#INSPIRATION RCT comparing intermediate vs standard dose DVT prophylaxis, just published @jama:
-no benefit to additional anticoag in ICU patients w/ #COVID19:no reduction in mortality, MV, LOS or any 2° endpoint
-time to rethink COVID #anticoagulation?
1/
bit.ly/3vCluqK
-no benefit to additional anticoag in ICU patients w/ #COVID19:no reduction in mortality, MV, LOS or any 2° endpoint
-time to rethink COVID #anticoagulation?
1/
bit.ly/3vCluqK



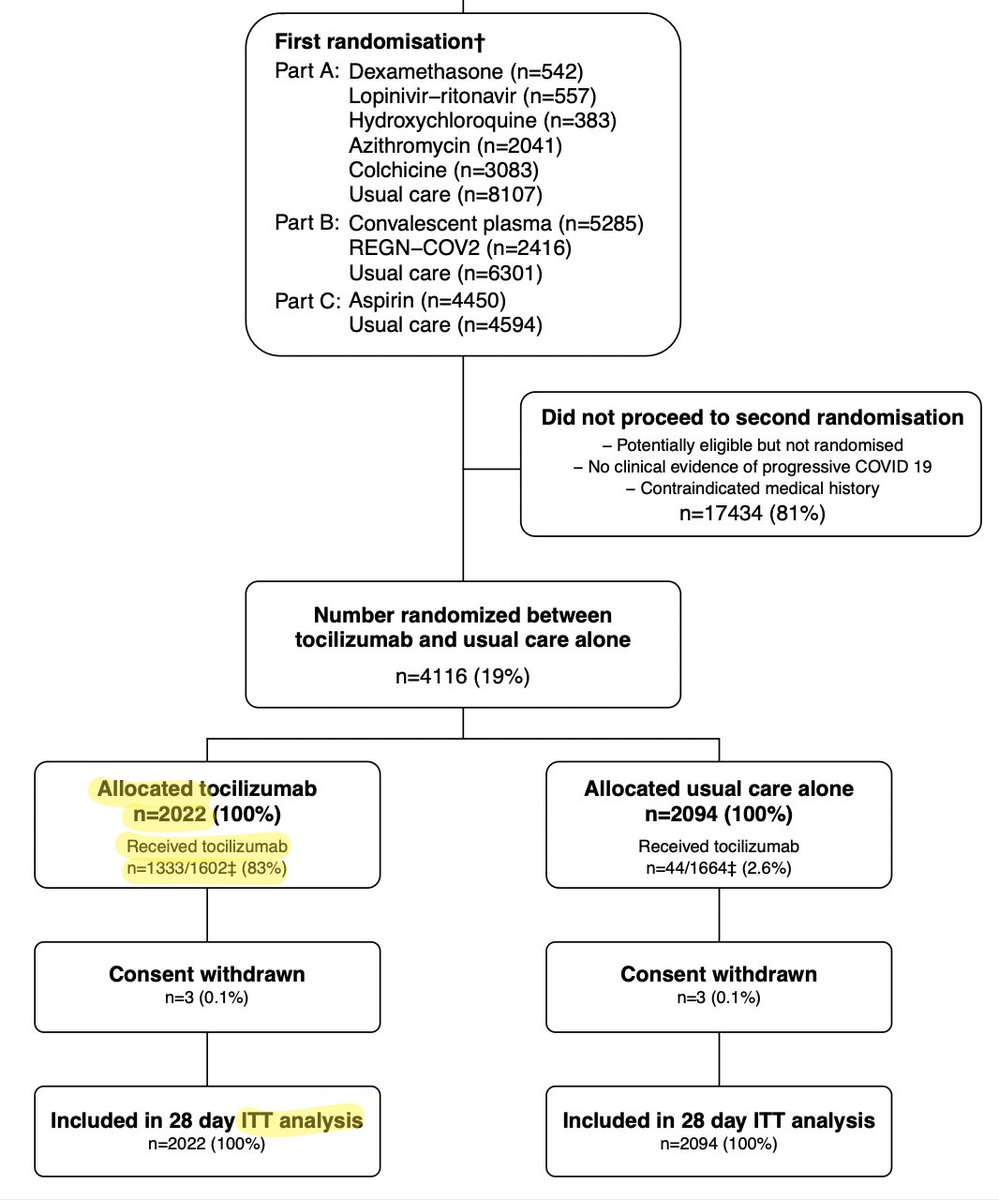
INSPIRATION was a 10 site open-label RCT in 🇮🇷 comparing intermediate vs standard dose prophylaxis in ICU patients with PCR-confirmed #COVID19.
