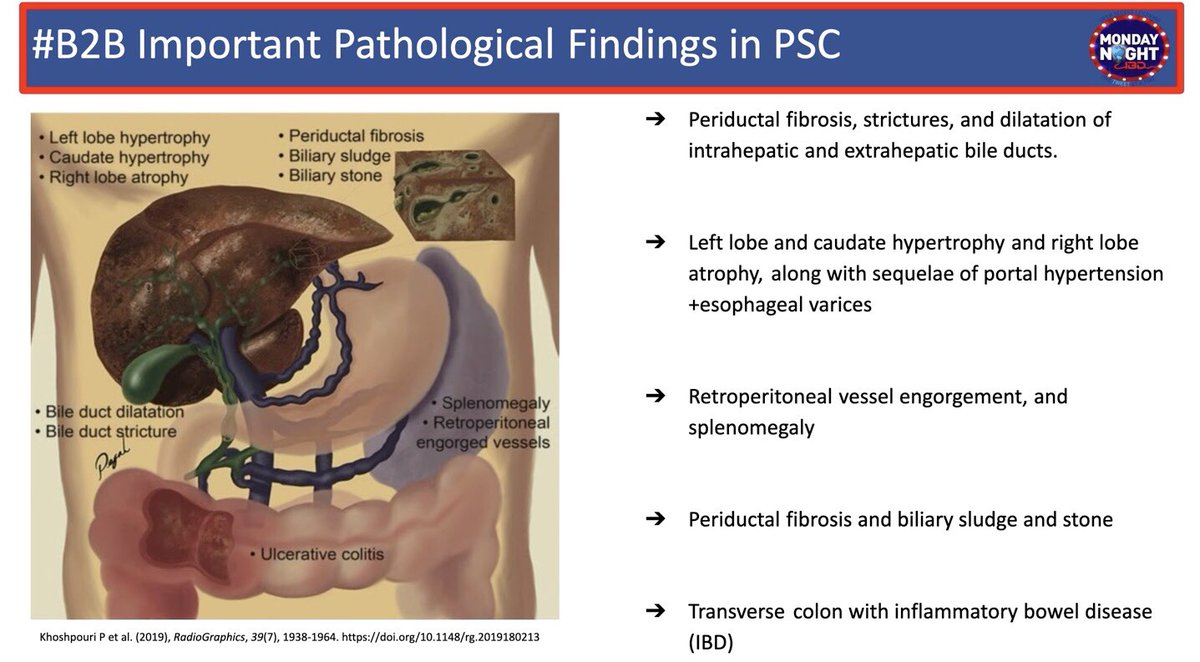
⭐️ If PSC (incl. postLT): Start at PSC dx, then qyr
⭐️ If UC>rectosigmoid or CD>⅓ colon
⭐️ Start at 8yrs of dis.
⭐️ q1-3 yrs, risk stratify
💎#B2BPearl:🤔risk factors: severity of 🔥,FH CRC, stricture in UC,foreshortened colon,age at dx, h/o dysplasia
⭐️ If PSC (incl. postLT): Start at PSC dx, then qyr


@MondayNightIBD @DCharabaty 5/ Skin CA in #IBD
⬆️risk for melanoma w/ biologics
⬆️risk for NMSC >1yr of thiopurines
⬆️ risk CD > UC
💎#B2BPearl Risk does not normalize after 🛑 AZA
⬆️risk for melanoma w/ biologics
⬆️risk for NMSC >1yr of thiopurines
⬆️ risk CD > UC
💎#B2BPearl Risk does not normalize after 🛑 AZA

@MondayNightIBD @DCharabaty 5b/ ⚠️RFs Skin CA #IBD
❗️Fair 👩🦳🧑🦳 skin
❗️ UV exposure
❗️Personal or FHx of melanoma
❗️Thiopurines (NMSC)
🙅🏻♀️Prevention🙅🏻
✅ ☀️ protection, sunscreen
✅Annual skin checks
doi.org/10.1053/j.gast…
@MLongMD
❗️Fair 👩🦳🧑🦳 skin
❗️ UV exposure
❗️Personal or FHx of melanoma
❗️Thiopurines (NMSC)
🙅🏻♀️Prevention🙅🏻
✅ ☀️ protection, sunscreen
✅Annual skin checks
doi.org/10.1053/j.gast…
@MLongMD

