Let's take a look at the updated NACI recommendations for the AstraZeneca vaccine...
Thread based on Appendix E, analyzing benefits of the AstraZeneca vaccine (preventing ICU admissions & deaths from COVID) vs risks of waiting for a later mRNA vaccine: canada.ca/content/dam/ph…
Thread based on Appendix E, analyzing benefits of the AstraZeneca vaccine (preventing ICU admissions & deaths from COVID) vs risks of waiting for a later mRNA vaccine: canada.ca/content/dam/ph…
QUICK SUMMARY: if you're in AB or ON, or anywhere with high COVD cases, the protections the AstraZeneca vaccine offer outweigh the rare but real risks -- at any age.
Also seems true for 30+ in areas with medium COVID levels.
Note current supply & provincial eligibility criteria
Also seems true for 30+ in areas with medium COVID levels.
Note current supply & provincial eligibility criteria
IMPORTANT: I'm trained as a scientist, but in neuroscience/molecular genetics -- fields completely unrelated to this topic.
Only expertise I bring to this, besides a love of data, is based on my work as a science communicator, particularly one specialized in vaccine confidence
Only expertise I bring to this, besides a love of data, is based on my work as a science communicator, particularly one specialized in vaccine confidence
(PS. lots of hot takes on this right now... anyone not clearly stating the caveats to their expertise in relation to this particular multi-dimensional subject is someone whose advice you may wanna take with a grain of salt)
Now let's dig into NACI's analyses: they assumed risk of VITT (Vaccine-induced Immune Thrombotic Thrombocytopenia) = by age & gender given lack of conclusive data to suggest otherwise.
(Because it's rare, not enough cases worldwide to be sure trends aren't confounded by rollout)
(Because it's rare, not enough cases worldwide to be sure trends aren't confounded by rollout)
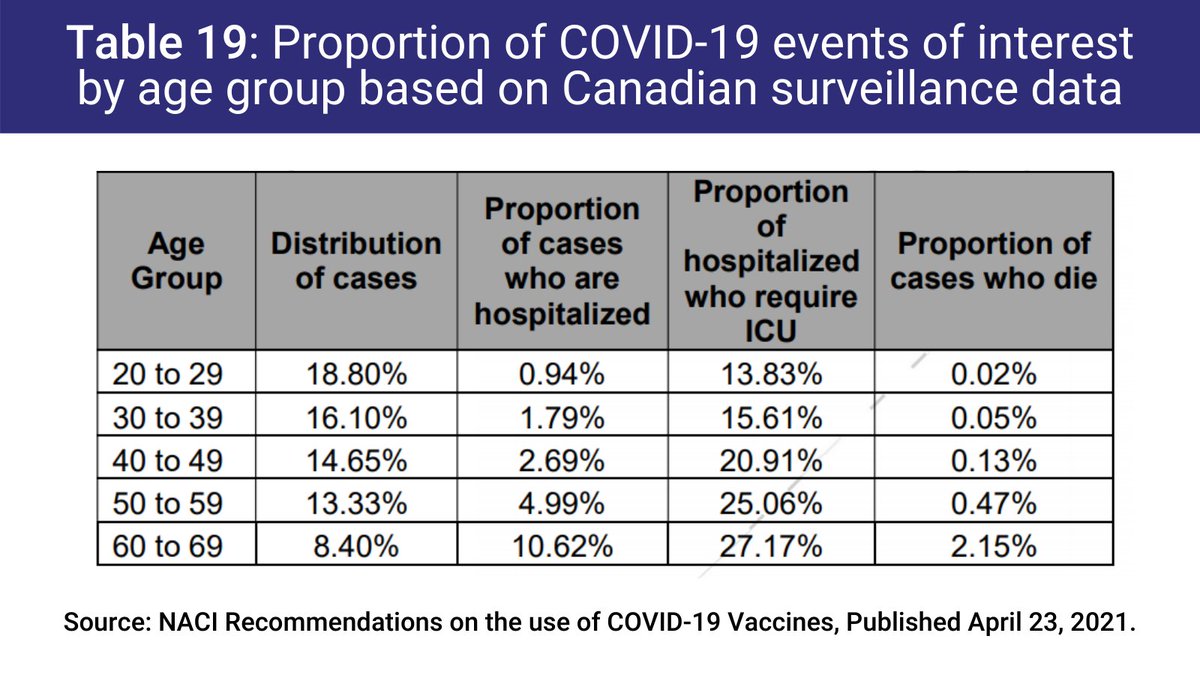
The reason they stratify risks by age in their analyses is because it is clear that the likelihood of severe outcomes from COVID-19 increase with age (see Table 19).
