A lot of praise for #ACIP's transparency
But de facto pausing for 7-10 days got the *substance* wrong, as @ashishkjha et al. observe
Understanding the expertise of ACIP members (deep but too narrow) can help understand why these decisions need diverse experts, not just MDs
1/6
But de facto pausing for 7-10 days got the *substance* wrong, as @ashishkjha et al. observe
Understanding the expertise of ACIP members (deep but too narrow) can help understand why these decisions need diverse experts, not just MDs
1/6
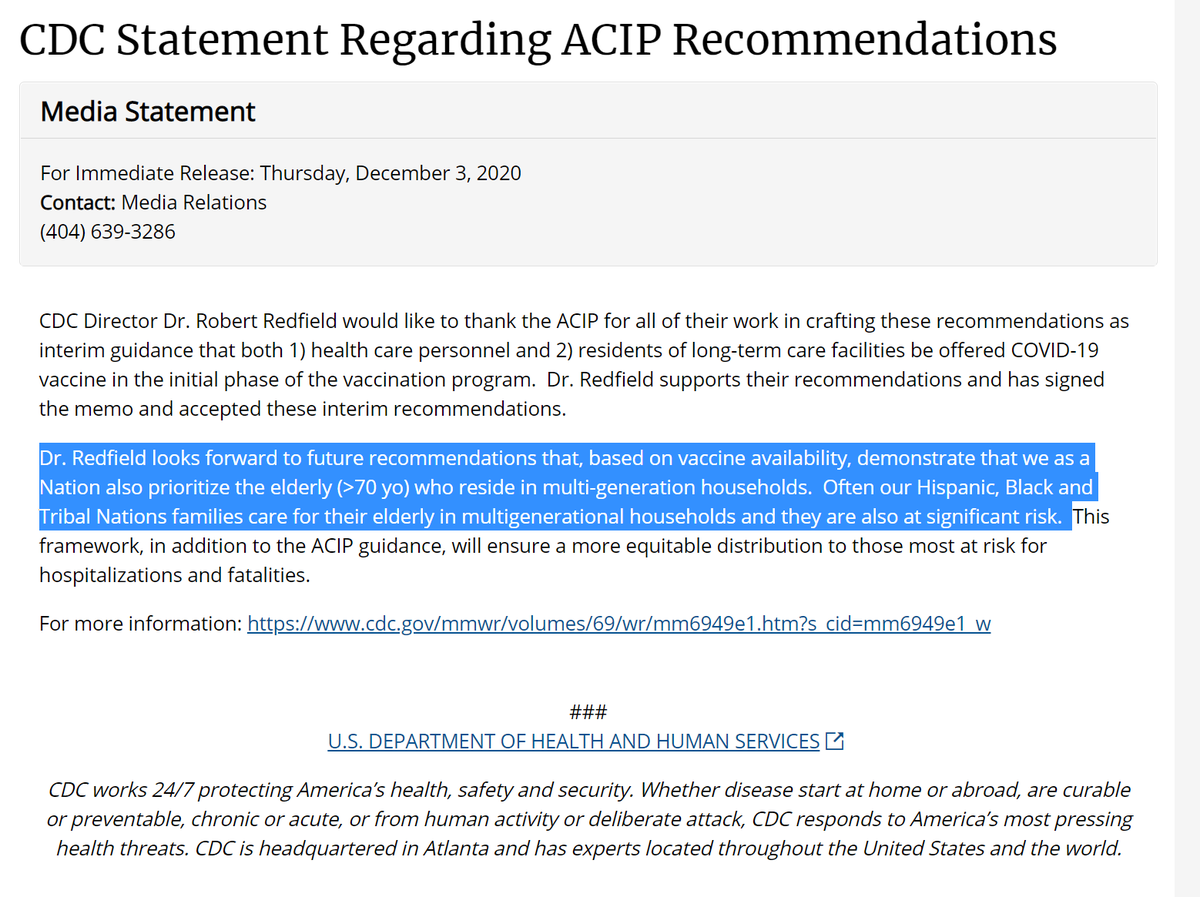
https://twitter.com/Yadav_supplychn/status/1382433633198280706
For vaccine allocation, CDC/NIH called on @NASEM_Health committee: nationalacademies.org/our-work/a-fra…
Not just MDs but:
- health econ (@healthecon_dan)
- behavioral health (@abuttenheim)
- literally wrote the book on "nonmaleficence" (Jim Childress)
- tribal health (@echohawkd3)
et al
2/6
Not just MDs but:
- health econ (@healthecon_dan)
- behavioral health (@abuttenheim)
- literally wrote the book on "nonmaleficence" (Jim Childress)
- tribal health (@echohawkd3)
et al
2/6
In contrast, every #ACIP voting member (exc 1 community member) is a MD/DO/RN. Couple w/a MPH. But no health econ. No ethicists. No behavioral sci. No tribal health experts.
