[May 9] Details of the local cases
1-4. Case 62873 (Changi T3) cluster
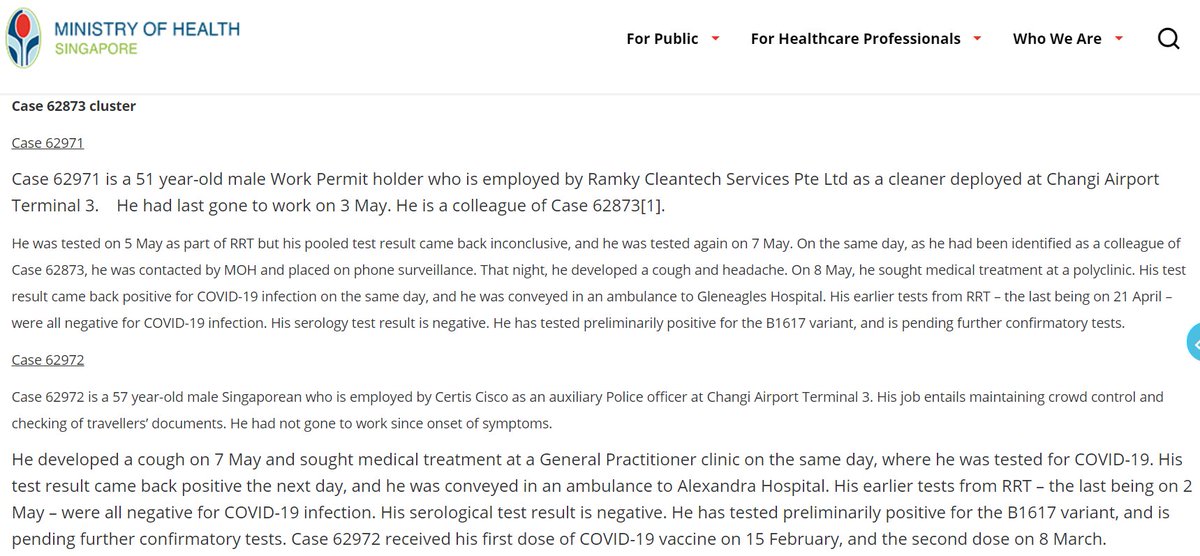
62971: Colleague of Case 62873
62972: Auxilliary police officer at T3
63015: Colleague of Case 62873
63026: Passenger escort at T3
Cases 62940, 62942, 62945 from May 8 reclassified from unlinked to linked.
1-4. Case 62873 (Changi T3) cluster
62971: Colleague of Case 62873
62972: Auxilliary police officer at T3
63015: Colleague of Case 62873
63026: Passenger escort at T3
Cases 62940, 62942, 62945 from May 8 reclassified from unlinked to linked.


5-7. TTSH cluster
Cases 63007, 63008, 63009 are patients who had been warded in Ward 9D (where most of the cases are linked to).
Current size: 43.
Variant involved: B.1.617.2.
Cases 63007, 63008, 63009 are patients who had been warded in Ward 9D (where most of the cases are linked to).
Current size: 43.
Variant involved: B.1.617.2.

8. Case 62969
Grab driver. Dev'd symptoms on May 7, got tested on the same day. 👍
Resides with his girlfriend who arrived from Vietnam on Apr 12, served SHN until Apr 26. Vietnam is low-risk, though. Infected in quarantine? May need to test her again.
Variant: B.1.617.
Grab driver. Dev'd symptoms on May 7, got tested on the same day. 👍
Resides with his girlfriend who arrived from Vietnam on Apr 12, served SHN until Apr 26. Vietnam is low-risk, though. Infected in quarantine? May need to test her again.
Variant: B.1.617.

9. Case 62998
WFH from Apr 30. Symptoms on May 7, got tested on the same day. 👍
Variant: B.1.617.
10. Case 63005
Landscaper at National Parks. Symptoms on May 6 night, got tested on May 7. 👍
Partially vaccinated (1st dose on Apr 23).
WFH from Apr 30. Symptoms on May 7, got tested on the same day. 👍
Variant: B.1.617.
10. Case 63005
Landscaper at National Parks. Symptoms on May 6 night, got tested on May 7. 👍
Partially vaccinated (1st dose on Apr 23).