Though that's just looking at hospitalization, ICU admission & death from COVID... not long COVID aka PASC.
Though that's just looking at hospitalization, ICU admission & death from COVID... not long COVID aka PASC.
What about underlying conditions? Gonna reference the brilliant Dr. @MPaiMD ...
Here she states that *based on what we know so far* there are not many underlying factors that seem to make someone at higher risk of developing VITT after AstraZeneca
Here she states that *based on what we know so far* there are not many underlying factors that seem to make someone at higher risk of developing VITT after AstraZeneca
https://twitter.com/MPaiMD/status/1385751233814843396?s=20
They do a few different analyses, some assuming risk of VITT is 1 in 100,000 doses of AstraZeneca given, others assuming 1 in 250,000 doses.
I'll show the ones assuming 1 in 100,000 to play it safe, since that's closer to what our fave Dr. @MPaiMD says
I'll show the ones assuming 1 in 100,000 to play it safe, since that's closer to what our fave Dr. @MPaiMD says
https://twitter.com/MPaiMD/status/1385743156818423815?s=20
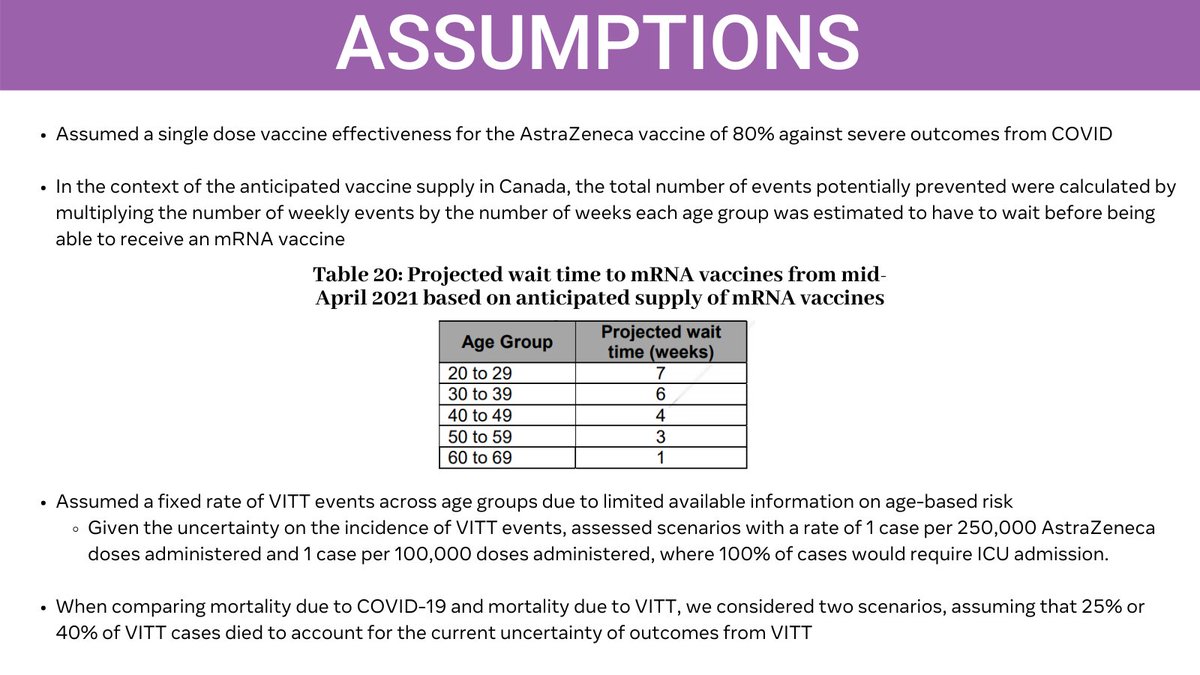
They also assumed one dose of the AstraZeneca vaccine has an effectiveness of 80% for preventing severe COVID outcomes.