@MondayNightIBD @DCharabaty @MLongMD 6/ Lymphoma in #IBD
📍 ⬆️Risk in CD, M>F
📍Drug-assoc: mainly driven by #Thiopurines: (slides👇)
📍EBV-associated lymphoma Risk:
⚠️ ↑ w/ duration of thiopurine use
⚠️↑ w/ combo Rx
⚠️Normalize w/🛑thiopurines
🙅🏻♀️Prevention
✔️De-escalate if combo
✔️Consider non-thiopurine IS/MTX
📍 ⬆️Risk in CD, M>F
📍Drug-assoc: mainly driven by #Thiopurines: (slides👇)
📍EBV-associated lymphoma Risk:
⚠️ ↑ w/ duration of thiopurine use
⚠️↑ w/ combo Rx
⚠️Normalize w/🛑thiopurines
🙅🏻♀️Prevention
✔️De-escalate if combo
✔️Consider non-thiopurine IS/MTX



@MondayNightIBD @DCharabaty @MLongMD 7/ Cervical CA
📌HPV associated
⚠️ RFs: Thiopurines, smoking
🙅🏻♀️Prevention🙅🏻
✔️Education on RFs👆🏼
✔️HPV vaccine💉
✔️Annual Pap if 🚬 or thiopurines
doi.org/10.1002/ibd.20… @UmaMahadevanIBD
📌HPV associated
⚠️ RFs: Thiopurines, smoking
🙅🏻♀️Prevention🙅🏻
✔️Education on RFs👆🏼
✔️HPV vaccine💉
✔️Annual Pap if 🚬 or thiopurines
doi.org/10.1002/ibd.20… @UmaMahadevanIBD