Singapore ATB index (daily average of unlinked community cases in the past week) as of May 9: 1.29.
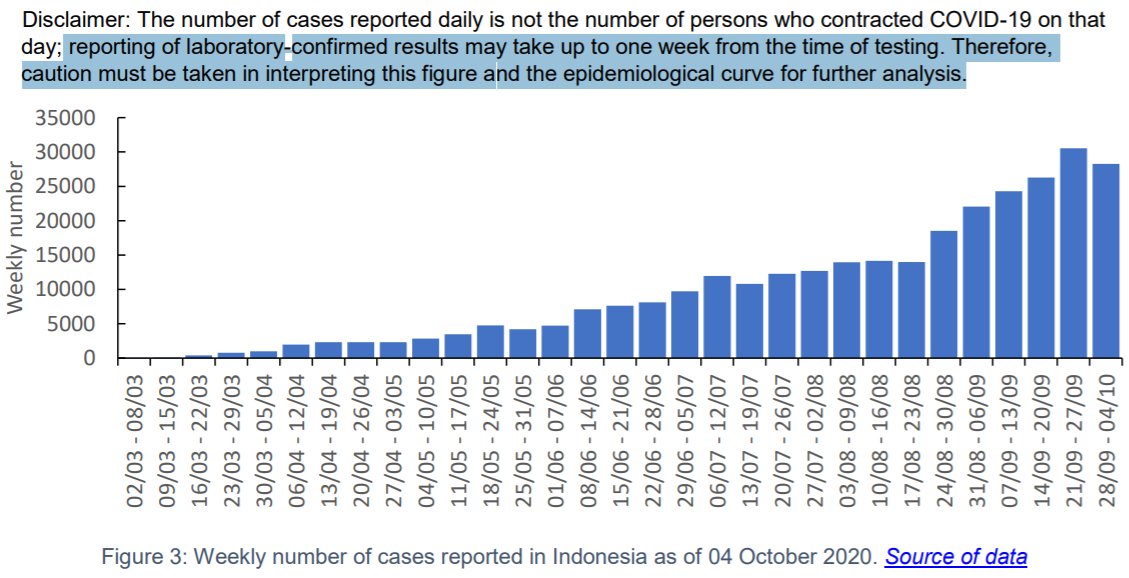
Several cases working in Changi Airport Terminal 3 were reclassified from unlinked to linked as they formed a new cluster linked to visits to T3 B2.
caas.gov.sg/who-we-are/new…
Several cases working in Changi Airport Terminal 3 were reclassified from unlinked to linked as they formed a new cluster linked to visits to T3 B2.
caas.gov.sg/who-we-are/new…

Almost 900 quarantine orders generated on May 8.
Really concerning: More random cases in the community with no clear link to frontliners & the circulating variant is B.1.617.
The only silver lining is all these cases got tested immediately after they developed symptoms. V impt!
Really concerning: More random cases in the community with no clear link to frontliners & the circulating variant is B.1.617.
The only silver lining is all these cases got tested immediately after they developed symptoms. V impt!

Variants involved in active clusters in Singapore as of May 9:
- B.1.617: 5 clusters (size: 43, 11, 8, 4, 4)
- B.1.351: 3 (size: 8, 7, 6)
- P.1: 1 (size: 5)
- B.1.525: 1 (size: 3)
- ?: 1 (size: 4)
All clusters could be traced to known imported case/exposure except TTSH cluster.
- B.1.617: 5 clusters (size: 43, 11, 8, 4, 4)
- B.1.351: 3 (size: 8, 7, 6)
- P.1: 1 (size: 5)
- B.1.525: 1 (size: 3)
- ?: 1 (size: 4)
All clusters could be traced to known imported case/exposure except TTSH cluster.


Changi staff cluster.
Four cases work for the same company. Link to the other cases is through same visited outlets in Terminal 3 Basement 2. Prime candidate would be the food court in T3 B2 where masks are off during eating/drinking.
caas.gov.sg/who-we-are/new…
#COVIDisAirborne
Four cases work for the same company. Link to the other cases is through same visited outlets in Terminal 3 Basement 2. Prime candidate would be the food court in T3 B2 where masks are off during eating/drinking.
caas.gov.sg/who-we-are/new…
#COVIDisAirborne



Singapore reported 19 #COVID19 cases on May 10.
- 16 imported cases (4🇮🇳🇮🇩 2🇯🇵 1🇭🇰🇲🇾🇳🇵🇵🇬🇵🇭🇦🇪)
- 3 local cases (2 linked, 1 unlinked)
Total: 61,378
Discharged: 60,953 (+20)
Isolation facilities: 259 (-3)
Hospitalized: 135 (+1)
ICU: 3 (+1) 😰😰
Deaths: 31
moh.gov.sg/news-highlight…
- 16 imported cases (4🇮🇳🇮🇩 2🇯🇵 1🇭🇰🇲🇾🇳🇵🇵🇬🇵🇭🇦🇪)
- 3 local cases (2 linked, 1 unlinked)
Total: 61,378
Discharged: 60,953 (+20)
Isolation facilities: 259 (-3)
Hospitalized: 135 (+1)
ICU: 3 (+1) 😰😰
Deaths: 31
moh.gov.sg/news-highlight…