This is fair based on findings from Scottish study that it can reduce risk of hospitalization by as much as 94%.
Here are some of their other assumptions.
This is fair based on findings from Scottish study that it can reduce risk of hospitalization by as much as 94%.
Here are some of their other assumptions.
I don't love how NACI's statement gives the impression the AstraZeneca vax is inferior (it is equally effective at preventing hospitalizations and deaths from COVID, even with 1 dose).
But I do like how their analyses factor in the risk of each week of waiting for an mRNA vax ⤵️
But I do like how their analyses factor in the risk of each week of waiting for an mRNA vax ⤵️

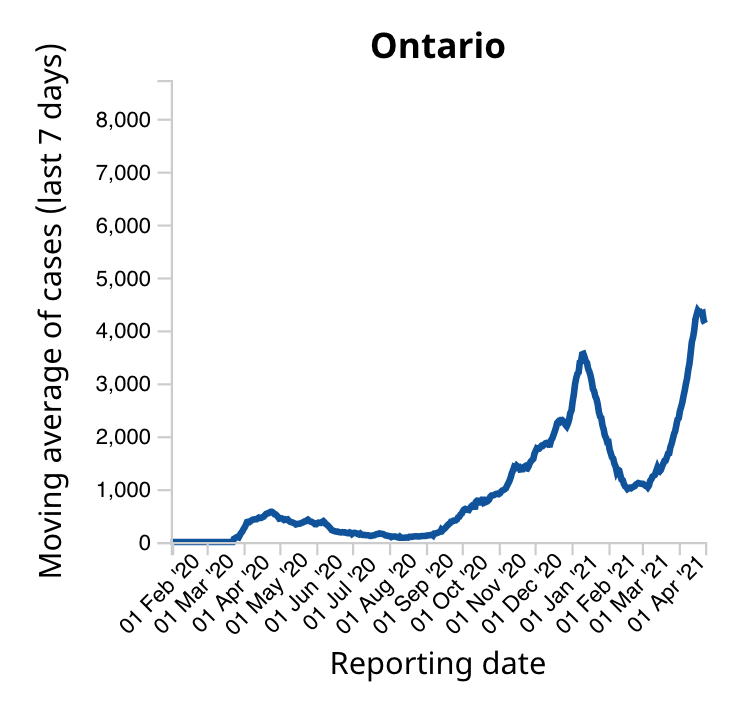
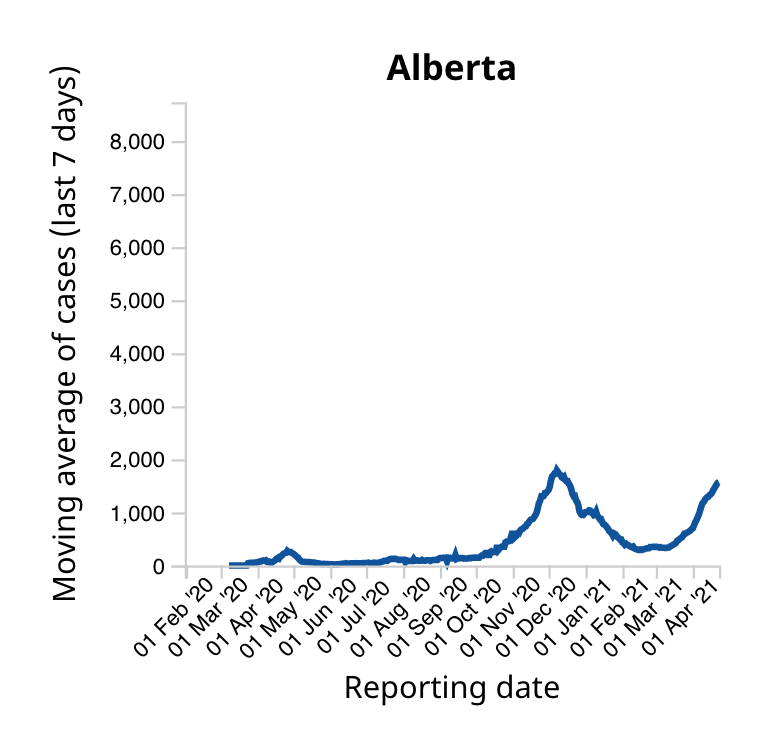
If you're in Ontario or Alberta, the conclusion from all NACI risk/benefit analyses are the same: take the 1st vax you can.