LMWH was the primary intervention (~40 mg vs 1mg/kg daily), dosed appropriately for weight; UFH was used if the GFR was too low.
2/
LMWH was the primary intervention (~40 mg vs 1mg/kg daily), dosed appropriately for weight; UFH was used if the GFR was too low.
2/
Overall the groups were balanced (total n=562) & were fairly representative of US ICU cohorts with COVID19.
The use of HFNC was very low (~3%) compared to in the US, which may reflect different practice patterns/availability.
Most patients (>90%) received corticosteroids
3/
The use of HFNC was very low (~3%) compared to in the US, which may reflect different practice patterns/availability.
Most patients (>90%) received corticosteroids
3/

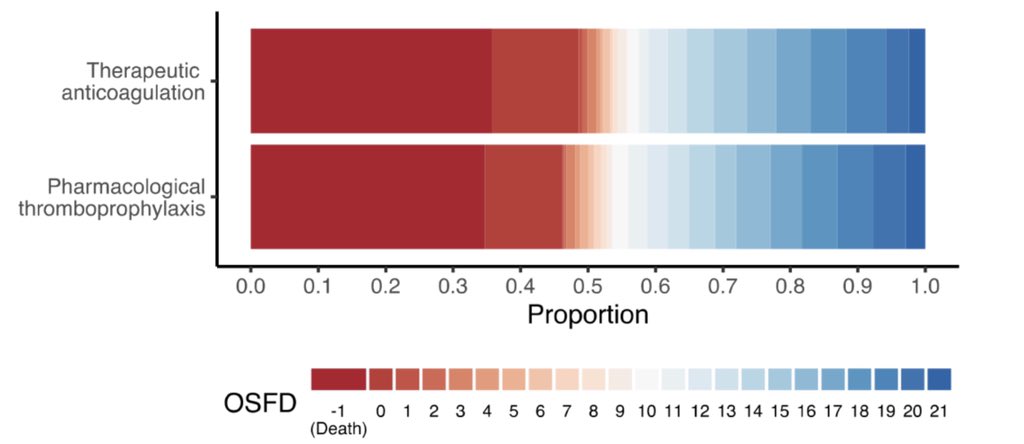
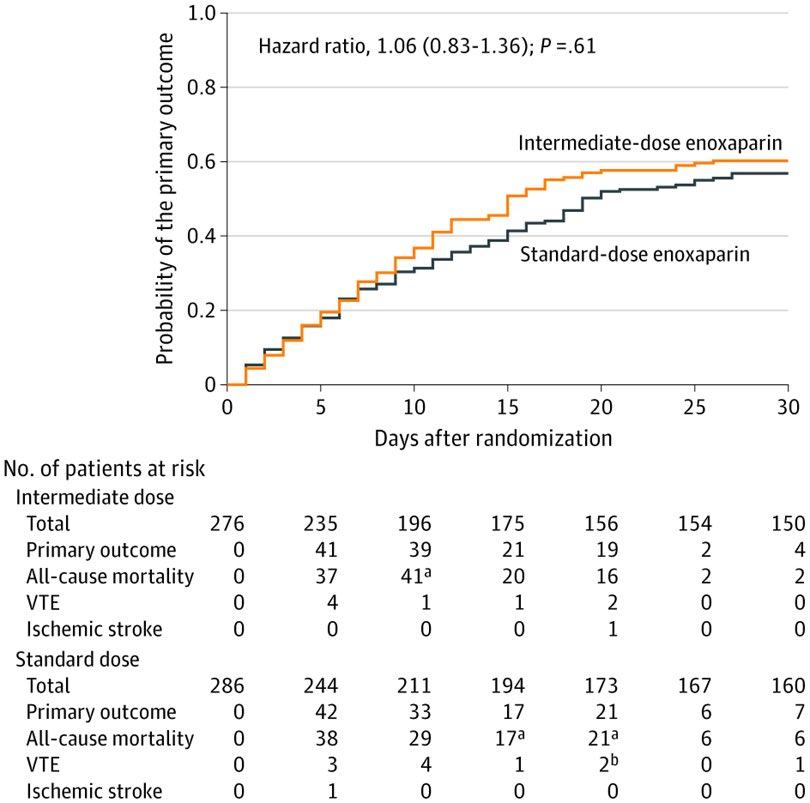
The 1° outcome - a composite of thrombosis, need for ECMO, & mortality - was not significant:
-46% intermediate dose (ID)
-44% standard dose (SD)
There was also no difference in 30-day mortality:
-41% ID
-43% SD
This is a low thrombosis rate & a slightly high mortality rate
4/
-46% intermediate dose (ID)
-44% standard dose (SD)
There was also no difference in 30-day mortality:
-41% ID
-43% SD
This is a low thrombosis rate & a slightly high mortality rate