[May 10] Details of local cases
1. Case 63037. Chef at MOS Burger Suntec City. Asymptomatic, tested in NTFGH during a visit for unrelated condition.
Another random case with no link yet to frontliners/other cases. There are definitely more cases like this now in the community.
1. Case 63037. Chef at MOS Burger Suntec City. Asymptomatic, tested in NTFGH during a visit for unrelated condition.
Another random case with no link yet to frontliners/other cases. There are definitely more cases like this now in the community.

2-3. Changi T3 cluster
Case 63047: Staff at Raffles Medical at Changi T3.
Case 63055: Security officer at Changi T3.
Both are fully vaccinated, symptomatic.
Current size: 10 (8 fully vax'd, 2 not vax'd; vax rate among aviation workers: 92%).
Variant involved: B.1.617.
Case 63047: Staff at Raffles Medical at Changi T3.
Case 63055: Security officer at Changi T3.
Both are fully vaccinated, symptomatic.
Current size: 10 (8 fully vax'd, 2 not vax'd; vax rate among aviation workers: 92%).
Variant involved: B.1.617.

Reclassification of cases on May 10 (MOH published this list on its situation report every Monday).

Singapore ATB index (daily average of unlinked community cases in the past week) as of May 10: 1.43.

572 quarantine orders were generated on May 9.
(The numbers for May 10 are not final yet.)
(The numbers for May 10 are not final yet.)

🇸🇬 vaccination as of May 9
- 1st dose: 1.8m (31.6% pop)
- Completed regimen: 1.2m (21.1% pop)
Average daily doses administered from the last update (Apr 18):
- 1st dose: 20,756 (0.36 per 100 pop)
- 2nd dose: 16,678 (0.29 per 100 pop)
- 1st dose: 1.8m (31.6% pop)
- Completed regimen: 1.2m (21.1% pop)
Average daily doses administered from the last update (Apr 18):
- 1st dose: 20,756 (0.36 per 100 pop)
- 2nd dose: 16,678 (0.29 per 100 pop)

Complete text of Minister of Health's speech in Parliament today: moh.gov.sg/news-highlight…
Among other things, Pfizer-BnT has submitted data to HSA 🇸🇬 for approval to use in kids aged 12-15.
(Anyway, it will take a few more months to get into this age group, probably end of Q3.)
Among other things, Pfizer-BnT has submitted data to HSA 🇸🇬 for approval to use in kids aged 12-15.
(Anyway, it will take a few more months to get into this age group, probably end of Q3.)

As of May 3, 104 applications for Vaccine Injury Financial Assistance Programme have been received.
75 have been processed with 30 accepted:
- 21 allergic reactions
- 4 neurology-related
- 3 cardiology-related
- 1 haematology case
- 1 dermatology case
(out of 3 million doses)
75 have been processed with 30 accepted:
- 21 allergic reactions
- 4 neurology-related
- 3 cardiology-related
- 1 haematology case
- 1 dermatology case
(out of 3 million doses)

Breakthrough infections as of May 10:
- Local: 30 (the settings of recent/ongoing outbreaks are in the frontlines -- hospital, airport, seaport)
- Imported: 24
- Most are asymptomatic, no severe case yet
Re-infection cases: 26 (imported 20, local 6 from MOH Situation Report).
- Local: 30 (the settings of recent/ongoing outbreaks are in the frontlines -- hospital, airport, seaport)
- Imported: 24
- Most are asymptomatic, no severe case yet
Re-infection cases: 26 (imported 20, local 6 from MOH Situation Report).

Numbers of swabs tested (May 4-10): 535,005 (76,429/day).
Singapore has more than doubled its testing rate within 2 weeks of the new wave of local cases.
Singapore has more than doubled its testing rate within 2 weeks of the new wave of local cases.