Both currently in "high" category of COVID levels with >30 new daily cases per 100k.
In ON, that's ~4371 new daily cases
In AB, it's ~1311 new daily cases
Both currently in "high" category of COVID levels with >30 new daily cases per 100k.
In ON, that's ~4371 new daily cases
In AB, it's ~1311 new daily cases
This table convinced me AZ benefits outweigh risks for any age in ON & AB ("high" COVID level).
Grey boxes = safer to get AZ vax than wait for mRNA
Note conservative variables: VITT risk (1 in 100k doses), assumes low ICU admission rate from COVID & every case of VITT -> ICU
Grey boxes = safer to get AZ vax than wait for mRNA
Note conservative variables: VITT risk (1 in 100k doses), assumes low ICU admission rate from COVID & every case of VITT -> ICU
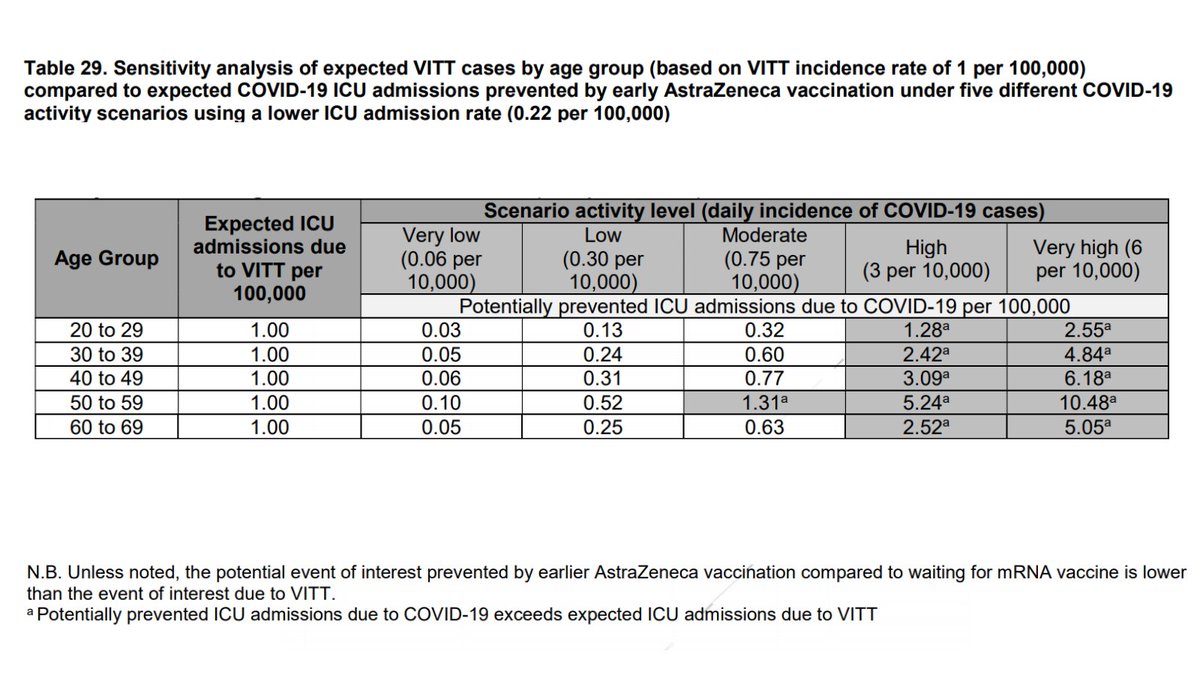
NACI analyses suggest that, even if you assume the worst of VITT and decent COVID outcomes in areas with high COVID:
For 30 to 39 year olds, the AstraZeneca vaccine could prevent 2.42 ICU admissions per 100k cases
Compared to 1 per 100k vaccinated with AZ who could get VITT.