4/



The low incidence of thrombosis is interesting. I can think of two explanations:
-they didn’t search for minor VTEs: only 63 duplex & 21 CTAs were done in the whole study
-there may be less thrombosis now: more ICU mobility, less sedation, & faster recoveries due to steroids
5/
-they didn’t search for minor VTEs: only 63 duplex & 21 CTAs were done in the whole study
-there may be less thrombosis now: more ICU mobility, less sedation, & faster recoveries due to steroids
5/


Some might argue that the low rate of VTE makes the study underpowered.
True except that the low rate of VTE with a high mortality rate suggests that people with COVID19 aren’t dying of (or even with) VTE. Hard to argue that anticoag is “lifesaving” in light of this finding.
6/
True except that the low rate of VTE with a high mortality rate suggests that people with COVID19 aren’t dying of (or even with) VTE. Hard to argue that anticoag is “lifesaving” in light of this finding.
6/
Aside from mortality, there was also no benefit to intermediate dose prophylaxis in terms of ventilator free days or ICU LOS.
There was also no benefit in *any* the prespecified subgroups (including patients with elevated D-dimer.)
Overall this was a very negative study.
6/
There was also no benefit in *any* the prespecified subgroups (including patients with elevated D-dimer.)
Overall this was a very negative study.
6/
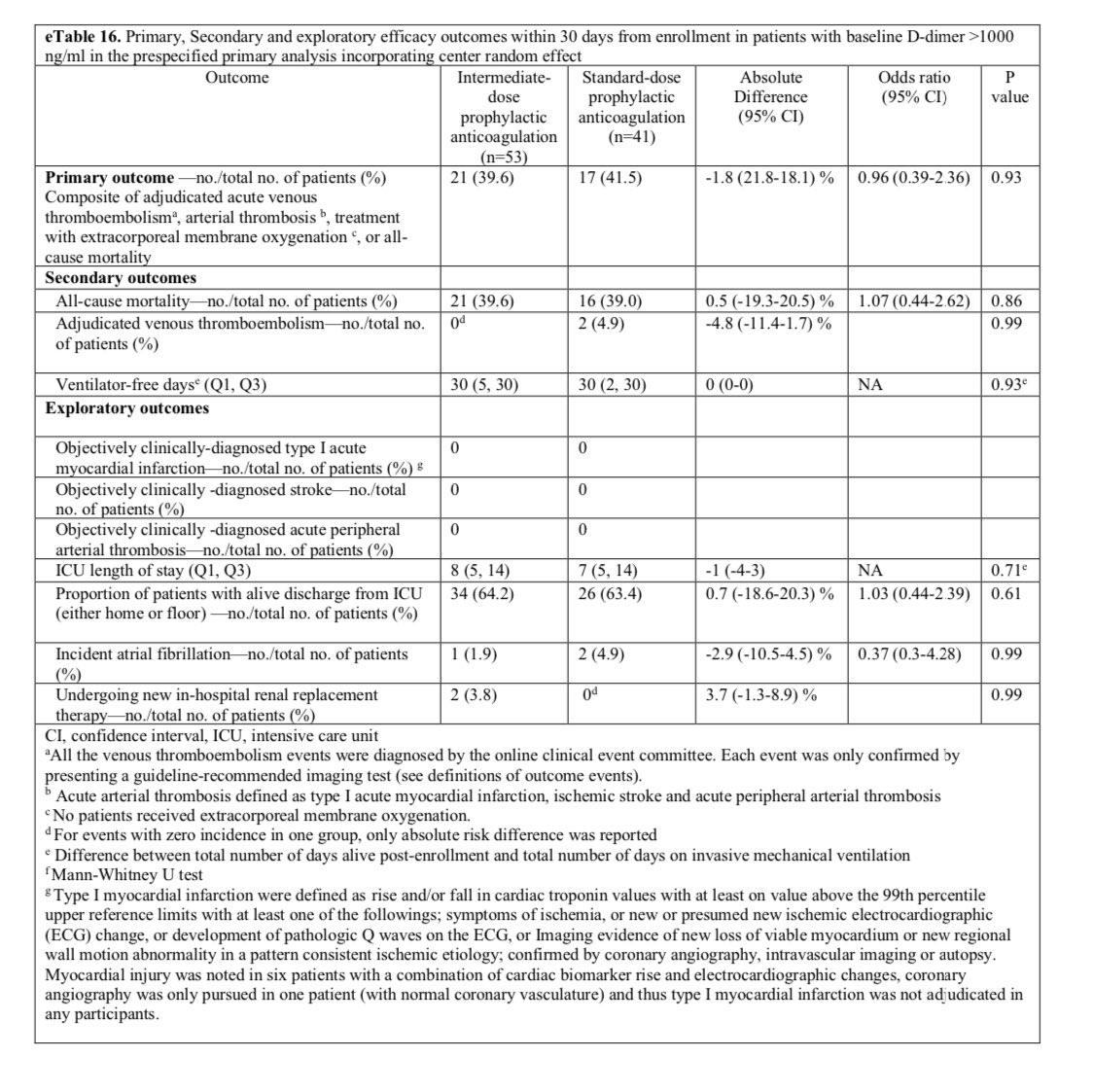
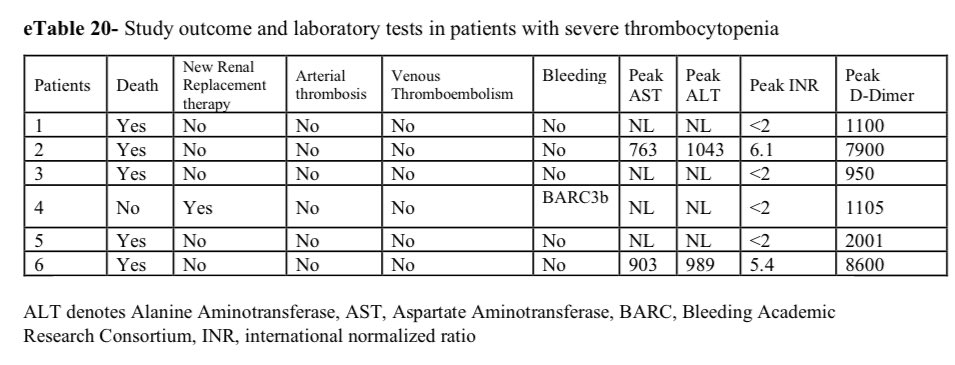
Unsurprisingly, there were numerically more bleeding events w/ intermediate dose anticoag.
Aside from 2x the bleeding risk, there was a safety signal: 6 ID pts had severe thrombocytopenia.
This suggests the risks of intermediate dose anticoag may be closer to treatment dose.
7/
Aside from 2x the bleeding risk, there was a safety signal: 6 ID pts had severe thrombocytopenia.
This suggests the risks of intermediate dose anticoag may be closer to treatment dose.
7/

Overall, I think this study is another 🚩for increased anticoagulation in people with COVID19 in the ICU.
Increased anticoagulation for an apparently “hypercoagulable” disease was a reasonable hypothesis, but it just hasn’t been validated in several high quality RCTs.
8/8
Increased anticoagulation for an apparently “hypercoagulable” disease was a reasonable hypothesis, but it just hasn’t been validated in several high quality RCTs.
8/8
• • •
Missing some Tweet in this thread? You can try to
force a refresh