Singapore reported 25 #COVID19 cases on May 11.
- 13 local cases (10 linked, 3 unlinked)
- 12 imported cases (4🇮🇳 3🇮🇩 1🇯🇵🇲🇾🇵🇭🇱🇰🇬🇧)
Total: 61,403
Discharged: 60,975 (+22)
Isolation facilities: 253 (-6)
Hospitalized: 144 (+9)
ICU: 3
Deaths: 31
moh.gov.sg/news-highlight…
- 13 local cases (10 linked, 3 unlinked)
- 12 imported cases (4🇮🇳 3🇮🇩 1🇯🇵🇲🇾🇵🇭🇱🇰🇬🇧)
Total: 61,403
Discharged: 60,975 (+22)
Isolation facilities: 253 (-6)
Hospitalized: 144 (+9)
ICU: 3
Deaths: 31
moh.gov.sg/news-highlight…




[May 11] Details of local cases
1. Case 63068: Manufacturing operator at Siltronic.
Dev'd symptoms on May 6, went to GP and was given MC for 2 days, more symptoms on May 8, went to another GP and got tested on May 9, confirmed on May 10.
Yet another case with unknown source.
1. Case 63068: Manufacturing operator at Siltronic.
Dev'd symptoms on May 6, went to GP and was given MC for 2 days, more symptoms on May 8, went to another GP and got tested on May 9, confirmed on May 10.
Yet another case with unknown source.

2. Case 63069: IT support at Kulicke & Soffa, part-time barista at Starbucks Plaza Singapura & worker at LBC Express @ Lucky Plaza.
Dev'd symptoms on May 6 but still went to work 😥, went to GP on May 8 night, tested on May 9, confirmed on May 10.
Partially vaccinated.
Dev'd symptoms on May 6 but still went to work 😥, went to GP on May 8 night, tested on May 9, confirmed on May 10.
Partially vaccinated.

3. Case 63073: OT technician at Ng Teng Fong General Hospital.
Dev'd symptoms on Apr 21, tested on... May 10. 😩
High Ct, serology +ve (well it's really long since onset), had travel history in late Jan. Fingers crossed this is a long Covid case shedding fragments of the virus.
Dev'd symptoms on Apr 21, tested on... May 10. 😩
High Ct, serology +ve (well it's really long since onset), had travel history in late Jan. Fingers crossed this is a long Covid case shedding fragments of the virus.

4. Case 63083: Close contact of Case 62969 (Grab driver). Fully vaccinated.
5. Case 63084: Close contact of Case 63005 (NParks landscaper).
6. Case 63078: Bunker tanker crew cluster (current size: 7).
All had been placed and detected in quarantine.
5. Case 63084: Close contact of Case 63005 (NParks landscaper).
6. Case 63078: Bunker tanker crew cluster (current size: 7).
All had been placed and detected in quarantine.

7-13. Changi T3 cluster
63059: Cleaner at T3. Vax'd.
63060: Spouse of 62945
63061: Contact of 62971. Vax'd.
63070: Cleaner at Kopitiam T3
63071: Cleaner at the same company with T3 cluster but deployed elsewhere
63072: Maintenance staff at T3. Vax'd.
63074: Contact of 63055
63059: Cleaner at T3. Vax'd.
63060: Spouse of 62945
63061: Contact of 62971. Vax'd.
63070: Cleaner at Kopitiam T3
63071: Cleaner at the same company with T3 cluster but deployed elsewhere
63072: Maintenance staff at T3. Vax'd.
63074: Contact of 63055




Case solved
Case 62941 (VJC student) who is previously an unlinked case is now linked to Changi T3 cluster. She visited Kopitiam T3 on May 3 at the same time when Case 62942 and 62945 were there.
Current size: 18
Variant involved: B.1.617.?
#COVIDisAirborne
Case 62941 (VJC student) who is previously an unlinked case is now linked to Changi T3 cluster. She visited Kopitiam T3 on May 3 at the same time when Case 62942 and 62945 were there.
Current size: 18
Variant involved: B.1.617.?
#COVIDisAirborne

Singapore ATB index (daily average of unlinked community cases in the past week) as of May 11: 1.71.
What's really concerning is the number of unlinked cases with no link to the frontlines and no recent travel history continue to increase. We are indeed on knife's edge now.
What's really concerning is the number of unlinked cases with no link to the frontlines and no recent travel history continue to increase. We are indeed on knife's edge now.

🇸🇬 vaccination as of May 10
- 1st dose: 1,852,684 (32.5% pop)
- Completed regimen: 1,284,646 (22.5% pop)
Average daily doses administered from the last update (Apr 18):
- 1st dose: 22,207 (0.39 per 100 pop)
- 2nd dose: 19,767 (0.35 per 100 pop)
moh.gov.sg/covid-19/vacci…
- 1st dose: 1,852,684 (32.5% pop)
- Completed regimen: 1,284,646 (22.5% pop)
Average daily doses administered from the last update (Apr 18):
- 1st dose: 22,207 (0.39 per 100 pop)
- 2nd dose: 19,767 (0.35 per 100 pop)
moh.gov.sg/covid-19/vacci…