For 30 to 39 year olds, the AstraZeneca vaccine could prevent 2.42 ICU admissions per 100k cases
Compared to 1 per 100k vaccinated with AZ who could get VITT.
For #GenXZeneca (age 40-49), the most conservative estimates from NACI suggest 1 AstraZeneca dose can prevent the 3.09 ICU admissions per 100k in high COVID areas.
Compare to 1 in 100k risk of VITT per dose.
If you recently got the AZ vax, you can feel good about that decision!
Compare to 1 in 100k risk of VITT per dose.
If you recently got the AZ vax, you can feel good about that decision!
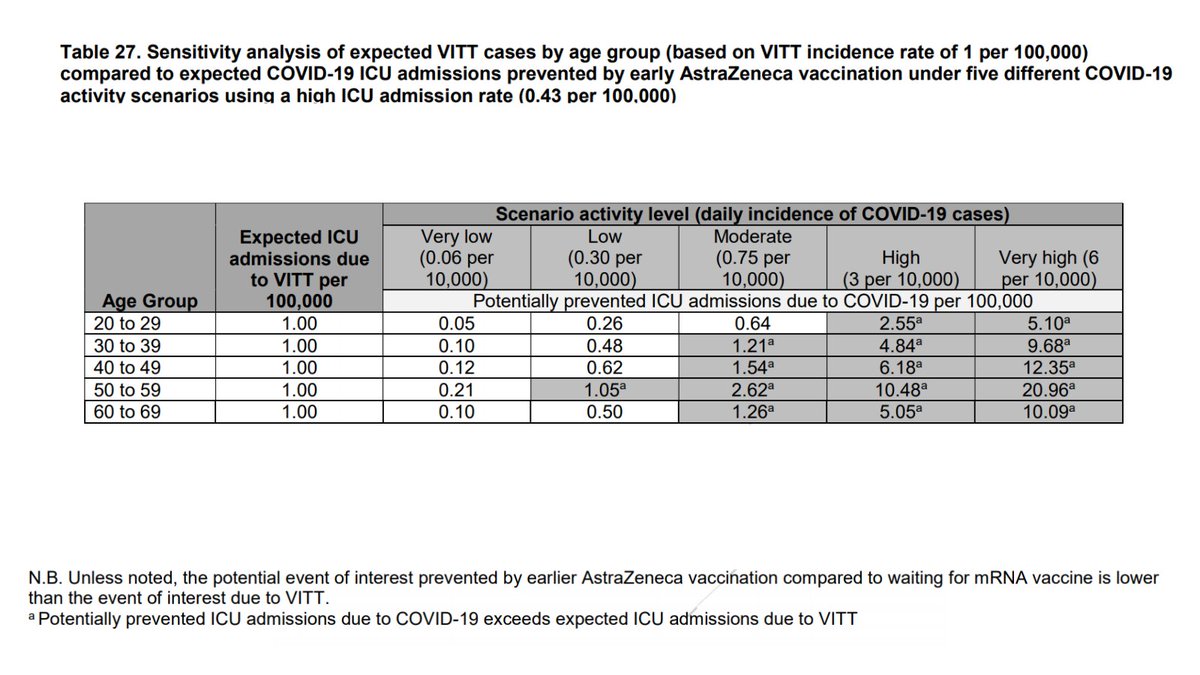
If you're somewhere with moderate levels of COVID spread (7.5 new daily cases per 100k people): the risk vs. benefit teeters depending on variables used.