Great group for indiv patient care & virology expertise
Not for managing trade-offs in a pandemic
3/6
Great group for indiv patient care & virology expertise
Not for managing trade-offs in a pandemic
3/6
There were warning signs
For vaccine allocation recs, #ACIP drew on outside ethics consultants. Not there yesterday
Overlooked several of NASEM's good equity recs, like CDC social vulnerability index
Best questions about tradeoffs yesterday came from the nonvoting members
4/6
For vaccine allocation recs, #ACIP drew on outside ethics consultants. Not there yesterday
Overlooked several of NASEM's good equity recs, like CDC social vulnerability index
Best questions about tradeoffs yesterday came from the nonvoting members
4/6
I wholeheartedly agree with @ashishkjha @thehowie and others that sadly #ACIP failed us yesterday by deciding not to decide
But I also think their composition set them up to fail, by depriving them of relevant expertise to deal with hard tradeoffs
5/6
But I also think their composition set them up to fail, by depriving them of relevant expertise to deal with hard tradeoffs
5/6
https://twitter.com/ashishkjha/status/1382536896555925509?s=20
A prominent theme yesterday in support of an extended pause: "nonmaleficence" "do no harm"
Having Jim Childress to explain why "nonmaleficence" isn't enough in public health decisions helped NASEM ethics.org.au/big-thinkers-t…
Having nobody like him hurt ACIP
https://twitter.com/amarkelkar/status/1382436517763809282?s=20
Having Jim Childress to explain why "nonmaleficence" isn't enough in public health decisions helped NASEM ethics.org.au/big-thinkers-t…
Having nobody like him hurt ACIP
I realized I forgot to link the ACIP bios: cdc.gov/vaccines/acip/…
Amazing (but duplicative) medical & infectious disease expertise. Little other expertise.
Compare to NASEM:
nationalacademies.org/our-work/a-fra…
ACIP needed some of these folks, not just great MD/inf disease experts
7/6
Amazing (but duplicative) medical & infectious disease expertise. Little other expertise.
Compare to NASEM:
nationalacademies.org/our-work/a-fra…
ACIP needed some of these folks, not just great MD/inf disease experts
7/6
Another limitation: many ACIP folks specialize in *childhood* vaccines.
Dr Long, who wanted 1-month(!) pause, is a pediatrics person:
Pausing pediatric rotavirus vax in 2010 was sensible
Pausing J&J in a pandemic way different.
Dr Long, who wanted 1-month(!) pause, is a pediatrics person:
https://twitter.com/abuttenheim/status/1382434160531357696?s=20
Pausing pediatric rotavirus vax in 2010 was sensible
https://twitter.com/drJoshS/status/1381984727775784961?s=20
Pausing J&J in a pandemic way different.
Point that rotavirus pause had a *very* different background context than pausing a vaccine in a pandemic nicely made by someone with relevant expertise here:
https://twitter.com/JSawyer330/status/1382316817650229250?s=20
• • •
Missing some Tweet in this thread? You can try to
force a refresh