Singapore reported 16 #COVID19 cases on May 12.
- 10 local cases (9 linked, 1 unlinked)
- 6 imported cases
Total: 61,419
Discharged: 61,006 (+31)
Isolation facilities: 239 (-14)
Hospitalized: 143 (-1)
ICU: 3
Deaths: 31
moh.gov.sg/news-highlight…
- 10 local cases (9 linked, 1 unlinked)
- 6 imported cases
Total: 61,419
Discharged: 61,006 (+31)
Isolation facilities: 239 (-14)
Hospitalized: 143 (-1)
ICU: 3
Deaths: 31
moh.gov.sg/news-highlight…




[May 12] Details of local cases
1. Case 63096
OT nurse in SKH. Symptoms on May 9 night, tested on May 10, confirmed on May 11.
Fully vaccinated.
Variant: B.1.617.
1. Case 63096
OT nurse in SKH. Symptoms on May 9 night, tested on May 10, confirmed on May 11.
Fully vaccinated.
Variant: B.1.617.

2. Case 63092
Contact of Cases 62969 and 63083. Recent travel history from Vietnam.
Placed on and detected in quarantine.
Formed a new cluster. Variant involved: B.1.617.
Contact of Cases 62969 and 63083. Recent travel history from Vietnam.
Placed on and detected in quarantine.
Formed a new cluster. Variant involved: B.1.617.

3-9. Changi T3 cluster
63091: IT engineer at T4, visited T3.
63094: ICA officer at T3. Vax'd.
63095: ICA officer at T3. Vax'd.
63097: Cleaner at T3. Vax'd.
63098: Security officer at T3.
63100: Cleaner at T3. Vax'd.
63019: Retail staff at T3. Vax'd.
#COVIDisAirborne
63091: IT engineer at T4, visited T3.
63094: ICA officer at T3. Vax'd.
63095: ICA officer at T3. Vax'd.
63097: Cleaner at T3. Vax'd.
63098: Security officer at T3.
63100: Cleaner at T3. Vax'd.
63019: Retail staff at T3. Vax'd.
#COVIDisAirborne




10. TTSH cluster
Case 63104: patient who had been warded in Ward 9D from 26 April. Placed on and detected in quarantine.
Current size: 44 (27 patients, 10 HCWs, 7 visitors)
Variant involved: B.1.617.2
Case 63104: patient who had been warded in Ward 9D from 26 April. Placed on and detected in quarantine.
Current size: 44 (27 patients, 10 HCWs, 7 visitors)
Variant involved: B.1.617.2

[Mystery case solved]
Case 63005 who is previously unlinked has been linked to Changi T3 cluster as he had visited the same locations as Case 62940, 62942.
PSA: ALL MEMBERS OF THE PUBLIC WHO HAD VISITED CHANGI AIRPORT T3 FROM MAY 3, PLEASE GET YOURSELF TESTED.
#COVIDisAirborne
Case 63005 who is previously unlinked has been linked to Changi T3 cluster as he had visited the same locations as Case 62940, 62942.
PSA: ALL MEMBERS OF THE PUBLIC WHO HAD VISITED CHANGI AIRPORT T3 FROM MAY 3, PLEASE GET YOURSELF TESTED.
#COVIDisAirborne

Singapore ATB index (daily average of unlinked community cases in the past week) as of May 12: 1.71.
Changi T3 cluster is a big deal. Setting of the outbreak is where the vast majority of the staff have been vaccinated and are still routinely tested, and yet it still explodes.
Changi T3 cluster is a big deal. Setting of the outbreak is where the vast majority of the staff have been vaccinated and are still routinely tested, and yet it still explodes.

Changi T3 cluster as of May 12:
- Variant: B.1.617.?
- (20-21)/25 are aviation workers
- 15 vax'd, 5-6 not vax'd
- 92% of aviation workers have been vaccinated (Pfizer-BioNTech)
- Estimated efficacy based on this tiny sample size: 74-78%
Visited Changi T3 recently? Get tested!
- Variant: B.1.617.?
- (20-21)/25 are aviation workers
- 15 vax'd, 5-6 not vax'd
- 92% of aviation workers have been vaccinated (Pfizer-BioNTech)
- Estimated efficacy based on this tiny sample size: 74-78%
Visited Changi T3 recently? Get tested!