But it often still tilts in favour of those 30+ getting the AstraZeneca vaccine vs. waiting for an mRNA vaccine.
But it often still tilts in favour of those 30+ getting the AstraZeneca vaccine vs. waiting for an mRNA vaccine.
For ex, keeping VITT risk @ 1 in 100k, and using slightly higher ICU admission rate from COVID (what they say is closer to recent overall rate):
1 dose of AZ offers more protection against ICU admission from COVID for 30+ than VITT risk, even @ moderate COVID levels (grey boxes)
1 dose of AZ offers more protection against ICU admission from COVID for 30+ than VITT risk, even @ moderate COVID levels (grey boxes)
When you factor in that VITT is treatable (4/5 cases in Canada reportedly recovering at home), and that outcomes are probably better now that we've learned more about it...
I think offering the AstraZeneca vaccine to those 30+ makes sense, even in areas with moderate COVID risk.
I think offering the AstraZeneca vaccine to those 30+ makes sense, even in areas with moderate COVID risk.
Internationally, regulatory agencies in UK and Europe have reached similar conclusions as NACI.
See this summary of the EMA's conclusions this week on the AstraZeneca (aka Vaxzevria) vaccine from the wonderful @kakape
See this summary of the EMA's conclusions this week on the AstraZeneca (aka Vaxzevria) vaccine from the wonderful @kakape
https://twitter.com/kakape/status/1385597115037061120?s=20
While NACI hasn't made statements on the Janssen J&J vaccine yet, here's the decision on that from the US.
Note both AstraZeneca and Janssen J&J use adenovirus vector, but unclear to what extent risks & mechanisms of clots following each vax are the same.
Note both AstraZeneca and Janssen J&J use adenovirus vector, but unclear to what extent risks & mechanisms of clots following each vax are the same.
https://twitter.com/kakape/status/1385697164484034562?s=20
CAVEAT: these are my interpretations of the NACI statement, as it currently stands April 24 at 2pm.
I am a scientist so I am comfortable reading and interpreting data, but this is not my area of trained expertise so I speak to you here as a communicator, not expert.
I am a scientist so I am comfortable reading and interpreting data, but this is not my area of trained expertise so I speak to you here as a communicator, not expert.
If you'd like to hear from a subject matter expert on clots, please check out this thread from the brilliant @MPaiMD.
This is a Dr. Menaka Pai stan account. She's the best (& lead author of @COVIDSciOntario's summaries on this topic, which are also great)
This is a Dr. Menaka Pai stan account. She's the best (& lead author of @COVIDSciOntario's summaries on this topic, which are also great)
https://twitter.com/MPaiMD/status/1385741537221480449?s=20
And here's a summary of what infectious disease expert Dr. Allison McGeer had to say about the benefits vs. risks of the AstraZeneca vaccine
(TL;DR -- if you're in Ontario or AB, take whatever vaccine you can ASAP).
(TL;DR -- if you're in Ontario or AB, take whatever vaccine you can ASAP).
https://twitter.com/maureentaylor31/status/1385694570294521862?s=20
For what it's worth, it is not my job to convince anyone to take any vaccine ever.
But I do see it as my job as a science communicator to make navigating the evidence to help with this decision a little easier.
But I do see it as my job as a science communicator to make navigating the evidence to help with this decision a little easier.
And regardless where you get your info from, always good to discuss your personal health concerns with your doctor since they know the full scope of your medical history 💗
If you want to share this with people not on Twitter, I compiled everything in this thread on @Medium here:
heysciencesam.medium.com/the-protection…
heysciencesam.medium.com/the-protection…
• • •
Missing some Tweet in this thread? You can try to
force a refresh