#AKIConsultSeries
👴 w Advanced Cirrhosis, hemorrhagic portal hypertension and hx of a heart block (w pacemaker).
Came to the ED w diarrhea 2/2 severe C. Diff.
Now in shock...
Initial resus with Norepinephrine 0.3 ug/kg/min, Crystalloid and albumin. Cr 3.8
1/7
👴 w Advanced Cirrhosis, hemorrhagic portal hypertension and hx of a heart block (w pacemaker).
Came to the ED w diarrhea 2/2 severe C. Diff.
Now in shock...
Initial resus with Norepinephrine 0.3 ug/kg/min, Crystalloid and albumin. Cr 3.8
1/7
18 hrs later, no renal improvement + oliguria.
MABP 70, CRT 2 seconds. 🧠 confused, + asterixis. No ascites or edema
Workup: hemodynamic AKI (⬆️SG, ⬇️UNa, ⬆️BUN/Cr, bland sediment)
Team wants to continue fluids, albumin and antibiotics... Dr. Harris, do you concur?
2/7
MABP 70, CRT 2 seconds. 🧠 confused, + asterixis. No ascites or edema
Workup: hemodynamic AKI (⬆️SG, ⬇️UNa, ⬆️BUN/Cr, bland sediment)
Team wants to continue fluids, albumin and antibiotics... Dr. Harris, do you concur?
2/7
Obviously you are here for the #POCUS so here we go:
IVC: Plethoric (No subX window 2/2 intestinal air)
LV, RV: Relatively preserved systolic fx
Pacemaker lead seen causing important Tricuspid Regurgitation!
3/7
IVC: Plethoric (No subX window 2/2 intestinal air)
LV, RV: Relatively preserved systolic fx
Pacemaker lead seen causing important Tricuspid Regurgitation!
3/7
LVOT-VTI = 21 (Normal stroke volume)
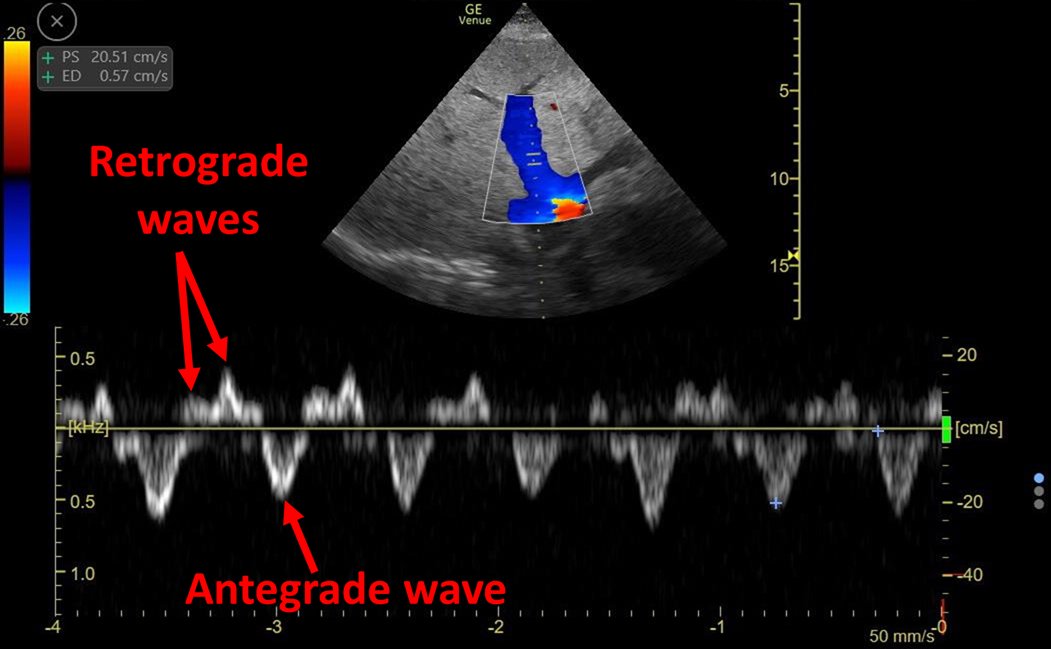
Hepatic Vein = S reversal (severe TR)
Portal Vein = Pt had portal vein thrombosis. No flow seen
Intra-Renal Vein Doppler (IRVD) = Monophasic "D" only
#VExUS = 3
TRVmax = 3.53 m/s (high probability PH)
4/7
Hepatic Vein = S reversal (severe TR)
Portal Vein = Pt had portal vein thrombosis. No flow seen
Intra-Renal Vein Doppler (IRVD) = Monophasic "D" only
#VExUS = 3
TRVmax = 3.53 m/s (high probability PH)
4/7




There is relatively preserved systolic fx
There is also venous congestion (Plethoric IVC)
But #VExUS tells me more: It tells me congestion is severe enough to be transmitted to the kidney!
There is a high chance this is congestive AKI!
(AKA intra-capsular tamponade)
5/7
There is also venous congestion (Plethoric IVC)
But #VExUS tells me more: It tells me congestion is severe enough to be transmitted to the kidney!
There is a high chance this is congestive AKI!
(AKA intra-capsular tamponade)
5/7
I recommended stopping albumin and fluids. Multi-agent diuresis (High dose Furosemide + Spironolactone) and continue Vasopressor
It worked! Pt had excellent urine output, negative fluid balance and 3 days later Cr returned to baseline 0.9 mg/dl 😎
6/7
It worked! Pt had excellent urine output, negative fluid balance and 3 days later Cr returned to baseline 0.9 mg/dl 😎
6/7
Low kidney perfusion in Cirrhosis can be 2/2 hipovolemia, vasodilation, abdominal hypertension, congestion, low CO....
Are you seriously going to keep calling all of these "low effective arterial blood volume"?
Dominate hemodynamics, #POCUS Always!
END/
Are you seriously going to keep calling all of these "low effective arterial blood volume"?
Dominate hemodynamics, #POCUS Always!
END/
• • •
Missing some Tweet in this thread? You can try to
force a refresh