Singapore reported 34 #COVID19 cases on May 13.
- 24 local cases (20 linked, 4 unlinked)
- 10 imported cases
Total: 61,453
Discharged: 61,029 (+23)
Isolation facilities: 243 (+4)
Hospitalized: 150 (+7)
ICU: 3
Deaths: 31
#StayHome, Singapore, #StayHome.
moh.gov.sg/news-highlight…
- 24 local cases (20 linked, 4 unlinked)
- 10 imported cases
Total: 61,453
Discharged: 61,029 (+23)
Isolation facilities: 243 (+4)
Hospitalized: 150 (+7)
ICU: 3
Deaths: 31
#StayHome, Singapore, #StayHome.
moh.gov.sg/news-highlight…




[May 13] Details of the local cases
1. 63120: Homemaker. Symptoms on May 7, but only got tested on May 11.
2. 63127: FDW. Symptoms on May 7, but only sought treatment on May 10 and tested on May 11.
Both are mystery cases.
1. 63120: Homemaker. Symptoms on May 7, but only got tested on May 11.
2. 63127: FDW. Symptoms on May 7, but only sought treatment on May 10 and tested on May 11.
Both are mystery cases.

3. 63131: Tutor at Learning Point. Symptoms on May 3, but only got tested on... wait for it... May 11. 😩
4. 63147: FDW. Symptoms on May 8, sought treatment immediately but not tested (why arh?), went back to the same GP on May 12 and finally got tested.
Both are mystery cases.
4. 63147: FDW. Symptoms on May 8, sought treatment immediately but not tested (why arh?), went back to the same GP on May 12 and finally got tested.
Both are mystery cases.

5. 63122: Student at Yio Chu Kang Primary School. Contact of 63096 (SKH nurse).
Symptoms on May 10 night, got tested immediately on May 11. 👍
Symptoms on May 10 night, got tested immediately on May 11. 👍

6-24. Changi T3 cluster
Breakdown: 9 staff, 7 contacts, 2 visitors, 1 unclear
Total (46): 29 staff, 12 contacts, 4 visitors, 1 unclear
Among staff (92% vaccinated): 20 vax'd, 9 non vax'd (efficacy: ~80%)
PSA: PLEASE GET TESTED IF YOU HAD VISITED CHANGI FROM MAY 1 ONWARDS.
Breakdown: 9 staff, 7 contacts, 2 visitors, 1 unclear
Total (46): 29 staff, 12 contacts, 4 visitors, 1 unclear
Among staff (92% vaccinated): 20 vax'd, 9 non vax'd (efficacy: ~80%)
PSA: PLEASE GET TESTED IF YOU HAD VISITED CHANGI FROM MAY 1 ONWARDS.



Singapore ATB index (daily average of unlinked community cases in the past week) as of May 13: 2.14.
The details are depressing with mystery cases of homemaker and FDWs who mostly stayed at home. We are dealing with a very nasty variant which transmits really easily.
The details are depressing with mystery cases of homemaker and FDWs who mostly stayed at home. We are dealing with a very nasty variant which transmits really easily.

Timeline of Changi T3 cluster as of May 13.
Breakdown: 29 staff, 12 contacts, 4 visitors, 1 unclear (staff?)
Among staff (92% of all aviation workers have been vaccinated): 20-21 vax'd, 9 not vax'd (efficacy: ~80%)
PSA: PLEASE GET TESTED IF YOU HAD VISITED CHANGI FROM MAY 1.
Breakdown: 29 staff, 12 contacts, 4 visitors, 1 unclear (staff?)
Among staff (92% of all aviation workers have been vaccinated): 20-21 vax'd, 9 not vax'd (efficacy: ~80%)
PSA: PLEASE GET TESTED IF YOU HAD VISITED CHANGI FROM MAY 1.

Variants involved in active clusters in Singapore as of May 13:
- B.1.617: 6 clusters (size: 46, 44, 11, 4, 4, 3)
- B.1.351: 3 (size: 8, 7, 7)
- P.1: 1 (size: 5)
- B.1.525: 1 (size: 3)
Best policy to deal with B.1.617.2 subvariant: Stop it at the border. Don't try this at home.
- B.1.617: 6 clusters (size: 46, 44, 11, 4, 4, 3)
- B.1.351: 3 (size: 8, 7, 7)
- P.1: 1 (size: 5)
- B.1.525: 1 (size: 3)
Best policy to deal with B.1.617.2 subvariant: Stop it at the border. Don't try this at home.


Cases with unknown source are bad but some are worse than others. Worst type is mystery cases without any link to the frontline (airport/seaport/quarantine facility) or travel history. The list grows faster recently and there are more of these still undetected now.