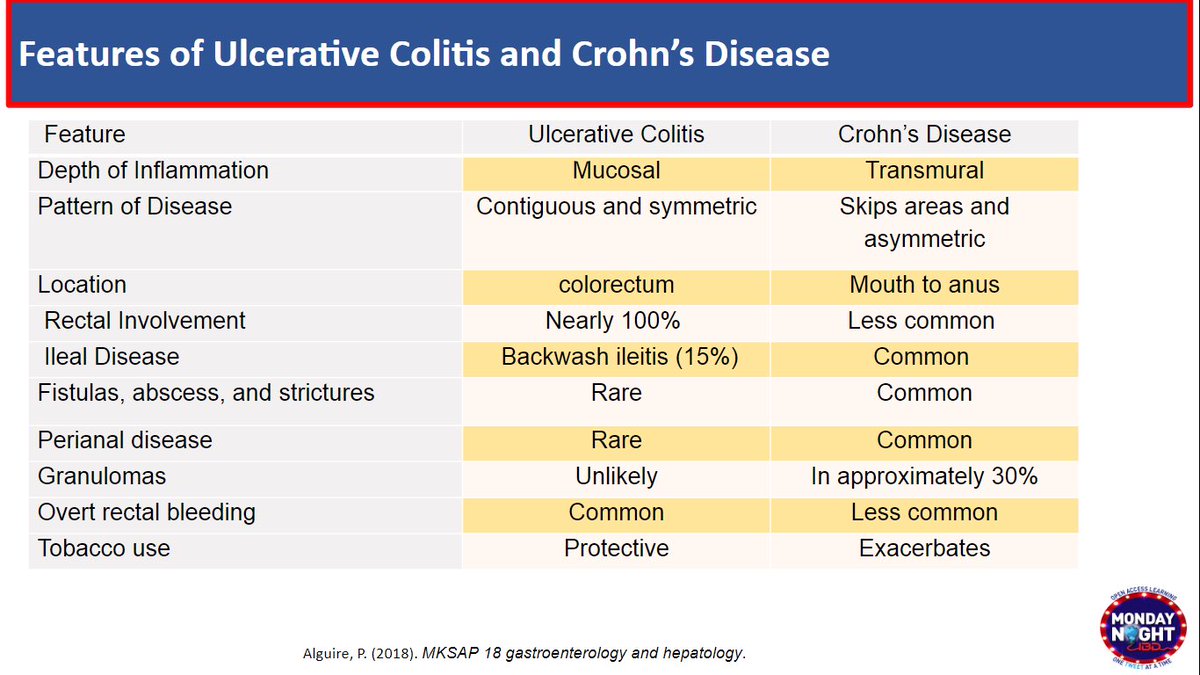
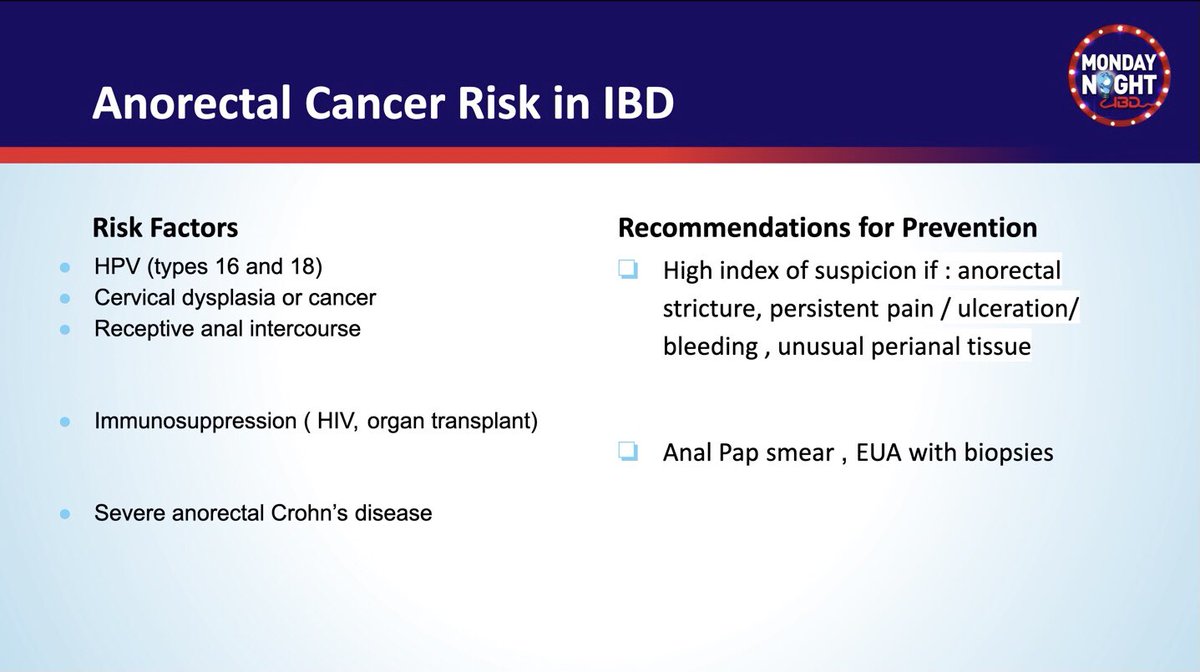
@MondayNightIBD @DCharabaty 8/ Anal CA in #IBD
⚠️ RFs:
▪️HPV 16 & 18
▪️Cervical dysplasia
▪️anal intercourse
▪️HIV
▪️Organ transplant
⚠️ RF: Severe anorectal Crohns
⚠️ RFs:
▪️HPV 16 & 18
▪️Cervical dysplasia
▪️anal intercourse
▪️HIV
▪️Organ transplant
⚠️ RF: Severe anorectal Crohns
@MondayNightIBD @DCharabaty 8b/ 🙅🏻♀️Prevention Anal CA #IBD
✅ Anal Pap smear
✅ EUA w/ Bx
💡Suspect anal CA if exuberant perianal tissue, stricture, ulceration, anorectal pain or🩸
doi.org/10.1016/j.croh…
✅ Anal Pap smear
✅ EUA w/ Bx
💡Suspect anal CA if exuberant perianal tissue, stricture, ulceration, anorectal pain or🩸
doi.org/10.1016/j.croh…
@MondayNightIBD @DCharabaty 9/ Let's Recap #CancerPrevention in #IBD #B2B
👉CRC
🔦C-scope start 8 yrs post-Dx, at Dx if PSC
👉Skin CA
🎯Avoid excess☀️
🎯Annual skin✅on IS
👉Lymphoma
⚖️Assess risk/benefits of thiopurines
👉Cervical CA
🔸HPV💉+Pap qyr if IS & 🚬
👉Anal CA
🔹🤔in anorectal Crohns & RFs
👉CRC
🔦C-scope start 8 yrs post-Dx, at Dx if PSC
👉Skin CA
🎯Avoid excess☀️
🎯Annual skin✅on IS
👉Lymphoma
⚖️Assess risk/benefits of thiopurines
👉Cervical CA
🔸HPV💉+Pap qyr if IS & 🚬
👉Anal CA
🔹🤔in anorectal Crohns & RFs
@MondayNightIBD @DCharabaty @DrMalSimons @JacquelineChuMD @BilalMohammadMD @rmulkimd @mohammad @purnie_mae @HarisMD14 @wingyanjoyce @ptandonGI @NasirSaleemMD @OmerShahabMD @Waseem_AhmedMD @GuiRamosMD @KM_Pawlak @anneliu_md @joshsteinbergMD @DVinsard @ibddocalex
@MondayNightIBD @DCharabaty @DrMalSimons @JacquelineChuMD @BilalMohammadMD @rmulkimd @mohammad @purnie_mae @HarisMD14 @wingyanjoyce @ptandonGI @NasirSaleemMD @OmerShahabMD @Waseem_AhmedMD @GuiRamosMD @KM_Pawlak @anneliu_md @joshsteinbergMD @DVinsard @ibddocalex @SobiaMujtabaMD @GCalderonMD @AparnaRepakaMD @DrAnatapia @KaazanPatricia @GhadyMoafa @MahamHayatMD
• • •
Missing some Tweet in this thread? You can try to
force a refresh