Singapore reported 52 #COVID19 cases on May 14.
- 28 imported cases
- 24 local cases (20 linked, 4 unlinked)
Total: 61,505
Discharged: 61,047 (+18)
Isolation facilities: 247 (+4)
Hospitalized: 180 (+30)
ICU: 3
Deaths: 31
moh.gov.sg/news-highlight…
- 28 imported cases
- 24 local cases (20 linked, 4 unlinked)
Total: 61,505
Discharged: 61,047 (+18)
Isolation facilities: 247 (+4)
Hospitalized: 180 (+30)
ICU: 3
Deaths: 31
moh.gov.sg/news-highlight…




[May 14] Details of local cases
1. 63160: Chef at Changi Prison. Symptoms on May 12, got tested immediately. Fully vaccinated.
2. 63166: Cook at Wok Hey White Sands. Symptoms on May 10, got tested on May 11.
Both are mystery cases, but work in East area. Linked to Changi?
1. 63160: Chef at Changi Prison. Symptoms on May 12, got tested immediately. Fully vaccinated.
2. 63166: Cook at Wok Hey White Sands. Symptoms on May 10, got tested on May 11.
Both are mystery cases, but work in East area. Linked to Changi?

3. 63183: A retiree. Symptoms on May 10, got tested on May 11.
4. 63220: GrabFood rider. Symptoms on May 12 night, got tested on May 13.
Both are mystery cases as well.
4. 63220: GrabFood rider. Symptoms on May 12 night, got tested on May 13.
Both are mystery cases as well.

5-9. Case 63131 (tutor) cluster
All attended the tutor's classes at Learning Point Parkway Centre (another one in the East).
63184: St Stephen's
63185: Kong Hwa
63186: St Andrew's Junior
63187: Kong Hwa
63188: St Stephen's
Symptoms on May 11/12, quarantined on May 12.
All attended the tutor's classes at Learning Point Parkway Centre (another one in the East).
63184: St Stephen's
63185: Kong Hwa
63186: St Andrew's Junior
63187: Kong Hwa
63188: St Stephen's
Symptoms on May 11/12, quarantined on May 12.

10. Case 63096 (SKH nurse) cluster
63221: Household contact of 63096. Placed on and detected in quarantine. Fully vaccinated, asymptomatic.
11. TTSH cluster
63168: Patient who had been warded in Ward 9D (where most cases in this cluster are linked to).
63221: Household contact of 63096. Placed on and detected in quarantine. Fully vaccinated, asymptomatic.
11. TTSH cluster
63168: Patient who had been warded in Ward 9D (where most cases in this cluster are linked to).

12-24. Changi T3 cluster
Today (13): 6 staff, 7 contacts
To date (59): 35 staff, 19 contacts, 5 visitors
Among staff (92% aviation workers are vaccinated): 25 vax'd, 10 not vax'd (efficacy: ~78%)
PSA: PLEASE GET TESTED IF YOU HAD VISITED CHANGI FROM MAY 1 ONWARDS.
Today (13): 6 staff, 7 contacts
To date (59): 35 staff, 19 contacts, 5 visitors
Among staff (92% aviation workers are vaccinated): 25 vax'd, 10 not vax'd (efficacy: ~78%)
PSA: PLEASE GET TESTED IF YOU HAD VISITED CHANGI FROM MAY 1 ONWARDS.


Daily average of unlinked community cases in the past week as of May 14: 2.29.
- The mystery cases are more concentrated in the East; link to Changi?
- Yesterday = public holiday so testing would be less as many GPs closed. Tomorrow = better idea of unlinked cases.
#StayHome
- The mystery cases are more concentrated in the East; link to Changi?
- Yesterday = public holiday so testing would be less as many GPs closed. Tomorrow = better idea of unlinked cases.
#StayHome

Timeline of Changi T3 cluster as of May 14.
Breakdown: 35 staff, 19 contacts, 5 visitors
Among staff (92% aviation workers are vaccinated): 25 vax'd, 10 not vax'd (efficacy: ~78%)
PSA: PLEASE GET TESTED IF YOU HAD VISITED CHANGI FROM MAY 1.
Table: docs.google.com/spreadsheets/d…
Breakdown: 35 staff, 19 contacts, 5 visitors
Among staff (92% aviation workers are vaccinated): 25 vax'd, 10 not vax'd (efficacy: ~78%)
PSA: PLEASE GET TESTED IF YOU HAD VISITED CHANGI FROM MAY 1.
Table: docs.google.com/spreadsheets/d…

Singapore reported 31 #COVID19 cases on May 15.
- 19 local cases (17 linked, 2 unlinked)
- 12 imported cases
Total: 61,536
Discharged: 61,062 (+15)
Isolation facilities: 253 (+6)
Hospitalized: 190 (+10)
ICU: 3
Deaths: 31
moh.gov.sg/news-highlight…
- 19 local cases (17 linked, 2 unlinked)
- 12 imported cases
Total: 61,536
Discharged: 61,062 (+15)
Isolation facilities: 253 (+6)
Hospitalized: 190 (+10)
ICU: 3
Deaths: 31
moh.gov.sg/news-highlight…




[May 15] Details of local cases
1. 62236: Personal chauffeur. Symptoms on May 12, tested on May 13. Positive for B.1.617.
2. 63237: Currently unemployed. Symptoms on May 12, tested on May 13. First dose of vaccine on May 10.
Both are mystery cases.
1. 62236: Personal chauffeur. Symptoms on May 12, tested on May 13. Positive for B.1.617.
2. 63237: Currently unemployed. Symptoms on May 12, tested on May 13. First dose of vaccine on May 10.
Both are mystery cases.

3. 63241: Homemaker. Family member of 63166 (cook at Wok Hey White Sands). Symptoms on May 12, quarantined and tested on May 13.
4. 63249: Retiree. Family member of 63183 (also a retiree). Symptoms on May 6, quarantined and tested on May 13 after identified as her close contact.
4. 63249: Retiree. Family member of 63183 (also a retiree). Symptoms on May 6, quarantined and tested on May 13 after identified as her close contact.

5. 63253: Inmate at Changi Prison. Contact of 63160 (chef at Changi Prison, who developed symptoms on May 12). Quarantined and tested on May 13. Asymptomatic.

6-8. Case 63131 (tutor) cluster
63251: Family member of 63187 (1 of the students in the tuition centre). Placed on, detected in quarantine.
63259, 63268: Siblings, students at St Andrew's Jr. Same school bus as 63186 (1 of the students). Symptoms on May 13/14, tested on May 14.
63251: Family member of 63187 (1 of the students in the tuition centre). Placed on, detected in quarantine.
63259, 63268: Siblings, students at St Andrew's Jr. Same school bus as 63186 (1 of the students). Symptoms on May 13/14, tested on May 14.

9-10. Case 63096 (SKH nurse) cluster
63256: Student at Palm View Primary.
63257: Student at YCK Primary.
Both are classmates of 63122 (household contact of 63096) at a tuition centre in Hougang. 63257 is also 63122's schoolmate.
Both were placed on and detected in quarantine.
63256: Student at Palm View Primary.
63257: Student at YCK Primary.
Both are classmates of 63122 (household contact of 63096) at a tuition centre in Hougang. 63257 is also 63122's schoolmate.
Both were placed on and detected in quarantine.

11. TTSH cluster
63248: Patient who had been warded in Ward 9D (where almost all of the cases in this cluster are directly linked to).
Current size of the cluster: 46 (29 patients, 10 HCWs, 7 visitors).
63248: Patient who had been warded in Ward 9D (where almost all of the cases in this cluster are directly linked to).
Current size of the cluster: 46 (29 patients, 10 HCWs, 7 visitors).

12-19. Changi T3 cluster
Today: 2 staff, 6 contacts
To date (68): 37 staff, 25 contacts, 5 visitors, 1 phylogenetically linked
Among staff (92% aviation workers are vaccinated): 26 vax'd, 11 not vax'd (efficacy: ~79%)
PSA: Please get tested if you had visited Changi from May 1
Today: 2 staff, 6 contacts
To date (68): 37 staff, 25 contacts, 5 visitors, 1 phylogenetically linked
Among staff (92% aviation workers are vaccinated): 26 vax'd, 11 not vax'd (efficacy: ~79%)
PSA: Please get tested if you had visited Changi from May 1



[Mystery case solved]
Case 62998 (staff at Lendlease Pte Ltd) is now linked to Changi T3 cluster through WGS and phylogenetic analysis. Epidemiological investigations are still ongoing to determine how the cases are linked.
Case 62998 (staff at Lendlease Pte Ltd) is now linked to Changi T3 cluster through WGS and phylogenetic analysis. Epidemiological investigations are still ongoing to determine how the cases are linked.

Daily average of unlinked community cases in the past week as of May 15: 2.29.
Entering #NoDineIn period now... stay home and stay safe, folks!
Entering #NoDineIn period now... stay home and stay safe, folks!

Schools and tuition centres attended by student cases in May 2021 wave.
Several schools and tuition centres still TBC by MOH (probably in today's press release):
- St Margaret's Primary
- Yu Neng Primary
- The Learning Lab United Square
- HCL Katong
google.com/maps/d/edit?hl…
Several schools and tuition centres still TBC by MOH (probably in today's press release):
- St Margaret's Primary
- Yu Neng Primary
- The Learning Lab United Square
- HCL Katong
google.com/maps/d/edit?hl…

• • •
Missing some Tweet in this thread? You can try to
force a refresh